
Abstract
Kikuchi-Fujimoto disease is an uncommon lymphohistiocytic disorder that frequently presents with acute or subacute clinical disease course. Cervical lymphadenopathy is the most common involved lymph node. Very rare cases of pathologic diagnosis of Kikuchi-Fujimoto disease with bilateral pleural effusion and multiple mediastinal lymphadenopathies have been reported in the literature. In this article, we report the case of a 60-year-old male presented with bilateral pleural effusion and multiple mediastinal lymphadenopathies. He received video-assisted thoracoscopic surgery of the right pleura and thoracoscopic excision of the mediastinal lymph node. The pathologic findings from the lymph node and pleura were compatible with Kikuchi-Fujimoto disease. He was treated with oral hydroxychloroquine and oral prednisolone. A computed tomography scan of the chest 4 months later showed regressive mediastinal lymphadenopathy and bilateral pleural effusion. Our case is a first reported case of Kikuchi-Fujimoto disease diagnosis by the pathology of the lymph node and pleura in the literature. Results from our case suggest that Kikuchi-Fujimoto disease should be included in the differential diagnosis of bilateral pleural effusion and multiple mediastinal lymphadenopathies.
Introduction
Kikuchi-Fujimoto disease (KFD) is a rare lymphohistiocytic disorder first described in 1972 that is most often diagnosed in young Asian women.1,2 KFD is frequently presented with acute or subacute clinical disease course. Cervical lymphadenopathy is the most common involved lymph node. The differential diagnosis of KFD includes systemic lupus erythematosus, herpes simplex–associated lymphadenopathy, non-Hodgkin lymphoma, plasmacytoid T-cell leukemia, nodal colonization by acute myeloid leukemia, metastatic adenocarcinoma, and infectious lymphadenitis. 3 Many studies have shown autoimmune disorders, ranging from systemic lupus erythematosus, rheumatoid arthritis, polymyositis, scleroderma, uveitis, and thyroiditis, which are associated with KFD.4 -6 Autoimmune disorders are diagnosed previously, simultaneously, or after KFD, especially systemic lupus erythematosus.7 -10 KFD is important to diagnose early. The clinicians and pathologists are essential for accurate diagnosis, and to avoid laborious investigation and inappropriate treatment. KFD is not ordinarily included in the differential diagnosis of bilateral pleural effusion and multiple mediastinal lymphadenopathy. We report a case of a 60-year-old male with bilateral pleural effusion and multiple mediastinal lymphadenopathies due to KFD. The diagnosis was confirmed by biopsy of the lymph node and pleura.
Case Report
The patient, a 60-year-old male, had a fever and cough beginning January 1, 2018. A computed tomography (CT) scan of his chest 3 days later (January 4, 2018) revealed bilateral pleural effusion and multiple mediastinal lymphadenopathies (Figure 1). Laboratory studies showed the following results: hemoglobin, 9.3 g/dL; leukocytes, 4020/µL with lymphopenia (522/µL); platelets, 147 × 103/µL; and C-reactive protein, 16.0 mg/dL. Serum biochemistry findings revealed impaired liver function: aspartate aminotransferase 124 IU/L; alanine aminotransferase 122 IU/L, alkaline phosphatase 232 IU/L; lactate dehydrogenase 368 IU/L; and gamma-glutamyltranspeptidase 219 IU/L. Antinuclear antibody and rheumatoid factor were negative. Pleural fluid showed numerous red blood cells; white blood cells, 1107; polymorphonuclear leukocytes, 68%; and lymphocytes, 16%. Results of all pleural fluid cultures were negative.

Computed tomography scan of chest showed bilateral pleural effusion and multiple mediastinal lymphadenopathy (arrow).
The patient was treated with decortication via video-assisted thoracoscopic surgery of the right pleura and thoracoscopic excision of the mediastinal lymph node. Pathologic studies of the mediastinal lymph nodes showed follicular lymphoid hyperplasia and focal, circumscribed, paracortical necrotizing lesions composed of abundant karyorrhectic debris, scattered fibrin deposits, and a collection of large mononuclear cells (Figure 2). Immunohistochemically, the large mononuclear cells were positive for myeloperoxidase. The overall histopathology indicated a necrotizing adenitis process and was compatible with Kikuchi`s lymphadenitis (Figure 3).
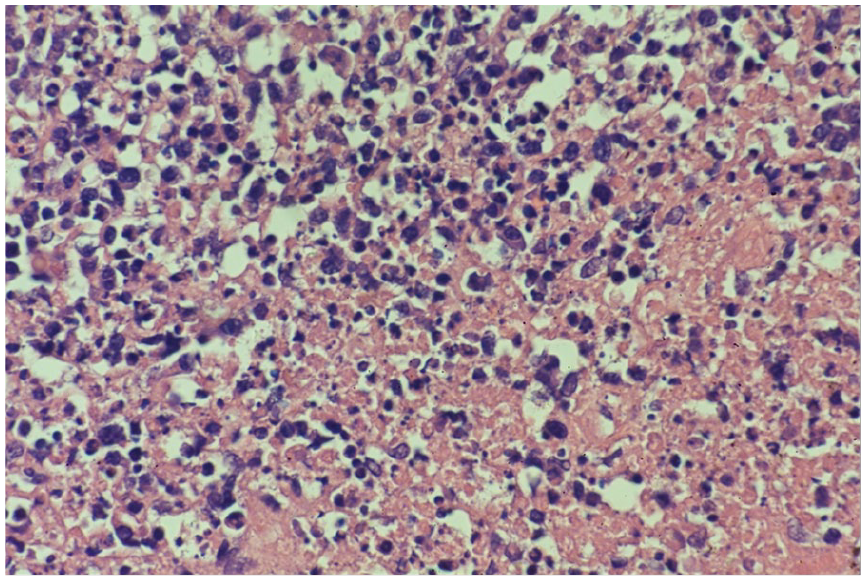
Follicular lymphoid hyperplasia and focal, circumscribed, paracortical necrotizing lesions, composed of abundant karyorrhectic debris, scattered fibrin deposits, and collection of large mononuclear cells (lymph node × 600).

Immunohistochemically, the large mononuclear cells are positive for myeloperoxidase (lymph node × 600).
Pathologic studies of the right pleura revealed necrotizing inflammation of the pleural tissue and some lymphoid tissue with necrotizing lesions, composed of abundant karyorrhectic debris with similar changes as in the mediastinal lymph nodes (Figure 4). The patient was treated with hydroxychloroquine, 200 mg orally once a day, and prednisolone, 5 mg orally twice a day, beginning January 22, 2018. CT of the chest on May 4, 2019, showed regressive mediastinum lymphadenopathy and bilateral pleural effusion (Figure 5). No recurrence of KFD was noted until October 2019.

Necrotizing inflammation of the pleural tissue and some lymphoid tissue with necrotizing lesions, composed of abundant karyorrhectic debris (pleura × 600).

Computed tomography scan of chest on May 2019, which showed regressive mediastinum lymphadenopathy and bilateral pleural effusion.
Discussion
Dumas’s review showed that the male-to-female ratio of KFD varies immensely, from 1:1 to 1:9. 11 The age distribution of KFD varies as well, but the mean age is analogous, between 25 and 30 years old. The classic symptoms of KFD are fever, headache, cough, weight loss, fatigue, arthralgia, myalgia, and night sweats, which are nonspecific for KFD. KFD patients frequently present with cervical lymphadenopathy. Deep sites of lymphadenopathy are mentioned in the literature, such as mediastinal lymphadenopathy, intraabdominal lymphadenopathy, hepatomegaly, and splenomegaly.12 -15 No specific laboratory test can be used to diagnose KFD. There are many nonspecific laboratory findings in KFD patients, such as leukopenia, lymphopenia, thrombocytopenia, and elevated alanine aminotransferase, an elevated erythrocyte sedimentation rate, elevated C-reactive protein, and elevated lactate dehydrogenase levels. Autoimmune disorders, especially systemic lupus erythematosus, are frequently reported in patients with KFD. Treatment guidelines for KFD was not well established in the literature. Most KFD patients were self-limited and observation is the most common management for KFD patients. The rate of spontaneous regression reported in the literature has varied from 61.5% to 95.0%. 11 However, patients with severe clinical courses may be treated with oral corticosteroids or hydroxychloroquine. The recurrence rate also varies, ranging from 0% to 21%. 11 Due to the risk of developing systemic lupus erythematosus, close long-term follow-up is recommended.
To our knowledge, only 3 cases of KFD with pleural effusion have been reported in the literature. Garcia-Zamalloa et al reported the case of a 32-year-old man admitted to the hospital with fever, malaise, and painful cervical lymphadenopathy. 16 The patient’s CT chest scan revealed generalized axillary, mediastinal, and hilar lymphadenopathy; interstitial infiltrates in both lungs; and bilateral pleural effusion. The diagnosis of KFD was made through a cervical lymph node biopsy. The patient was treated with oral prednisolone at a dosage of 1 mg/kg/day. After 2 years of follow-up, there was no evidence of recurrence. Tandon et al reported the case of a 19-year-old female who presented with a 1-month history of chest tightness. 17 CT scan of the chest showed mediastinal lymphadenopathy, a large pleural effusion, and enhancing left paraspinal soft tissue along the pleural surface. Thoracentesis produced lymphocytic, predominantly transudative fluid. Pleuroscopy revealed inflamed parietal pleura. Pleural biopsy revealed histiocytes and acute necrotizing lymphangitis. Steroids were started, and the patient showed symptomatic improvement within 48 hours. Liu et al reported the case of a 26-year-old woman who complained of unexplained fever, swelling of the cervical lymph node, and bilateral pleural effusion. Lymph node biopsy showed histiocytic necrotizing lymphadenitis. After treatment with glucocorticoids, the swelling of the lymph nodes disappeared, and the pleural effusion was reabsorbed. 18 Our patient with his severe clinical course was the oldest patient among the literature’s cases and the only case in which KFD was diagnosed through pathologic studies of the mediastinal lymph node and pleura. Our patient was treated with oral hydroxychloroquine and oral prednisolone. After 4 months of therapy, regression of lymphadenopathy and bilateral pleural effusion was noted, and there was no recurrence.
Conclusions With Learning Points
Kikuchi-Fujimoto disease is most commonly seen among younger females with cervical lymphadenopathy. Bilateral pleural effusion and multiple mediastinal lymphadenopathies is a very rare clinical manifestation of KFD.
Differential diagnosis of bilateral pleural effusion and multiple mediastinal lymphadenopathies should include KFD.
Footnotes
Acknowledgements
Chihen Tseng provided the histopathological figures and final approval of the version to be published. Chungchieh Huang provided the clinical data and operation finding.
Authors’ Note
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
The Buddhist Dalin Tzu Chi General Hospital Research Ethics Committee approved the reporting of this case.
Informed Consent
The patient and his legally authorized representative provided written informed consent for this case report to be published in a medical journal.