
Abstract
Cerebral venous sinus thrombosis (CVT) is an uncommon yet serious condition. While CVT has many known precipitants and etiologies, hyperthyroidism as a precipitant of CVT is not well understood. This study reported a case of a 41-year-old male with a 4-year history of hyperthyroidism presented with seizure. Consequently, a diagnosis of superior sagittal sinus thrombosis was confirmed by computed tomography and magnetic resonance (MR) venograms. Extensive investigations yielded no apparent underlying cause, but laboratory findings were consistent with uncontrolled hyperthyroidism. The patient improved rapidly following anticoagulation. Follow-up MR and MRV scans 2 months after treatment revealed full recanalization of the superior sagittal sinus. This case report highlighted hyperthyroidism, as a procoagulant condition, resulting specifically in superior sagittal sinus thrombosis.
Keywords
Introduction
Cerebral venous thrombosis (CVT) is an uncommon condition with an incidence ranging between 0.22 and 1.57 per 100 000 annually. 1 The major risk factors of CVT in adults are prothrombotic conditions, oral contraceptives, pregnancy and puerperium, malignancy, infections, and head injury along with genetic thrombophilia including antithrombin deficiency, protein C or protein S deficiency, factor V Leiden mutation, and hyperhomocysteinemia.2,3
Coagulation disturbances are reported in patients with hyperthyroidism. 4 However, the link between hyperthyroidism and CVT is not clearly understood despite an emerging number of case reports linking both conditions. We report a case of a young male, without clear acquired or genetic thrombotic risk factors, who was diagnosed with superior sagittal sinus thrombosis (SSST) and concomitantly had uncontrolled hyperthyroidism. This case report highlighted hyperthyroidism as a precipitant factor of CVT (SSST specifically).
Case Presentation
A 41-year-old gentleman with a 4-year history of hyperthyroidism presented to the emergency department with an episode of generalized tonic colonic seizure, self-terminated within 5 minutes. The patient denied history of previous seizures. There was no fever, headache, or weakness. No history of recent infection or trauma. Regarding his hyperthyroidism, he was started on carbimazole on diagnosis. However, during the last 3 years, the patient discontinued his medication, and he was lost to follow-up. He had no past medical history of coagulation or bleeding abnormalities. He does not smoke or consume alcohol.
On physical examination, he was afebrile, tachycardic (100-110 beats per minute), alert, and oriented. No focal neurological deficit was detected. Neck examination revealed a mild goiter, but no audible bruit. Electrocardiography showed sinus tachycardia. Laboratory studies revealed normal white blood cell count and C-reactive protein, and normal basic electrolytes. Lactic acid was 1.6 mmol/L (0.5-2.2 mmol/L). Thyroid function test showed thyroid-stimulating hormone <0.01 mLU/L (0.30-4.20 mLU/L), FT4 73 mLU/L (11.6-21.9 mLU/L), and FT3 29 mLU/L (3.7-6.4 mLU/L). Antithyroid peroxidase level was 293 IU/mL (0-35 IU/mL). Neck ultrasound showed mildly enlarged thyroid gland with diffuse heterogeneous echotexture suggestive of chronic thyroiditis. Head noncontrast computed tomography (CT) scan displayed increased attenuation along the anterosuperior aspect of the superior sagittal sinus and adjacent cortical veins bilaterally (Figure 1) suggesting focal superior sagittal sinus and adjacent cortical veins thrombosis. This was confirmed by CT and magnetic resonance (MR) venograms (Figure 2). Coagulation profile showed normal PT/PTT/INR (prothrombin time/partial thromboplastin time/international normalized ratio) and elevated D-dimer. IgM (immunoglobulin M) and IgG anticardiolipin antibodies and lupus anticoagulant were negative. Prothrombin c.*97G>A variant and 161G>A mutation for Factor V Leiden were not detected. Antithrombin activity was normal (80%). Protein C and protein S were normal. Homocysteine level was 12 µmol/L (0-12 µmol/L). He had low vitamin B12 level, 124 pmol/L (145-596 pmol/L). He was started on therapeutic dose of enoxaparin and carbimazole, 15 mg BID (twice daily). He was discharged on dabigatran 150 mg BID and vitamin B12 replacement.

Noncontrast computed tomography (CT) scan axial (A), coronal (B) and sagittal (C) planes displaying increased attenuation along the anterosuperior aspect of the superior sagittal sinus (orange arrows) and adjacent cortical veins bilaterally (green arrows) suggesting focal superior sagittal sinus and adjacent cortical veins thrombosis.
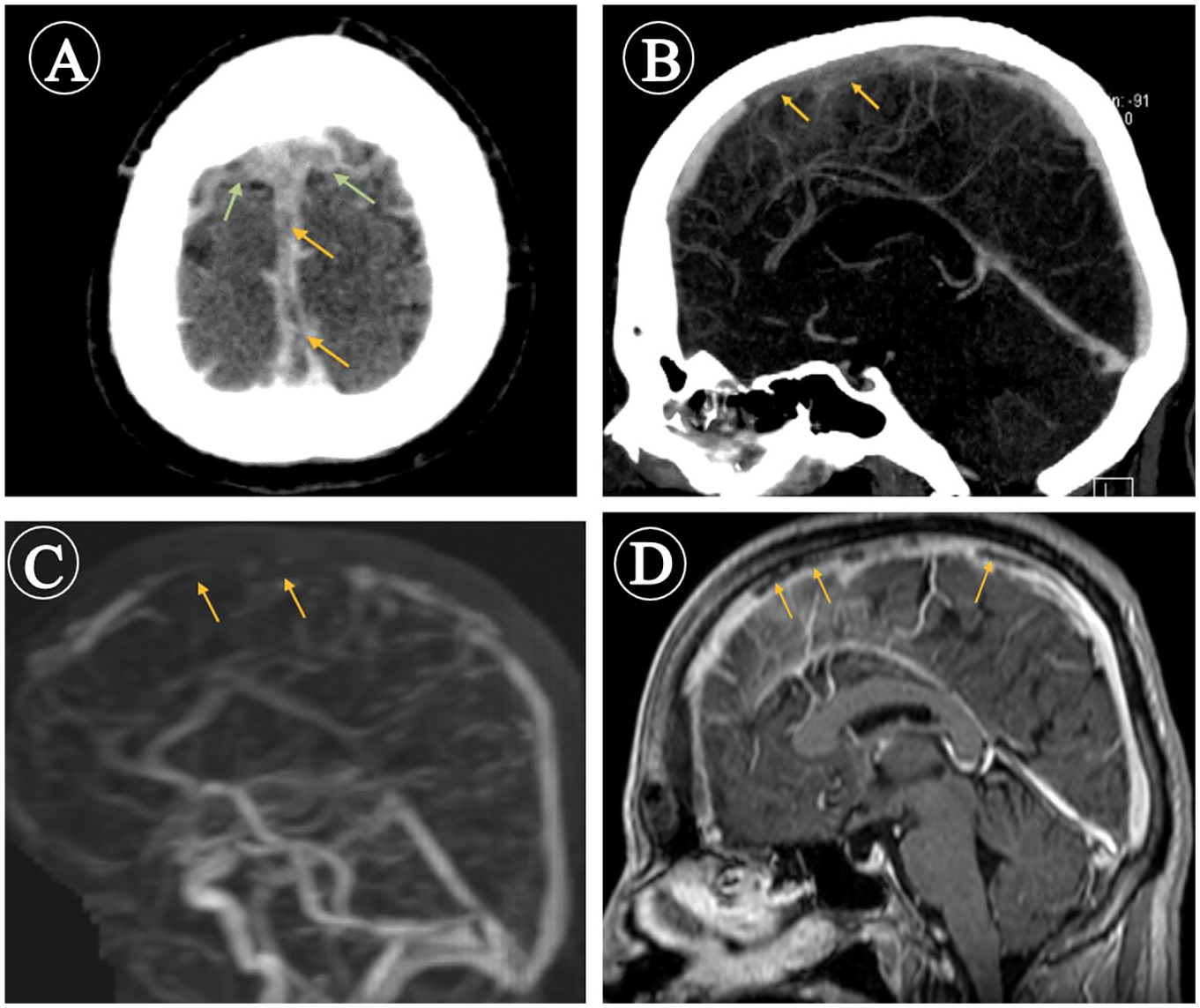
Computed tomography (CT) and magnetic resonance (MR) venogram scans. CT venogram axial (A) and sagittal (B) planes showing nonopacification of the anterosuperior aspect of the superior sagittal sinus (orange arrows) and adjacent cortical veins (green arrows) confirming their thrombosis. MR venogram (C) and MR sagittal (D) T1W-Fat sat postcontrast demonstrate filling defects within the anterosuperior aspect of the superior sagittal sinus (orange arrows).
Two months later, follow-up MR and MRV demonstrated evidence of recanalization of the previously noted thrombosed portion of the superior sagittal sinus and adjacent cortical veins (Figure 3). Moreover, a follow-up thyroid function test turned out to be normal.
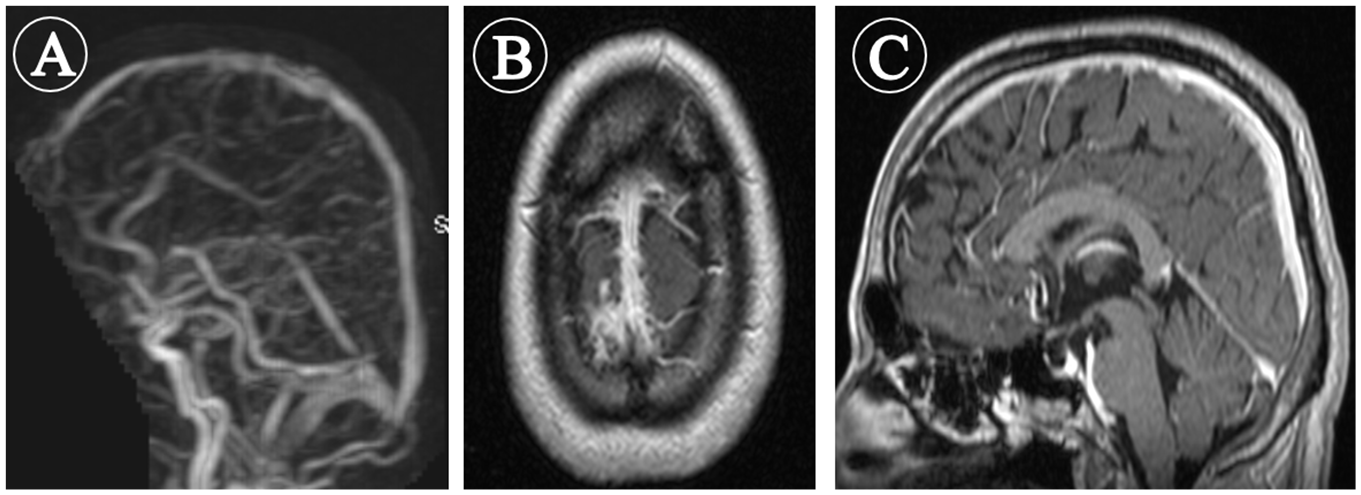
Follow-up magnetic resonance (MR) venogram (A) MR axial (B) and sagittal (C) T1W-Fat sat postcontrast images demonstrate recanalization of the superior sagittal sinus and the adjacent cortical veins with no sizeable filling defects.
Discussion
CVT is an uncommon multifactorial condition with up to 25% of cases being considered as idiopathic. 5 Thyrotoxicosis as a cause of CVT was first described by Kaliebe 6 in 1913. Since then, an emerging number of reports have linked CVT with hyperthyroidism.7 -12 To the best of our knowledge, this the first report in the Middle East demonstrating the association between CVT and hyperthyroidism. On a through literature review, we have noticed, as in our case, that the superior sagittal sinus was the most common site of hyperthyroidism-related CVT. A systemic review done by Bensalah et al 8 in 2011 showed that SSST was involved in 18 out of 26 cases (69%) of hyperthyroidism-related CVT. Imai et al 10 and Yokoyama et al 11 also reported hyperthyroidism-related SSST in 2018 and 2019, respectively.
As in any thrombosis, CVT development is related to Virchow’s triad of hypercoagulability, vessel wall injury, and venous stasis. 13 Hypercoagulable and hypofibrinolytic states are reported in hyperthyroidism; in a meta-analysis of 51 studies assessing the effect of high thyroid hormone levels (exogenous or endogenous) on coagulation system, high thyroid hormone levels were associated with a rise in factors VIII, IX, Von Willebrand factor, and fibrinogen. 4 Additionally, hyperthyroidism has been reported to cause an increase in factor X. 14 On the other hand, hypofibrinolysis in hyperthyroidism is suggested to be caused by a reduction of plasmin and plasmin activator, as well as an elevation of plasminogen activator inhibitor-1, 2-antiplasmin, and thrombin activatable fibrinolysis inhibitor.4,14 There is evidence suggesting that the procoagulant effect seen in hyperthyroidism is meditated through the thyroid hormone receptor beta gene (THRB), as, in contrast to patients with hyperthyroidism, patients with resistance to thyroid hormone, who have defective THRB, did not show an increased risk of hypercoagulability despite having high levels of thyroid hormone. 15 As Graves’ disease is the most common cause of hyperthyroidism, 16 this could raise an assumption that attributes hypercoagulability and hypofibrinolysis to inflammatory or autoimmune mechanisms. However, administering exogenous doses of levothyroxine in healthy volunteers was also found to cause hypercoagulable and hypofibrinolytic states. 17
In our case, we investigated the possibility of known risk factors causing CVT, all of which were negative. Notably, the homocysteine level in our patient was in the upper normal range (12 µmol/L). There is evidence that suggests high homocysteine levels as a risk factor for thrombosis 18 ; Gowda et al 19 and Kanaya et al 20 have reported CVT in patients with high homocysteine levels (>50 µmol and 90 nmol, respectively) in the absence of other risk factors. However, this is unlikely in our patient as the homocysteine level was still within the normal range. Regarding the possibility of venous stasis, it has been reported that large goiters may contribute to cerebral venous stasis. 21 However, the neck ultrasound of our case showed a mild goiter. Moreover, there was no evidence of vessel wall injury as a cause of thrombosis.
Conclusion
We suggest that hyperthyroidism may precipitate CVT by causing hypercoagulability. Therefore, we recommend considering CVT in any patient with hyperthyroidism presenting with neurological symptoms. Likewise, important is considering thyroid function testing in CVT patients with no clear causes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Verbal informed consent was obtained from the patient for his anonymized information to be published in this article.