
Abstract
A 66-year-old female was found hypotensive in ventricular tachycardia (V-tach). Workup confirmed septic shock and takotsubo cardiomyopathy (TCM) with left ventricular (LV) thrombus. Despite the initiation of anticoagulation therapy, she developed an embolic stroke on day 14. Malignant ventricular arrhythmia and LV thrombosis are rare complications of TCM. However, there is no specific guideline regarding prophylactic anticoagulation.
Introduction
Takotsubo cardiomyopathy (TCM) or broken heart syndrome is defined as a stress-induced reversible systolic dysfunction of the heart in the absence of significant coronary artery disease. It may occur more frequently in postmenopausal women. Different mechanisms, including coronary artery vasospasm and hyperstimulation of the sympathetic system, have been associated with TCM. 1 Thrombus formation is one of the complications of TCM, which is caused by blood stasis, endothelium damage, and hypercoagulability. In takotsubo, cardiomyopathy thrombosis can happen due to excessive catecholamine release and apical hypokinesis. 2 In this case report, we are presenting an interesting case of ventricular tachycardia and later embolic cerebral vascular accident (CVA) secondary to left ventricular (LV) thrombus in a patient with TCM while on anticoagulation.
Case Presentation
A 66-year-old Caucasian woman with past medical history of poorly controlled diabetes mellitus, peripheral neuropathy, neurogenic bladder, major depressive disorder, hypertension, chronic pain, and bilateral hip osteoarthritis brought to emergency room (ER) by paramedics with chief complaint of altered mental status. Per paramedics, the patient was found to be in ventricular tachycardia and hypotensive at home and was defibrillated at the scene. Upon arrival at ER, the patient was febrile with a temperature of 38.6°. Her blood pressure, heart rate (HR) and respiratory rate (RR) were 114/74 mmHg, 140 and 28, respectively. She was found to have atrial flutter with 2:1 atrioventricular conduction with chronic right bundle-branch block (Figure 1).
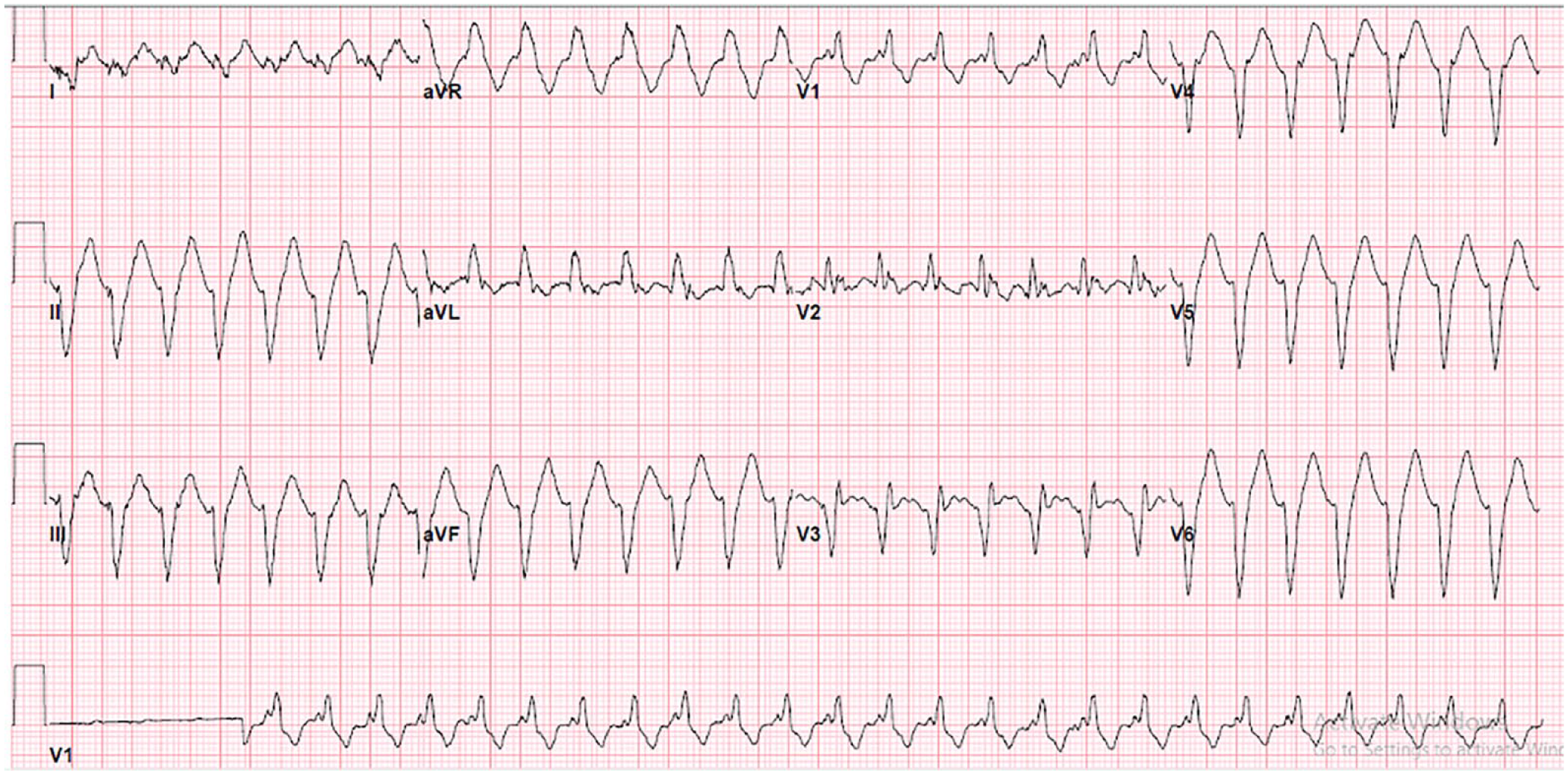
Electrocardiogram (ECG) on admission, shows atrial flutter with 2:1 atrioventricular (AV) conduction with chronic right bundle-branch block.
She was given IV amiodarone bolus and started on drip in the ED. Lab was significant for leukocytosis, hypokalemia (K:3.4 mmol/lit), elevated high sensitivity troponin (1505 pg/mL), elevated lactic acid (5.3 mmol/L), and A1C 11%. Physical exam was benign except for a huge left elbow abscess. Abscess drainage was performed in the ER, which grew methicillin sensetive staph aureus. Later in the ER, the patient became hypotensive, and she remained hypotensive despite receiving 2.5 L of normal saline. Patient was admitted to the ICU with the diagnosis of cardiogenic or septic shock. Patient was started on broad spectrum coverage with cefepime and vancomycin. Patient was started on pressor, Levophed. And, cardiology was consulted for further management. Urgent transthoracic echocardiography showed moderate-to-severe cardiomyopathy with severe apical hypokinesis with ejection fraction (EF) of 35% to 40% most consistent with ischemic heart disease with possible old apical infarction or stress-induced cardiomyopathy/TCM. Moreover, a partially mobile, multilobular echodense mass (2.1 cm × 1.5 cm), attached to the apex and anteroseptal LV was noted, worrisome for LV Thrombus (Figure 2). There was no valvular vegetation to suggest any infective endocarditis. Intravenous heparin drip was started for anticoagulation.

Multilobular echodense mass (2.1 cm × 1.5 cm), attached to the apex and anteroseptal left ventricular (LV).
Meanwhile, blood culture grew MSSA in 2 of 2 bottles. Once the patient weaned off the pressors, she was started on a congestive heart failure (CHF) guideline medical therapy. Coronary angiography was initially deferred while the patient was septic. Infectious disease was consulted, and antibiotics were de-escalated to IV nafcillin. The patient underwent a left elbow bursectomy by an orthopedic surgeon. Once the patient recovered completely from sepsis, cardiac catheterization was performed for the new onset heart failure. Angiography demonstrated single-vessel coronary artery disease involving 80% ostial stenosis of the second diagonal. The left anterior descending artery (LAD) itself had nonobstructive disease with 40% to 50% focal stenosis just prior to the origin of this 2nd diagonal. TIMI 3 flow was present in LAD and diagonals. Left main, left circumflex/OM, and dominant right circumflex artery (RCA) were all angiographically clear of disease (Figure 3).

Patent left main, left anterior descending artery (LAD), left circumflex/obtuse marginal (OM), and diagonals.
Based on the catheterization finding, the diagnosis of TCM was made. While on heparin drip, warfarin was started with an international normalised ratio (INR) goal of 2.0 to 3.0. On hospital day 14, she developed acute expressive aphasia. CT/CTA/CTP head and neck revealed acute infarct in the left parieto-occipital lobe with an ischemic core of 3 cc, total hypoperfusion of 11 cc, mismatch volume of 8 cc and a mismatch ratio of 3.7 without intracranial hemorrhage, mass effect, or significant stenosis. Her NIHSS was 1 and she was not a candidate for tissue plasminogen activator (TPA). Brain magnetic resonance imaging (MRI) demonstrated subacute infarct in the left parietal lobe with smaller subacute infarct in the right frontoparietal centrum semiovale. Transesophageal echocardiogram (TEE) was performed to rule out infective endocarditis as one of the reasons for this cardioembolic event. TEE showed improved EF to 50% to 55% and resolution of TCM. Moreover, the LV thrombus had almost resolved except for a small mobile mass attached to the apical septum. She was discharged on guideline directed medical therapy (GDMT) for nonischemic cardiomyopathy, warfarin, amiodarone, and 6 weeks of intravenous (IV) cefazolin.
Discussion
Malignant ventricular arrhythmias are known complications of TCM. The prevalence varies from 2 to 13.5% in different studies. Reentry, triggered activity and automaticity were identified as the major mechanisms. 3 In our case, we do believe the ventricular tachycardia was due to underlying cardiomyopathy and demand myocardial ischemia while the patient was septic.
Current data almost exclusively consist of isolated case reports and a few case series. The incidence of LV thrombosis in patients with TCM widely varies. In the literature review, LV thrombus was reported in 5.7% of patients. 4 However, the incidence of LV thrombus was reported 2.2% in Francesco’s study. It is also reported that all thrombus were documented within the first 5 days of hospitalization. 5 However, in our case the condition happened several weeks after the initial presentation.
The incidence of the thromboembolic events varies in TCM. CVA was seen in 17% of patients with LV thrombus in the study of Francesco. 5 However, in the study of Heckle, thromboembolic events were reported in 9.2% of patients with TCM. 4 Moreover, thromboembolic events can happen in the absence of LV thrombus. LV thrombus was not reported in 38% of patients who had a thromboembolic event in the study of Heckle. 4
In 2013 STEMI guideline, there is a IIb recommendation to anticoagulated patients with massive anterior MI. 6 Of note, the incidence of thromboembolic events can be higher in patients with TCM compared with patients with acute coronary syndrome. 7 Similar studies were performed on patients with TCM. In the study of Haghi, the sensitivity, specificity, and positive and negative predictive value of c-reactive protein in prediction of LV thrombus formation in patients with TCM was 100%. 8 Furthermore, in the study of El-Battrawy, CRP was reported as the only single predictor of thromboembolic events in patients with TCM. 7 D-dimer was found to be significantly higher in patients with LV thrombus compared with the patients without thrombosis in the study which was performed on patients with anterior MI who underwent LADA PCI. 9 In another study, troponin level more than 10 was the only predictor for LV thrombus formation. 5 Unfortunately, D-dimer and CRP were not available in our case. However, HS-troponin was elevated in our case (1500 pg/mL).
Little is known about the role of prophylactic anticoagulation in patients with TCM. 10 In one of the studies done in Europe, prophylactic use of oral anticoagulation (OAC) was recommended in patients over 75 years old, EF < 35%, moderate or severe mitral regurgitation, and LV outflow tract obstruction. 10 In Francesco’s study, it is recommended that prophylactic OAC for 3 months in patients with troponin level > 10 ng/mL and apical ballooning is safe and effective approach in LV thrombus in TCM. 5
A similar event happened to our patient, who had an embolic stroke while she was on warfarin with heparin bridging. In different studies, details about the dosage and duration of anticoagulation therapy were not clear.
In general, it is recommended to use anticoagulation till resolution of systolic dysfunction. 10 However, our case report suggested that anticoagulation until normalization of LV function may not be adequate. Based on the studies, there might be a significant association between thrombosis in patients with TCM and inflammatory markers such as CRP and D-dimer. However, considering that our patient was septic, the inflammatory markers would not have been of value and predictive of thrombosis. Given the fact that thromboembolic events can happen in the absence of documented LV thrombosis, to formulate firm recommendations on identifying proper candidates for prophylactic anticoagulation therapy, further studies are needed to find out the association and predictive tools for thrombosis and cardioembolic events in patients with TCM.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Verbal informed consent was obtained from the patient for their anonymized information to be published in this article.
Prior Presentation of Abstract Statement
Not presented before.