
Abstract
Commonly, pericardial effusions can cause suboptimal heart contractility. Larger pericardial effusions can lead to compression of structures that surround in the heart in the mediastinum. Our patient presented with dyspnea that required mechanical ventilation. Bronchoscopy revealed compression of the bronchus from an external source. Echocardiogram showed a large circumferential pericardial effusion, which compressed the left main stem bronchus causing left lung atelectasis and persistent respiratory failure. A subxiphoid pericardial window was performed, which led to an improvement in her oxygen requirements. This case portrays the importance of including pericardial effusions in patients who present with respiratory failure refractory to antibiotic treatment and intervention with bronchoscopy. Although our patient passed away, recognition and earlier appropriate management with a pericardial window or pericardiocentesis could have prevented this adverse event.
Introduction
Pericardial effusion can occur as a result of inappropriate fluid accumulation within the pericardial cavity. 1 Commonly, pericardial effusion can lead to internal compression causing suboptimal heart contractility. However, slower growing, large pericardial effusions can lead to compression of surrounding structures in the mediastinum. We present a case of pericardial effusion, which led to the compression of the left main stem bronchus causing left lung atelectasis and persistent respiratory failure. Our patient had an improvement in respiratory status shortly after pericardial window, suggestive of the importance of this association and its appropriate management.
Case Presentation
We present the case of a 57-year-old Caucasian female with a past medical history significant for a repaired atrial septal defect and unrepaired ventricular septal defect, Eisenmenger’s syndrome, heart failure with preserved ejection fraction, prior cataracts, and chronic obstructive pulmonary disease who presented to our cardiac intensive cardiac unit from an outside facility for management of her pericardial effusion.
She initially presented to an outside hospital for increasing dyspnea and productive cough. She required intubation. She was found to have Enterococcus and methicillin-sensitive Staphylococcus aureus pneumonia and was started on appropriate antibiotic therapy. Imaging done at the outside hospital showed collapse of the left lung. Computed tomography scan of the thorax (Figure 1) showed the presence of a large pericardial effusion measuring up to 2.5 cm in thickness along the left ventricle and left lower lobe atelectasis. Bronchoscopy showed mucous plugging with bronchomalacia of the left main bronchus. The left mainstem bronchus was visualized as being compressed from an outside source. Our patient failed extubation after bronchoscopy and arrived at our facility intubated and sedated. Ventilator settings were pressure-regulated volume control with a respiratory rate of 12 breaths per minute, tidal volume of 300 mL, fraction of inspired oxygen of 60%, and positive end-expiratory pressure of 10. Her oxygen saturation was found to be in a range of 82% to 85%.

Computed tomography scan of the thorax showed the presence of a large pericardial effusion measuring up to 2.5 cm (blue arrow) in thickness along the left ventricle and left lower lobe atelectasis.
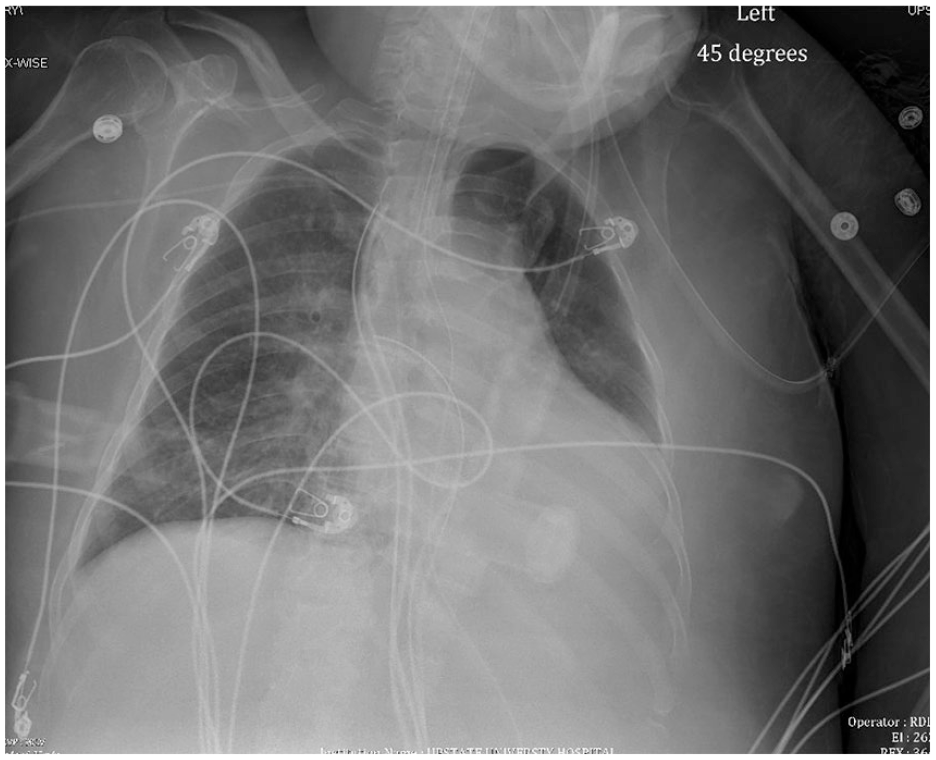
Chest radiography showed atelectasis of the left lower lobe (Figure 2). Transthoracic echocardiogram (Figure 3) was performed, which showed a large circumferential pericardial effusion with normal inferior vena cava morphology. There was tricuspid morphology that was consistent with Ebstein’s anomaly. Ejection fraction was noted to be 45% to 50% and atrial/ventricular septal defects were seen. Chamber collapse was not visualized.

Chest radiograph on admission showed atelectasis (blue arrow) of the left lower lobe.

Transthoracic echocardiogram showing a large circumferential pericardial effusion (blue arrow).
A subxiphoid pericardial window was performed the day after admission with 400 mL of purulent fluid drained along with pericardial and thoracic drain placement. A transesophageal echocardiogram done immediately after the procedure showed resolution of the pericardial effusion. Following the procedure, her oxygen saturation improved to the 88% to 90% range.
The following day, she was noted to have an output of 280 mL from her pericardial drain. Chest radiography showed improvement in aeration of the left lung (Figure 4). Transthoracic echocardiogram (Figure 5) after the procedure showed a small residual pericardial effusion with an ejection fraction of 60% to 65%. She was started on a furosemide drip at 10 mg/h.
Chest radiography showing overall improvement in aeration of the left lung after a pericardial window.

Transthoracic echocardiogram after the pericardial window showing resolution of the pericardial effusion.
Pericardial effusion cultures grew methicillin-sensitive Staphylococcus aureus, for which our patient was started on cefazolin, as per Infectious Disease team recommendations. She was treated with inhaled nitric oxide. Her oxygen requirements initially decreased; however, our patient was made comfort care and was terminally extubated.
Discussion
Left lung collapse secondary to compression by a pericardial effusion is an extremely rare occurrence with only 3 similar cases reported in literature, to our knowledge.2,3 The mediastinum is a tightly packed cavity that houses the trachea, right and left mainstem bronchi, esophagus, and the heart. As a result, any derangements, enlargement, or inflammation in any of the organs situated in the mediastinum have a direct effect on surrounding structures.
Pericardial effusion occurs as a result of inflammation or infection and is defined by an accumulation of fluid within the pericardial cavity, which surrounds the myocardium. In the case of our patient, fluid analysis showed the growth of methicillin-sensitive Staphylococcus aureus. We can presume that this pericardial effusion was purulent, and the etiology was infectious. The likely source of the infection could be underlying pneumonia, with contiguous spread. The exudative nature of the effusion could also explain the rapid accumulation and subsequent compression of surrounding anatomical structure.
Clinically, pericardial effusions could present anywhere on the spectrum from acute chest pain to hemodynamic instability. Large pericardial effusions can lead to the compression of the heart chambers, leading to decreased contractility, impaired diastolic function, and subsequent hemodynamic instability. 4 In some instances, large pericardial effusions could compress structures around rather than within the myocardium. Notably, the left mainstem bronchus is located directly posterior to the heart. With regard to the left lung atelectasis that ensued in our patient, we can presume that it was either due to an intrinsic or extrinsic compression of the left mainstem bronchi. After bronchoscopy and removal of the mucus plugs failed to improve our patient’s respiratory status, it became apparent that the bronchus was compressed from an external source.
Bronchi are robust and sturdy structures made of thick cartilage, which ideally are resistant to external compression. 5 However, the combination of bronchomalacia (likely secondary to infection and course of intubation), and a pericardial effusion led to the left lower lobe atelectasis seen in our patient. The improvement in respiratory status shortly after the pericardial window, as seen on chest radiography and improved oxygenation, further goes to show that the pericardial effusion was the etiology of her left lower lung atelectasis.
Conclusion
Although very rare, this case highlights the importance of associating pericardial effusion with left lung atelectasis in patients who present with respiratory failure that is refractory to antibiotic treatment and intervention with bronchoscopy. Interventions such as pericardial window or pericardiocentesis would be beneficial to relieve the external compression.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Verbal informed consent was obtained from the patient for their anonymized information to be published in this article.