
Abstract
Oxyntic gland adenomas (OGAs) are benign gastric neoplasms composed of gland-forming epithelial cells with predominantly chief cell differentiation resembling oxyntic glands confined to the mucosa. If the tumor has submucosal invasion, it should be classified as gastric adenocarcinoma of fundic gland type. The OGAs can pose a diagnostic challenge, as they can resemble aggressive gastric neoplasms. There are no current guidelines on the management of OGA. Due to the relatively small size and low malignant potential, these lesions are typically managed endoscopically. In this case, we are reporting a 22-year-old woman who was diagnosed with OGA during evaluation of iron deficiency anemia and underwent successful endoscopic resection.
Keywords
Introduction
Oxyntic gland adenomas (OGAs) are benign gastric neoplasms composed of gland-forming epithelial cells with predominantly chief cell differentiation resembling oxyntic glands. These neoplasms are typically asymptomatic and are often discovered incidentally. While the exact incidence of OGAs is not known, they are thought to be quite rare. Despite their benign nature, OGAs can pose a diagnostic challenge, as they can resemble aggressive gastric neoplasms. In this case report, we describe a patient who was incidentally diagnosed with OGA during evaluation of iron deficiency anemia (IDA) and underwent successful endoscopic removal. This report will shed light on the unique clinical presentation, endoscopic characteristics, and management strategies of OGA, as well as highlight the youngest case reported in the literature thus far.
Case Description
We are presenting a 22-year-old woman with IDA. Patient denied menorrhagia or family history of gastrointestinal malignancy. She denied dysphagia, odynophagia, heartburn, nausea, vomiting, abdominal pain, altered bowel habits, melena, hematochezia, and unintentional weight loss. Vitals signs were normal. Physical examination was unrevealing with the exception of mild conjunctival pallor. Laboratory data: hemoglobin 11.5 g/dL, transferrin saturation 12.8%, ferritin 200 ng/mL, and iron 76 mcg/dL.
Despite the normal ferritin level, the low transferrin saturation <20% was in favor of iron deficiency and the patient underwent esophagogastroduodenoscopy (EGD) and colonoscopy at a different institution for evaluation of IDA. A 7-mm fundic lesion was identified during EGD; the lesion was biopsied and 2 hemostatic clips were placed due to oozing at the biopsy site (Image 1). Biopsy of the gastric lesion demonstrated well-circumscribed proliferation of chief cells arranged in small, tight tubules, consistent with an OGA. Of note, duodenal biopsies did not show features of celiac disease, and ileocolonoscopy did not identify any bleeding source. Following the identification of the OGA, the patient was referred for endoscopic removal. Patient underwent repeat EGD and endoscopic resection was performed successfully. The excised specimen was consistent with the known diagnosis of OGA (Image 2). Given the absence of menorrhagia and negative bidirectional endoscopy, the patient was advised to follow up at the gastroenterology clinic and discuss video capsule endoscopy to exclude small intestinal causes of anemia. Patient underwent repeat EGD after 3 months, and no evidence of recurrence of the OGA was found.
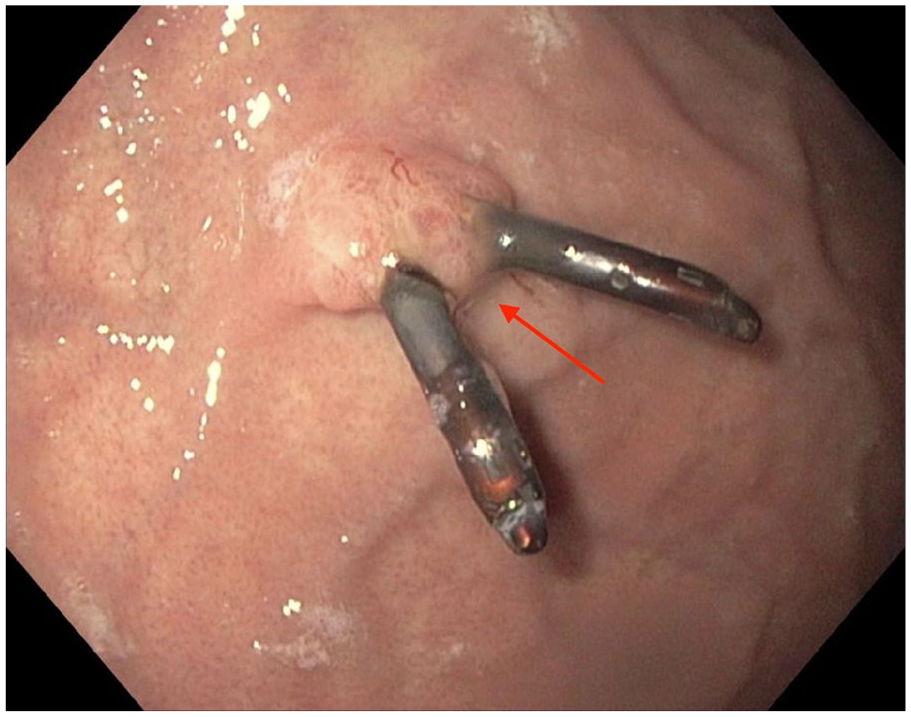
EGD image showing oxyntic gland adenoma with previously placed hemostatic clips (red arrow).

Histopathology image showing well-circumscribed proliferation of chief cells arranged in small, tight tubules.
Discussion
Gastric adenomas represent only 1% to 10% of gastric polyps and the subtypes include intestinal type, foveolar type, pyloric gland type, and oxyntic gland type. Of the subtypes, intestinal-type adenomas and foveolar-type adenomas are more common, representing 56% and 41% of gastric adenomas, respectively. 1 The prevalence of OGA has not been well established. A single-center study of 7488 patients conducted in Japan yielded a disease frequency of 0.36% which was higher than the previous reports of 0.01%. 2 The authors attributed the higher frequency to the increased awareness and experience needed to make an accurate diagnosis.
OGA is a relatively newly described entity and the nomenclature has been updated with the evolving understanding of the disease process. In 2007, Tsukamoto et al 3 reported the first case of gastric adenocarcinoma with chief cell differentiation (GA-CCD) which comprised well-differentiated tubular adenocarcinoma with shared characteristics of chief cells and mucous neck cells. Subsequently in 2010, Ueyama et al compared GA-CCD with adenocarcinomas of differentiated type and found that GA-CCD was less aggressive with mild atypism, low proliferative potential, and without p53 overexpression, lymphovascular invasion, and recurrence. Based on these clinicopathological findings, the authors proposed the new term called gastric adenocarcinoma of fundic gland type (GA-FG), chief cell predominant type. 4 In 2012, Singhi et al 5 proposed the reclassification of GA-CCD, as “oxyntic gland polyp/adenoma.”
The 2019 World Health Organization (WHO) classification (5th edition) defined OGA as a benign epithelial neoplasm confined to the mucosa. 6 If submucosal involvement is identified, the tumor should be classified as GA-FG subtype. The OGAs are composed of well-differentiated columnar cells which differentiate into parietal cells, chief cells, or both. The tumor cells have pale basophilic cytoplasm and mild nuclear atypia, resembling oxyntic glands (mainly chief cells). Oxyntic gland differentiation can be established by immunohistochemistry, such as pepsinogen I (for chief cells) and H+ K+ ATPase (for parietal cells). In our patient, the resected lesion demonstrated proliferation of chief cells without submucosal invasion, compatible with the diagnosis of OGA.
The OGAs are typically diagnosed incidentally, with the average age of diagnosis ranging between 60 and 70 years. 6 Prior to our case, the youngest patient found to have OGA in the literature was 41 years old. 7 Our case highlights the youngest patient found to have OGA to date, at 22 years of age. The OGAs are polypoid, submucosal tumors, or flat lesions with faded whitish mucosa with vasodilation or branched vessels on the tumor surface. 6 In a retrospective study of 136 subjects, Iwamuro et al 8 compared the characteristics of GA-FG and OGA and found that larger lesion size (>5 mm), elevated tumor morphology, and no or closed-type atrophy in the background gastric mucosa were endoscopic features of GA-FG.
There are no current guidelines on the management of OGA. Due to the relatively small size and low malignant potential, these lesions are typically managed endoscopically. In a retrospective study of 116 patients with 126 lesions (OGA or GA-FG), 114 lesions were removed by endoscopic mucosal resection or endoscopic submucosal dissection. None of the resected lesions had positive vertical margins and during a median follow-up of 14.5 months, there were zero deaths attributed to OGA or GA-FG. 9 This study recognizes endoscopic resection as a suitable treatment option for OGA.
Conclusion
Our case highlights the importance of differentiating OGAs from GA-FG and the application of endoscopy as an effective treatment option. The successful endoscopic resection and absence of recurrence during follow-up align with existing literature, affirming endoscopic intervention as a viable and effective management strategy for OGAs. However, the rarity of OGAs and the absence of standardized guidelines emphasize the necessity for continued research to establish definitive management protocols and elucidate the natural history of this condition comprehensively. Furthermore, the recognition of OGA at a notably young age expands our understanding of its potential occurrence in diverse age groups, urging clinicians to maintain a broad differential diagnosis for similar presentations.
Footnotes
Authors’ Note
Abstract was presented as a poster at the American College of Gastroenterology Conference, October 2023.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institutions do not require ethical approval for reporting individual cases or case series.
Informed Consent
Verbal informed consent was obtained from the patient for the anonymized information to be published in this article.