
Abstract
Pericardial disease is a rare complication after renal transplantation. We present a patient who developed high-output cardiac failure from a large arteriovenous (AV) fistula with recurrent pericardial effusion resulting in a constrictive hemodynamic pattern that was revealed during cardiac catheterization. Pericardiectomy was considered for recurrent effusive pericarditis, but per cardiac surgery recommendations, closure of the AV fistula dramatically cured the patient’s heart failure, and no recurrence of pericardial effusion was seen during follow-up almost a year later.
Introduction
Of all the known causes of heart failure, arteriovenous (AV) fistulas are less common but can cause high-output cardiac failure 1 that can result in the development of transudative pericardial effusions. 2 In patients with pericardial effusion, the amount and rapidity of fluid accumulation determine the development of cardiac tamponade with significant hemodynamic compromise. 3 Recurrent pericardial effusion may eventually develop effusive-constrictive pericarditis. We present a case of recurrent transudative pericardial effusion from right heart failure mimicking effusive-constrictive pericarditis, which resolved completely after closure of an AV fistula that was left patent after renal transplantation.
Case
A 61-year-old man with past medical history of coronary artery disease status postplacement of a bare-metal stent in the ramus branch of the left circumflex artery several years ago had end-stage renal disease secondary to long-term vesicoureteral reflux disease. He had a living donor renal transplantation performed 6 years ago that had remained stable on antirejection therapy with tacrolimus and mycophenolate mofetil. He also had a patent left brachiocephalic AV fistula that was placed for hemodialysis 3 years before his renal transplant.
He was referred to our cardiology clinic with progressive shortness of breath and bilateral lower extremity edema of 4 months duration. An echocardiogram showed moderate pericardial effusion, dilated right and left atria (Figure 1), and severe tricuspid regurgitation with a right ventricular systolic pressure of 41 mm Hg. Autoimmune panel, liver and thyroid function tests, tuberculosis testing, uric acid, and blood urea nitrogen levels were all normal. His glomerular filtration rate was 61 mL/min/1.73 m2. Tacrolimus level was 8.2 ng/mL (expected range 6-15 ng/mL). Furosemide was started with partial symptomatic improvement, but the effusion continued to recur despite diuretic therapy. Tacrolimus was suspected as a potential cause of his pericardial effusion4,5 and was replaced by cyclosporine. However, off tacrolimus, his symptoms continued, and his glomerular filtration ratio (GFR) worsened from 61 mL/min/1.73 m2 just before stopping the medication to 40 mL/min/1.73 m2 almost a month later. Thus, tacrolimus had to be reinstated to prevent rejection of the transplanted kidney.

Echocardiogram (A) parasternal long axis, (B) parasternal short axis, and (C) apical 4 chamber. Moderate pericardial effusion (arrows) and moderately dilated right atrium and left atrium.
Because of the persistence of symptoms with right heart failure and pericardial effusion despite aggressive diuretic therapy, he underwent a pericardial window and was placed on steroid tapering therapy as advised by nephrology. The pericardial fluid analysis revealed a transudate that was negative for malignancy. The anatomic pathologic results on the pericardial tissue sample showed only reactive mesothelial changes (Figure 2). His symptoms improved significantly but recurred 2 months later.

Anatomic pathology after pericardial window. Pericardial tissue with reactive mesothelial cells (arrows) at (A) 10× and (B) 20×.
Cardiac magnetic resonance (CMR) imaging showed moderate pericardial effusion with flattening of the interventricular septum during inspiration, small bilateral pleural effusion, ascites, and normal myocardium (Figure 3). Left and right cardiac catheterization showed a cardiac output of 7.45 L/min, equalization of left ventricular and right ventricular diastolic pressures. The pressure waveform showed prominent Y descent with pronounced right ventricular rapid filling wave the “square root sign” (Figure 4). Coronary angiography showed total occlusion of nondominant right coronary artery with grade 2 left to right collaterals and a patent stent in the ramus branch.

Cardiac magnetic resonance imaging (CMR) showing pericardial effusion (A-C). Bilateral pleural effusion (A, B). Small ascites (A). Ventricular septum flattening during inspiration (C).

(A) Right atrial pressure tracing showing prominent Y descent (arrows). (B) Equalization of biventricular end-diastolic pressures (circle) with pronounced right ventricular rapid filling wave >7 mm Hg.
The CMR and cardiac catheterization results suggested the presence of effusive-constrictive pericarditis, and the patient was then referred to cardiac surgery for possible total pericardiectomy. However, before proceeding with pericardiectomy, per the recommendation of the cardiac surgeon, closure of the patient’s patent AV fistula was performed. To our surprise, shortly after AV fistula closure, the patient’s symptoms completely subsided. An echocardiogram showed a small amount of pericardial effusion and mild tricuspid regurgitation. A repeat cardiac catheterization revealed resolution of the constrictive physiology with normalization of right and left heart hemodynamics (Figure 5; Table 1). He has remained asymptomatic during follow-up approximately 1 year later.

Studies post fistula closure. Left and right heart cardiac catheterization (A and B) showing (A) normal right atrial pressures, prominent Y descent no longer present. (B) There is no equalization of end-diastolic pressures or pronounced right ventricular rapid filling wave. Follow-up echocardiogram 1 month after AV fistula closure (C and D) showing only mild pericardial effusion (arrow).
Hemodynamics From Right and Left Heart Catheterization Before and After Fistula Closure.
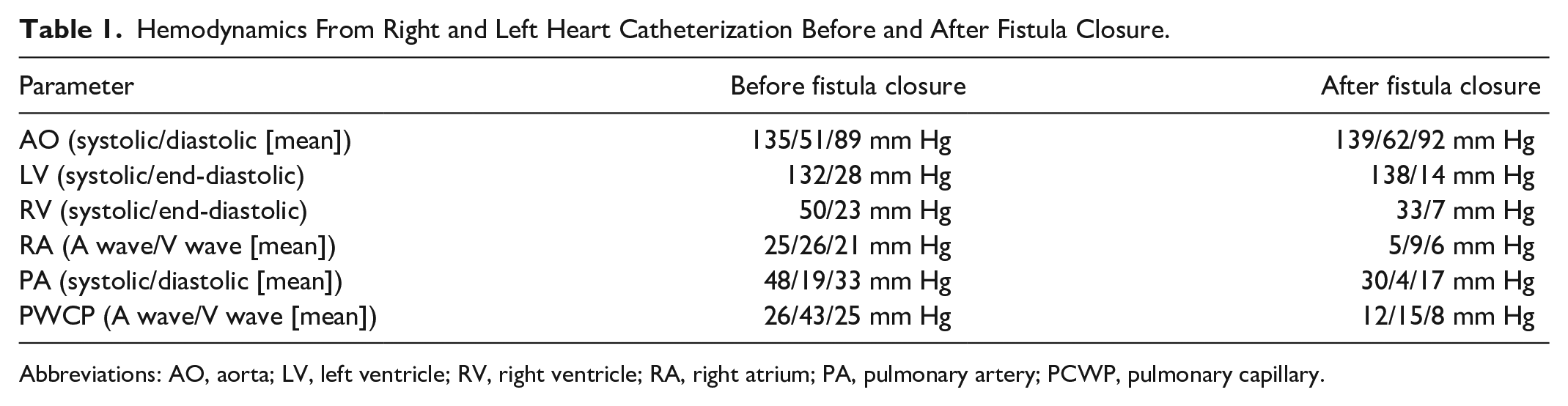
Abbreviations: AO, aorta; LV, left ventricle; RV, right ventricle; RA, right atrium; PA, pulmonary artery; PCWP, pulmonary capillary.
Discussion
Pericardial effusion usually develops with pericarditis that is often associated with the elevation of inflammatory biomarkers like C-reactive protein (CRP), but it can also occur in its absence. 6 In our patient, the recurrent pericardial effusion was a result of right heart failure. The large AV fistula is an important but uncommon cause of high-output congestive heart failure which may lead to recurrent pericardial effusion. 7 A large pericardial effusion or fast accumulation of even small/medium amount of effusion can cause cardiac tamponade with significant hemodynamic compromise. 3 Its definitive treatment will vary depending on the cause of the effusion.
Recurrent pericarditis with or without effusion may lead to constrictive pericarditis causing fibrosis of the parietal and visceral pericardium that restricts diastolic ventricular filling and presents with features of right heart failure. Echocardiogram and CMR are useful diagnostic tools that can also help differentiate between constrictive pericarditis and restrictive cardiomyopathy. The classical finding in cardiac catheterization is equalization of right and left ventricular end-diastolic pressures. The definitive treatment of constrictive pericarditis is total pericardiectomy. 8
Our patient developed recurrent pericardial effusion several years after renal transplantation. The absence of exudative features in the pericardial fluid and further laboratory studies ruled out uremia, tuberculosis, and autoimmune diseases as possible underlying causes of recurrent pericardial effusion. Tacrolimus was temporarily suspected to cause recurrent pericarditis as there are cases linking its use to effusive pericarditis.4,5 His symptoms and pericardial effusion did not improve even after discontinuation of tacrolimus, several pericardial drainages, and the creation of a pericardial window. The patient was being made ready to undergo a pericardiectomy, an invasive and complicated procedure, which was proven to be unnecessary after the preoperative closure of his AV fistula.
Right heart failure with pericardial effusion may mimic effusive-constrictive pericarditis, and it can be difficult to differentiate between them. The diagnosis of effusive-constrictive pericarditis should be based on hemodynamic findings, cardiac computed tomography, or CMR and confirmed by performing a combined pericardiocentesis and cardiac catheterization. 8 Although not definitive, other findings that pointed away from effusive-constrictive pericarditis were the absence of pericardial fibrosis after the pericardial window (Figure 2) and the absence of pericardial calcifications or thickening on CMR.
Conclusion
In patients with recurrent pericardial effusion and systemic venous congestion, even years after renal transplantation, the possibility of high-output congestive heart failure caused by a patent AV fistula for prior hemodialysis should be kept in mind.
Footnotes
Author Contributions
ACS contributed by conceptualizing and writing the original draft. MV contributed by conceptualizing and writing the original draft. RS contributed by writing original draft. AM contributed by writing original draft. MM contributed by supervision and review. SPM contributed by supervision and review.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our Institution does not require ethical approval for reporting individual cases.
Informed Consent
Informed consent was obtained for publication of this case report.