
Abstract
Left ventricular (LV) thrombosis usually occurs as a complication of acute anterior myocardial infarction (MI) and dilated cardiomyopathy. It also occurs in patients with a hypercoagulable state. However, in the setting of normal systolic function, LV thrombi are extremely rare. We present a case of a healthy woman who had LV thrombus despite normal LV systolic function that presented as an acute aortoiliac embolism.
Introduction
Virchow’s triad describes 3 factors that can explain thrombus formation: stasis, endothelial damage, and hypercoagulability. Most ventricular thrombi occur in the presence of impaired left ventricular (LV) function such as dilated cardiomyopathy and aneurysms or following myocardial infarction (MI). We report an LV thrombus in a patient with normal LV function and structure presenting with an acute aortoiliac embolism.
Case Presentation
A 54-year-old Caucasian woman presented to our emergency department with complaint of progressive right leg pain and weakness of 2-hour duration. She had a history of uncontrolled type 2 diabetes and 30-pack-year smoking. She had no previous similar symptoms, coagulopathies, trauma, recent travel, or use of hormonal medications. On physical examination, blood pressure was 163/115 mm Hg, heart rate was 111 beats/minute, respiratory rate was 16 breaths/minute, temperature was 36.5°C, and oxygen saturation was 100% on room air. The patient had right leg skin mottling and tenderness over the right thigh with loss of sensation distal to the calf. Right dorsalis pedis and posterior tibial pulses were absent, and the extremity was cold. The rest of the physical examination was unremarkable. Initial laboratory workup was significant for leukocytosis of 21 100 cells/µL (normal, 3500–10 600 cells/µL). Other labs were unremarkable. A computerized tomography (CT) scan of the head was normal, whereas an abdominal CT-angiogram revealed a near-complete occlusion at the aortoiliac bifurcation, bilateral common iliac arteries, and proximal left internal iliac artery secondary to thrombosis. She was started on a heparin infusion and underwent a bilateral aortoiliac embolectomy.
After the procedure, she had palpable pulses in the bilateral lower limbs. The patient received low-dose aspirin of 81 mg and atorvastatin 80 mg daily. Although her initial troponin level was normal, postoperatively her troponin level began trending up from 79 to 321 ng/L. Postoperative electrocardiogram (ECG) showed a right bundle branch block with no ischemic changes (Figure 1), similar to the preoperative ECG (Figure 2). Transthoracic echocardiogram (TTE) revealed 2 mobile pedunculated echo-densities in the LV apical region measuring 1.8 × 1.2 cm and 1.0 × 0.5 cm within the setting of a normal LV ejection fraction of 55% and normal wall motion (Figure 3). A subsequent transesophageal echocardiogram (TEE) was performed and provided a better visualization as it showed a large mobile echo-density (2.3 × 2.1 cm) with a stalk attached to the anterior wall of the left ventricle (Figure 4) and a second smaller mobile echo-density attached to the apex of LV. The patient’s condition was further investigated for underlying hypercoagulability and systemic autoimmune or cancerous conditions, but her homocysteine levels, antinuclear antibody, antineutrophil cytoplasmic antibody, anti–double-stranded DNA, anticardiolipin antibodies, anti-β(2)glycoprotein 1 antibody, activated protein C resistance, protein C and protein S activity, antithrombin activity, factor V Leiden, antithrombin activity, and the tumor marker assays Cancer Antigen (CA) 15-3, CA 19-9, CA 125, and alpha-fetoprotein were all within normal limits. The CT scan of the thorax, abdomen, and pelvis—with and without contrast—to rule out malignancy was unremarkable. The patient underwent cardiac catheterization, which revealed nonobstructive coronary disease. Cardiothoracic surgery revealed LV mass excision, which was grossly described as a pedunculated mass attached to the anterolateral LV wall close to the tip of the papillary muscle, along with another smaller mass attached to the LV apex. Pathology confirmed that the masses were consistent with thrombi. Subsequently, the patient was treated with warfarin with a target international normalized ratio (INR) of 2 to 2.5. The patient improved clinically and was discharged to follow up with vascular surgery, hematology, and cardiac surgery teams.

Postoperative electrocardiogram shows a right bundle branch block (RBBB).

Preoperative electrocardiogram shows a right bundle branch block (RBBB) with artifacts.

Transthoracic echocardiogram with contrast shows 2 mobile echo-density masses in the left ventricular apical region measuring 1.8 × 1.2 cm (red arrow) and 1.0 × 0.5 cm (yellow arrow).
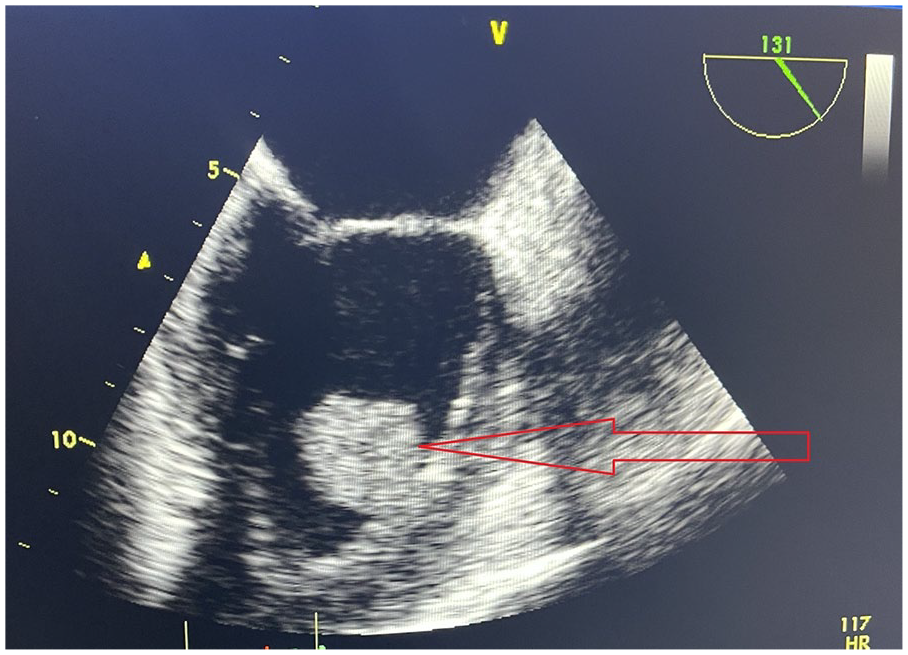
Transesophageal echocardiogram shows a large mobile echo-density (2.3 × 2.1 cm) with a stalk attached to the anterior wall of the left ventricle.
Discussion
Left ventricular thrombus formation with normal LV ejection fraction is a rare clinical entity, as only 33 similar cases have been documented so far in the literature. Most cases presented with systemic embolic signs and symptoms.1,2 In a case series of 31 patients, with a median age of 43 years and slight male predominance (58%), embolic complications made up the primary presenting conditions in about 27 (88%) patients, and febrile illness was present in only 3 patients. 3
Unlike our patient, most reported cases of LV thrombus with normal LV ejection fraction occurred secondary to medical conditions associated with greater risk of thrombosis formation, such as inflammatory conditions (rheumatoid arthritis, systemic lupus erythematosus, inflammatory bowel diseases), blood dyscrasias (essential thrombocythemia, hyperaggregable platelets, protein C or S deficiency), or malignancies.4-6 Similar to our patient, 2 case reports identified LV thrombus with no underlying cause.7,8
Overall, after evaluating the patient’s clinical features, laboratory results, echocardiographic imaging, and age-appropriate cancer screening, we could not identify any underlying cause that would lead to LV thrombosis formation except for her pre-existing risk factors of diabetes and heavy smoking.
The LV apex is considered the most common site for LV thrombi in patients with normal LV systolic function; other sites include the septum and mitral valve apparatus. 9 Our patient had 2 thrombi, one at the apex and the other at the anterolateral wall, which look similar to myxoma but in an unusual site and without pathologic findings of myxoma.
There are no consensus guidelines for treating LV thrombus in patients with normal LV systolic function. However, the 2014 American Heart Association/American Stroke Association stroke-prevention guidelines recommend treating LV thrombus following MI with a vitamin K antagonist for 3 months with a goal INR value of 2 to 2.5. 10 If repeat imaging shows resolution of the thrombus, cessation of oral anticoagulation is recommended. Conversely, oral anticoagulation should be resumed if the thrombus persists. 11 However, as the literature has reported thrombi recurrence, individuals with normal LV systolic function and no identifiable cause require prolonged anticoagulation 3 ; we have advised our patient to take vitamin K antagonist with goal INR values of 2 to 2.5 and follow up closely to reassess the anticoagulation duration periodically.
Conclusion
Left ventricular thrombi are extremely rare in the setting of normal LV function and may be mistaken for cardiac tumors. Anticoagulation is the mainstay treatment, with or without surgical intervention. However, the duration of anticoagulation is currently unknown.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Verbal informed consent was obtained from the patient for their anonymized information to be published in this article.