
Abstract
Kikuchi-Fujimoto disease (KFD) is a benign and self-limited disorder that usually presents with regional cervical lymphadenopathy and fever. We report a case of a 12-year-old female who complained of fever, night sweating, significant weight loss, and tender right cervical lymph node enlargement for 2 months. A full workup including laboratory tests and imaging studies, an excisional biopsy, and histopathological analysis were done, and the diagnosis of KFD was confirmed. The patient was treated with analgesia and oral prednisolone, resulting in good improvement. A high degree of clinical suspicion is imperative for physicians, given the rarity of the disease and the associated diagnostic challenges.
Keywords
Introduction
Kikuchi-Fujimoto disease (KFD) is a benign and self-limited condition initially reported independently by Kikuchi and Fujimoto in 1972. It is characterized by lymphadenitis with abundant karyorrhectic debris and focal proliferation of histiocytic cells, which is why it is also referred to as histiocytic necrotizing lymphadenitis. 1 The typical age of onset is under 30 years, and there is a notable female predominance, with a female-to-male ratio as high as 4:1. Although increasingly recognized in the literature, the actual prevalence of KFD remains unknown. 2
Kikuchi-Fujimoto disease commonly manifests with localized lymphadenopathy, predominantly unilateral in the cervical region, accompanied by fever, skin rashes, and headaches. 3 It has been recognized as a potential cause of fever of unknown origin. 4 Additional symptoms, albeit less frequent, include chills, night sweats, arthralgia, and weight loss. 5 The etiology of KFD remains idiopathic, although some studies propose associations with viral infections such as COVID-19 and Epstein-Barr virus (EBV), or an autoimmune mechanism, given its link to systemic lupus erythematosus (SLE). 6 Furthermore, KFD may precede, coexist with, or follow SLE. Due to its potential to mimic conditions like lymphoma or SLE, histopathological examination is crucial for definitive diagnosis.2,7
Herein, we present the case of a 12-year-old female patient with prolonged fever, cervical lymphadenopathy, and systemic symptoms, ultimately diagnosed with KFD by lymph node biopsy. The patient demonstrated significant improvement with corticosteroid therapy.
Case Presentation
A 12-year-old female patient presented with a persistent daily fever of 40°C over a 30 day period. Previous treatment with antibiotics and antipyretics, administered a month ago for pharyngitis associated with an enlarged right cervical lymph node, yielded no significant improvement. The patient exhibited ongoing right cervical lymph node enlargement, notable weight loss (10 kg within 1 month), night sweats, frequent vomiting (up to 6 times daily), and frontal headache without specific diurnal correlation. Absence of cough, dyspnea, skin rash, or abnormal movements was reported. The patient had no history of allergy, recent travel, exposure to cat bites or scratches, or contact with individuals diagnosed with tuberculosis.
Upon examination, the patient appeared reasonably well, active, and oriented to time, place, and person. Mild dehydration was noted, with an absence of dysmorphic features, jaundice, or cyanosis. Vital signs were as follows: a temperature of 39°C, respiratory rate of 17 breaths per minute, blood pressure 112/75 mm Hg, and a heart rate of 96 beats per minute. Multiple enlarged and tender lymph nodes, predominantly located in the right cervical region with a maximum size of 4 cm × 2 cm, were observed, with no noticeable changes in the overlying skin. Head, Eyes, Ears, Nose, and Throat (HEENT) examination was done to rule out reactive lymphadenopathy and yielded no significant findings. Examination of the cardiovascular and respiratory systems was unremarkable. The abdomen was soft and nontender without organomegaly. Notably, examination of the extremities revealed bilaterally tender, warm, and edematous hands, coupled with bilateral knee pain and normal skin overlaying these areas.
Lumbar puncture (LP) was done due to the presence of fever, vomiting, and headache. The results indicated white blood cells (WBCs) at 50/μL, protein at 25.6 g/dL, lymphocytes at 60, neutrophils at 40, and glucose at 67 mg/dL, with no growth observed in culture. The diagnosis of aseptic meningitis was established and managed with supportive therapy and intravenous acyclovir for 4 days with improvement. Additional laboratory tests performed are summarized in Tables 1 and 2. Imaging studies, including targeted ultrasonography of the right cervical lymph node and a contrast-enhanced computed tomography (CT) scan of the abdomen and pelvis, revealed multiple lymph node enlargements up to 3 cm × 2 cm, some of which displayed necrotic features. However, the CT scan did not reveal any additional significant abnormalities.
Laboratory Results of the Patient.

Abbreviations: Hb, hemoglobin; MCV, mean corpuscular volume; PLTS, platelets; WBCs, white blood cells; TLC, total lymphocyte count; RBC, red blood cell; ESR, erythrocyte sedimentation rate; CRP, c-reactive protein; SGPT, serum glutamate pyruvate transaminase; SGOT, serum glutamic-oxaloacetic transaminase; BUN, blood urea nitrogen; LDH, lactate dehydrogenase.
Additional Laboratory Investigations of the Patient.
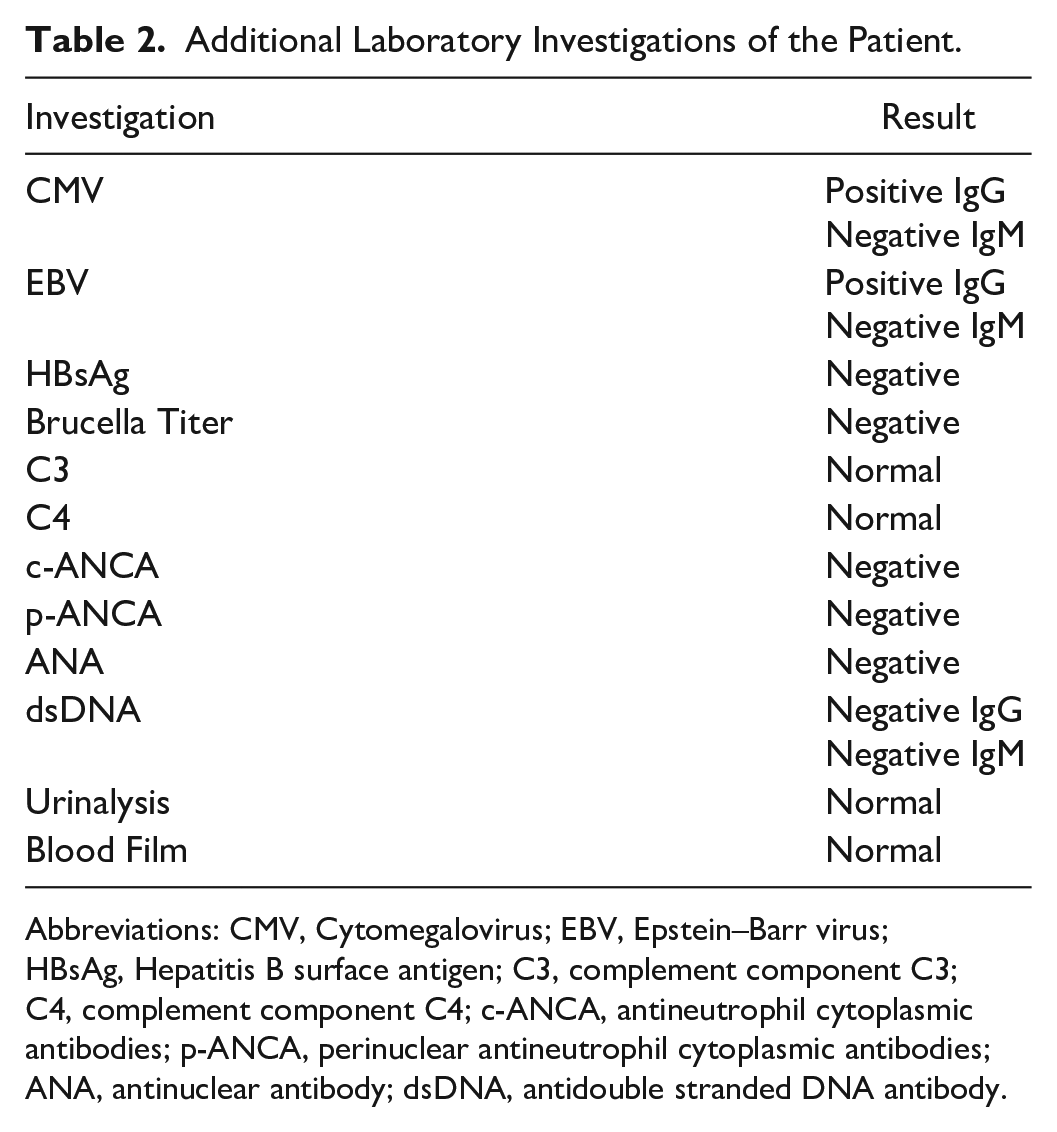
Abbreviations: CMV, Cytomegalovirus; EBV, Epstein–Barr virus; HBsAg, Hepatitis B surface antigen; C3, complement component C3; C4, complement component C4; c-ANCA, antineutrophil cytoplasmic antibodies; p-ANCA, perinuclear antineutrophil cytoplasmic antibodies; ANA, antinuclear antibody; dsDNA, antidouble stranded DNA antibody.
Subsequent to the persistence of vomiting even after the resolution of meningitis, an endoscopy was done and revealed prolapsed cardiac gastropathy. Biopsies obtained from the stomach body and antrum demonstrated the growth of Helicobacter pylori, prompting the initiation of triple therapy. An excisional biopsy of the right cervical lymph node was performed, confirming the diagnosis of KFD (Figure 1).

Excisional biopsy of the right cervical lymph node (Kikuchi lymphadenitis). (A) Section revealed lymph node with distorted architecture by irregular areas of paracortical necrosis (arrow) (H&E, 4×). (B) These areas show a zone of central necrosis surrounded by pale zone of mononuclear cells (H&E, 10×). (C) The mononuclear cells are composed of lymphocytes, histiocytes, and plasmacytoid cells with no neutrophils. Frequent apoptosis and abundant karyorrhectic debris are noted (arrow) (H&E, 40×). (D) CD3 immunostaining revealed predominant reactive T lymphocytes. (E) CD68 immunostaining revealed increased histiocytes with many crescentic forms. (F) CD20 highlights scattered reactive B lymphocytes.
Consequently, the patient was initiated on oral prednisolone 1 mg/kg/day, along with oral paracetamol for a duration of 5 days. This resulted in progressive clinical and laboratory improvement. Subsequently, the patient was discharged in a good health condition and underwent regular follow-up at the pediatric rheumatology clinic, with a gradual tapering of corticosteroid treatment.
Discussion
Necrotizing lymphadenitis represents a category of infective and inflammatory disorders distinguished by inflammatory infiltrates comprising varying cell types, including plasma cells, histiocytes, and neutrophils, alongside nongranulomatous, noncaseating necrosis within the lymph nodes. Among these conditions, KFD, acute EBV infection, and SLE stand out as the most prevalent. Kikuchi disease, in particular, is the most common, accounting for 62.2% of cases, followed by EBV and lupus lymphadenitis.8,9 In addition, mycobacterial infections such as tuberculosis and Hodgkin’s lymphoma can induce lymph node necrosis, albeit characterized by distinct morphological and histological features. 8
Although the precise pathophysiology of KFD remains incompletely elucidated, current theories invoke both infectious and autoimmune mechanisms. 10 The infectious hypothesis, particularly viral etiologies, gains prominence from the observed presence of histiocytic and cytotoxic T lymphocytes in KFD-affected lymph nodes. 10 Viruses implicated include human Herpes simplex viruses (HHVs) 1, 2, 6, 7, 8, parvovirus B19, human immunodeficiency virus (HIV), and COVID-19.11,12 Numerous documented cases have demonstrated an association between KFD and SLE, whether concurrent, preceding, or succeeding SLE diagnosis. This led to the consideration of an autoimmune mechanism in the pathogenesis of KFD.13-15 Moreover, rare autoimmune disorders like Sjögren syndrome, thyroiditis, and leukocytoclastic vasculitis have been found to be associated with KFD. 11
Kikuchi-Fujimoto disease often presents with a variable array of nonspecific symptoms, including weight loss, fatigue, night sweats, skin rash, arthritis, arthralgia, and myalgia. Fever and lymphadenopathy constitute the primary clinical manifestations of KFD. 16 Our patient exhibited all these characteristic symptoms, with the exception of a skin rash. The principal differential diagnoses for KFD encompass SLE, lymphoma, toxoplasmosis, Bartonella henselae (cat scratch disease), HIV, and EBV, all of which were ruled out in our case. 17
Given the ambiguous presentation of KFD, a conclusive diagnosis cannot be solely established through history, physical examination, and laboratory analyses. The primary diagnostic modality involves an excisional lymph node biopsy, coupled with histopathological analysis, typically revealing crescent-shaped histiocytes, karyorrhectic debris, and paracortical necrosis.8,18 The lymph node biopsy in our case corroborated these characteristic findings.
Kikuchi-Fujimoto disease is inherently self-limiting, and initial management often revolves around supportive care utilizing antipyretics and analgesics. However, patients with persistent symptoms have demonstrated positive responses to corticosteroid therapy, 11 as exemplified in our case, where the patient was discharged following a 1-week course of paracetamol and prednisolone treatment. An alternative or adjunct to corticosteroids is hydroxychloroquine; nevertheless, its potential for retinopathy in prolonged usage mandates baseline eye examinations shortly after initiation and subsequent evaluations every 5 years.19,20 To prevent misdiagnosis and inappropriate treatment of KFD, a comprehensive diagnostic strategy that integrates clinical presentation, imaging studies, laboratory tests, and histopathology is essential.
Conclusions
In summary, Kikuchi-Fujimoto is a rare, benign, self-limiting disease that primarily affects young people and presents with fever, maculopapular rash, and persistent cervical lymphadenopathy that does not improve with antibiotics. Further research is required for a better understanding of the pathophysiology.
The prognosis for KFD is generally favorable, yet vigilant follow-up is recommended due to the potential for recurrence and the risk of SLE development. Physicians should routinely consider this disease in the differential diagnosis for patients presenting with persistent lymphadenopathy or lymphadenitis, emphasizing the importance of a lymph node biopsy to establish a definitive diagnosis. The potential for misdiagnosis persists, particularly given the histopathological similarities with other necrotizing lymphadenitis disorders, notably lymphoma. Consequently, consultation with a hematopathologist is strongly recommended to ensure precise diagnostic interpretation.
Footnotes
Acknowledgements
The authors express their gratitude to the patient and their family for their great contribution.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
This case report did not require review by the Ethics Committee.
Informed Consent
Written informed consent was obtained from a legally authorized representative for anonymized patient information to be published in this article.