
Abstract
Serotonin syndrome is a life-threatening syndrome that can occur when medications or drugs that cause serotonergic activity are taken. Frequently this syndrome is caused using 2 serotonergic medications at once or switching from 1 serotonergic medication to another without tapering appropriately. The classic triad of serotonin syndrome is neuromuscular excitability, autonomic dysfunction, and altered mental status. Patients can have symptoms ranging from tachycardia, diaphoresis, fever, and hypertension to severe swings in blood pressure, tremors, hyperreflexia, muscle rigidity, and even death. Most patients admitted to the hospital with fevers, tachycardia with hypertension, or hypotension will have blood cultures drawn as infection can easily explain these symptoms. If these symptoms persist, however, other options should be explored, including serotonin syndrome.
Introduction
Serotonin syndrome is an array of symptoms manifesting due to the overactivity of serotonergic receptors in the central nervous system. This syndrome is often not diagnosed as there is little literature on the topic and no confirmatory tests for it. Most often serotonin syndrome occurs within 24 hours of a medication change or dose adjustment of serotonin-affecting medications. 1 Many symptoms that occur in serotonin syndrome can mimic sepsis or a stroke. In an intensive care unit (ICU), it is extremely important to have serotonin syndrome on the differential for a patient with sustained fever, diaphoresis, hyperreflexia, and clonus after treatment if there are negative blood cultures and computed tomographic scan. The following case is an example of how an alternative diagnosis should be sought after symptoms do not improve on appropriate treatment.
Case Presentation
A 60-year-old man with a past medical history of chronic obstructive pulmonary disease (COPD) and schizoaffective disorder treated with quetiapine was initially admitted to the hospital for a COPD exacerbation due to pneumonia as shown on chest x-ray (Figure 1) along with Bordetella hinzii and group B Streptococcus bacteremia. All home medications were stopped on admission to the hospital. The patient was started on penicillin G and meropenem for the bacteremia. The patient also received dextromethorphan for a cough he developed. After 1 week of treatment, the patient started to become hyperthermic to 105 °F and was tachycardic to a high of 140 beats per minute. The patient also developed severe diarrhea and hypersecretions of the oropharynx were noted. The patient was still alert and oriented but had severe muscle rigidity and clonus which were initially attributed to hyperthermia. The patient then went into respiratory distress and was sedated, intubated, and transferred to the ICU where he was placed on multiple drips, including fentanyl for pain. The patient remained in the ICU for 1 week while broad-spectrum antibiotics and antifungals were given while awaiting results from additional blood cultures, and Clostridium difficile antigen, which ultimately all turned out negative. The patient was not improving after all appropriate treatments were given. The patient was still hyperthermic even on cooling blankets. A trial of cyproheptadine was initiated and the patient became afebrile the next day and was no longer tachycardic. Furthermore, the diarrhea subsided as well. The cyproheptadine was then stopped due to the resolving symptoms but then the patient became febrile and tachycardic again. Cyproheptadine was resumed and 2 days later the patient passed the weaning trial for extubation and was extubated and discharged from the ICU.

X-ray On Admission.
Discussion
Serotonin syndrome encompasses a wide array of symptoms that can vary in intensity and clinical presentation. 2 Although it is most common due to an increase in the dose of antidepressant medication, there are many serotonergic drugs and medications that can compound serotonergic effects leading to serotonin syndrome. There are no specific confirmatory tests for serotonin syndrome as it is namely a clinical diagnosis. A popular diagnostic criterion was developed and referred to as the Hunter Toxicity Criteria Decision Rules (Figure 2). If one does not meet these criteria, a diagnosis of exclusion is still possible. 3 The classic symptoms of serotonin syndrome include a triad consisting of any or all of the following: altered mental status, neuromuscular abnormalities, and autonomic hyperactivity. 4 The most common medications that may cause serotonin syndrome are monoamine oxidase inhibitors, selective serotonin reuptake inhibitors, and serotonin-norepinephrine reuptake inhibitors. 5 A patient on a stable medication regimen interfering with serotonin levels will rarely experience any issues. Serotonin syndrome is much more common when 2 medications are used simultaneously that affect serotonin levels or a recent dosage adjustment is made. In our particular case, the patient was on a stable home dose of quetiapine. This patient recently stopped taking dextromethorphan, which impairs serotonin reuptake from the synaptic cleft. We theorize that this could have increased serotonin levels and subsequently flooded upregulated receptors causing a significant serotonin response. Therefore, dextromethorphan may be responsible for the initial bout of serotonin syndrome. Fentanyl can be responsible for the continuation of serotonin syndrome as it is a direct serotonin agonist. 5
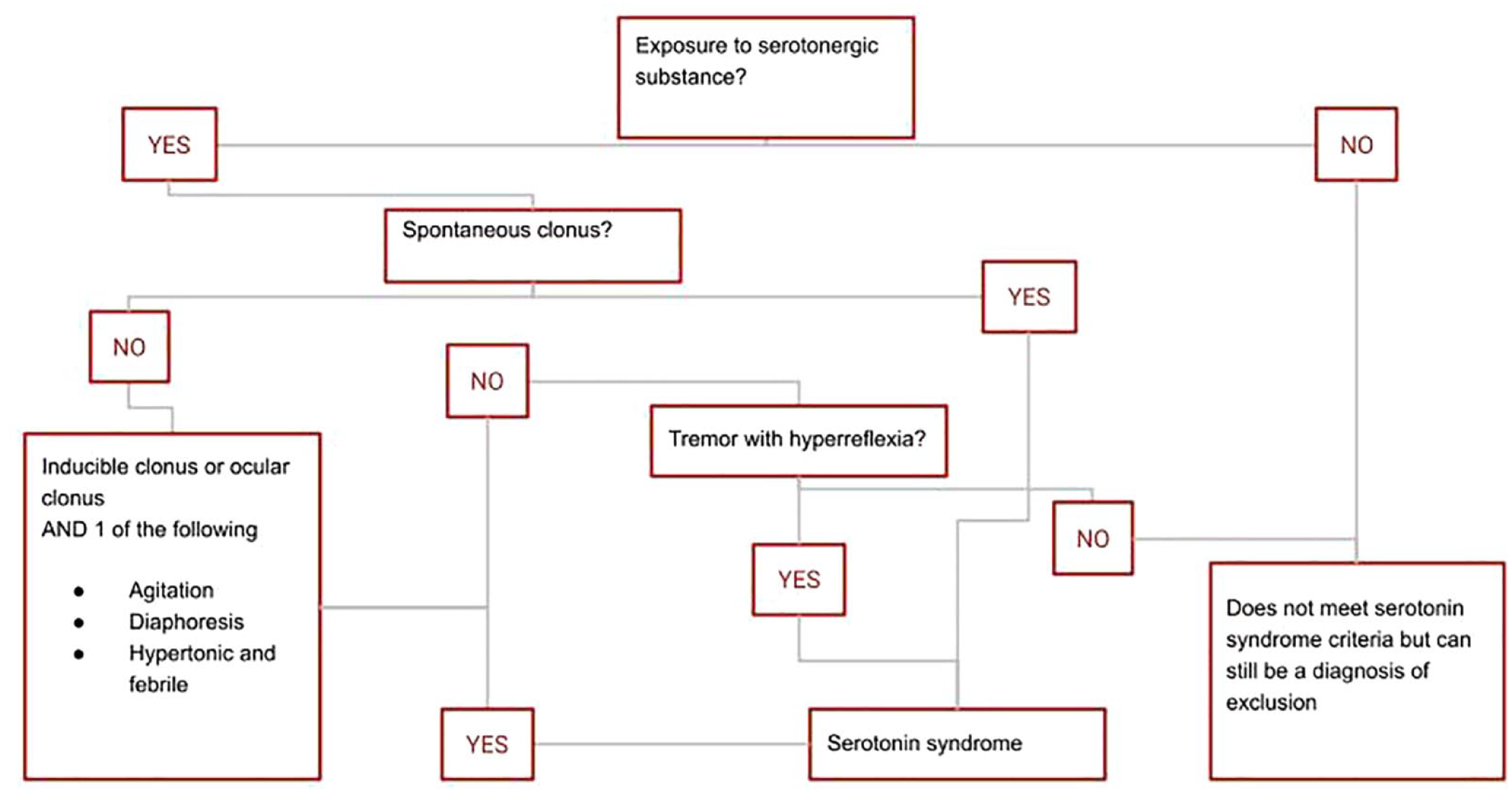
Serotonin syndrome diagnosis flow chart.
Serotonin syndrome can share some similar symptoms with other conditions, such as recurrent sepsis, malignant hyperthermia, other causes of drug-induced fevers, and neurologic causes of a fever. However, there are some differences that can help differentiate serotonin syndrome from these other conditions.
Recurrent sepsis is characterized by repeated episodes of bacterial infections that cause fever. While fever is a common symptom of both serotonin syndrome and sepsis, the other symptoms seen in serotonin syndrome, such as rigors and diarrhea, are not typically seen in sepsis.
Malignant hyperthermia is a rare but potentially life-threatening condition that can occur during general anesthesia. The symptoms can include high fever, muscle rigidity, and rapid heart rate. This can easily be differentiated from serotonin syndrome if the patient did not just receive general anesthesia.
Neurologic causes of fever, such as meningitis or encephalitis, can also cause fever but are typically associated with other neurologic symptoms such as headache, confusion, or seizures. These symptoms are not typically seen in serotonin syndrome.
The treatment of serotonin syndrome usually consists mainly of supportive measures such as fluids and removing the causative agent. In some instances, when this is insufficient, cyproheptadine should be initiated which works as a serotonin antagonist. Chlorpromazine can be used as an alternative through a similar mechanism of action but can be administered intravascularly, whereas cyproheptadine is only available in oral formulations. 6
Conclusion
Patients with unresolved symptoms in a critical care setting should be evaluated for serotonin syndrome. This is especially true for patients who take medications generally that increase the serotonergic effects on the central nervous system. A trial of cyproheptadine may be warranted.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases.
Informed Consent
Verbal informed consent was obtained from the patient for their anonymized patient information to be published in this article.