
Abstract
Mulibrey (
Introduction
Mulibrey Nanism syndrome (MUL) is a rare, autosomal recessive genetic disorder caused by truncating mutations in the TRIM (tripartite motif) 37 gene located at 17q22-q23 that encodes a RING-B-box-coiled-coil zinc-finger family of proteins. The function of these proteins is not completely understood.1,2
MUL is mostly seen in the Finnish population, with sporadic non-Finnish cases reported. 3 It is associated with growth failure, midface hypoplasia, retinal pigmentary changes, cardiac involvement, muscular hypotonicity, and hepatomegaly.2,4
We present one of the oldest reported cases of MUL, highlighting the importance of early recognition and treatment of constrictive pericarditis.
Case
A 57-year-old female presented with worsening fatigue, shortness of breath, and anasarca. Her past medical history was significant for MUL with constrictive pericarditis that required pericardiectomy at age 12, diastolic congestive heart failure (CHF), atrial fibrillation, infertility, liver cirrhosis, and diabetes mellitus type 2.
On physical exam at admission, her blood pressure was 120/62, with an irregularly irregular heart rate of 81 beats per minute, oxygen saturation more than 95% on room air, and a temperature of 36.7°C. Pitting edema bilaterally on upper and lower extremities with abdominal distention, ascites, and bilateral lower lung rales were noted.
Laboratory analysis was significant for elevated proBNP at 3899 pg/mL and red cell distribution width 22.7%, low hemoglobin 6.7 g/dL, hematocrit 22.4%, mean corpuscular volume (MCV) 66.4fl, iron saturation 5.2%, and ferritin 12 ng/mL. The percentage of reticulocytes was 1.8% with an absolute reticulocyte count of 1 and a reticulocyte index of 0.48. Folate and vitamin B12 were normal at 6.92 ng/mL and 555 pg/mL, respectively. These results indicated chronic, hypo proliferative, microcytic, hypochromic anemia likely due to iron deficiency.
She also had thrombocytopenia 142,000/uL, hypoalbuminemia 2.6 g/dL, and slight hyperammonemia 61 umol/L. These results were chronic, secondary to liver cirrhosis and appeared stable compared to previous results. Urinalysis showed slight proteinuria at 30 mg/dL and hematuria at 272 red blood cells/HPF (high power field).
Chest x-ray showed pulmonary vascular congestion, cardiomegaly, diffuse pulmonary interstitial edema, and bilateral pleural effusions. Computed tomography of the abdomen and pelvis showed a nodular, cirrhotic liver, abdominal ascites. Echocardiogram showed preserved ejection fraction of 55% to 60% and moderate mitral and tricuspid regurgitation with grade II diastolic dysfunction. The patient’s anasarca, ascites, and pulmonary congestion were all multifactorial in etiology and mostly due to known complications of MUL.
For her cirrhosis, she was following with gastroenterology as an outpatient, the decision not to pursue a liver biopsy had been made as the results would likely not have changed management. Blood work to rule out other medical causes including alpha-1 antitrypsin deficiency, anti-nuclear antibodies, anti-smooth muscle antibodies, IgG, IgA, IgM, and hepatitis viral panel were within normal limits. Her liver cirrhosis was thought to be secondary to CHF.
She was managed with furosemide boluses, which were later changed to continuous furosemide drip due to poor urine output. Diuresis effects were suboptimal throughout the admission course due to third spacing secondary to hypoalbuminemia. Ongoing electrolyte imbalances further complicated her management. Later she developed altered mental status. A computed tomography scan of the head was done which did not show any acute changes. Her ammonia levels were increasing despite being on rifaximin, lactulose, and spironolactone which indicated worsening decompensated cirrhosis.
Due to worsening respiratory and mental status as well as lack of improvement despite maximal medical therapy. Following discussion with family, comfort care measures were ensued leading to the patient’s demise.
Discussion
TRIM37 encompasses a family of 37 proteins with common cellular functions and compartmentalization. They are a subfamily of E3 ligases that mediate the transfer of ubiquitin to substrate target proteins. TRIM37a is the major human transcript. There are several alternatively spliced variants, the most common is TRIM37b. 3
Overexpression of TRIM37 has been associated with different types of neoplasms. Its deficiency results in MUL. It is also associated with neoplasms including thyroid, kidney, and lymphoblastic leukemia.3,5
There have been approximately 26 TRIM37 mutations associated with MUL. The most common is a truncating mutation known as the Fin-major mutation (c.493-2A > G) of which there are more than 100 cases reported. 1 Rearrangements and gene deletions have also been reported.3,6,7 Unfortunately, our patient was diagnosed with MUL several decades ago and there were no records of genetic testing done.
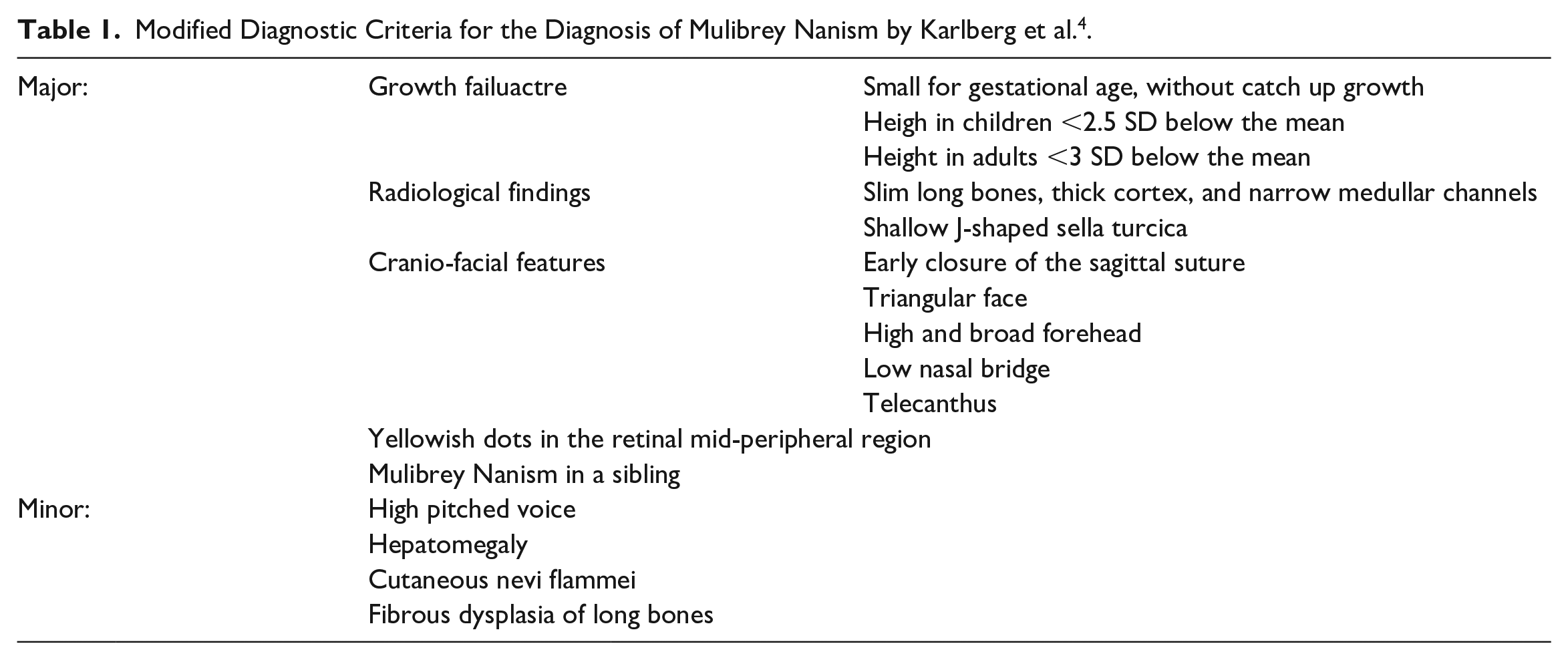
Clinical diagnosis of MUL is made using the modified diagnostic criteria (Table 1). Diagnosis is made with the presence of three major plus one minor or two major plus three minor criteria. 4 The main differential diagnosis in patients with MUL is Silver Russel Syndrome. The differentiating features of MUL are hepatomegaly, cardiac involvement, yellow dots in ocular fundi, cortical thickening, and fibrous dysplasia of long bones.4,8
Modified Diagnostic Criteria for the Diagnosis of Mulibrey Nanism by Karlberg et al. 4 .
Pregnancy and delivery are mostly uneventful. Poor fetal growth has been reported in less than a third of cases. Most newborns are small for gestational age, catch-up growth is seen 6% of the time. Failure to thrive is common, requiring nasogastric tube in almost a third of patients and less frequently, percutaneous gastrostomy tube. 4
Respiratory tract Infections are common and respiratory failure can be seen 25% of the time. 4 This could be explained by the fact that TRIM37 has been identified as a mediator in the regulation of innate immunity and is related to the expression of genes associated with the inflammatory pathway, specifically with ubiquitination of NF-kB related proteins. 3
Liver involvement is common. Fatty liver is seen in all adults and adolescents. 9 In half the patients, hepatomegaly is seen at the time of diagnosis which has been theorized to be due to heart failure given histopathological studies showing chronic congestion. 4
Up to 70% of patients with MUL develop metabolic syndrome. In patients younger than 10 years old, hypoglycemia was recorded half of the time. In contrast, at >20 years old 92% of patients had either impaired glucose tolerance or type 2 diabetes mellitus. This change in glucose metabolism was accompanied by abdominal obesity, overweight, acanthosis nigricans, hypertension, and increased triglycerides.4,9
Hypogonadism and infertility are common. The median age of menarche is about 12 years, half the women don’t have regular menses, 10 years after menarche 8% will have regular menses. Ovaries are usually hypoplastic and most patients have less than two antral follicles on ultrasound. 10 In males, testicular size is small and semen samples show impaired sperm motility with or without decreased sperm count. 11
Cardiac complications are the most important driver of mortality in these patients. The most common cardiac manifestations are CHF and constrictive pericarditis seen in up to 51% and 39% of the cases, respectively. Echocardiographic findings are characterized by left ventricular hypertrophy and diastolic dysfunction with preserved systolic function irrespective of previous pericardiectomy. 12
Lipsanen-Nyman et al found that patients who died from cardiac causes died younger than those from non-cardiac causes, on average 6.8 versus 33.7 years, respectively. Microscopic analysis of diseased pericardium almost invariably shows extensive fibrosis. 12
The standard treatment for patients with constrictive pericarditis is pericardiectomy. As the disease progresses adherence of the pericardial layers to the myocardium may complicate the procedure. 12 Pericardiectomy has shown more benefits in patients with New York Heart Association (NYHA) class II or III compared to class IV. 13 Our patient underwent a pericardiectomy at 12 years old, soon after cardiac symptoms started and constrictive pericarditis was diagnosed. She was subsequently diagnosed with mild diastolic dysfunction, which remained stable for approximately 44 years. Her diastolic CHF deteriorated in her last year of life, leading to her demise. Our patient lived a relatively normal life, she attended college, had stable work, and was an active member of her church.
Although pericardiectomy is the treatment of choice, it is important to remember that constrictive pericarditis is often accompanied by diastolic CHF. Anwer et al 14 successfully performed a heart transplant in a patient with extensive pericardial calcifications extending into the myocardium and suggest that cardiac transplant in these patients might be used as definitive treatment. More research is needed to demonstrate the effectiveness of this therapy.
Conclusion
In patients with Mulibrey Nanism syndrome with constrictive pericarditis, early pericardiectomy is associated with improved mortality, potentially allowing them to live a normal or near-normal life.
Footnotes
Acknowledgment of Authorship
Andres Cordova Sanchez: conceptualizing and writing original draft; Mostafa Vasigh: conceptualizing and writing original draft; and Robert Carhart: supervision and review.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our Institution does not require ethical approval for reporting individual cases.
Informed Consent
Informed consent for patient anonymized information to be published in this article was not obtained from the patient because our institution does not require informed consent for individual case reports with information anonymized.