
Abstract
Neuroendocrine tumors (NETs) are a relatively rare entity; however, the incidence and prevalence of these tumors are increasing, likely attributed to improved diagnostic accuracy. The diagnosis of suspected NETs is facilitated by clinical symptoms, laboratory test abnormalities such as elevated chromogranin-A, and other diagnostic modalities such as the use of computed tomography scans, magnetic resonance imaging scans, positron emission tomography (PET) scans, and biopsy. The expression of high levels of somatostatin receptors in NETs enables the use of a specialized PET scan using the radiolabeled somatostatin analogues 68Ga-DOTATATE. The sensitivity and specificity of 68Ga-DOTATATE PET is very high for the diagnosis of NETs, but the specificity decreases especially with no clear symptoms and with only borderline elevated tumor markers. We present a case of a suspected NET, which was initially diagnosed as a metastatic NET by virtue of a positive 68Ga-DOTATATE PET scan; however, on biopsy it was revealed to be a squamous cell carcinoma originating from the head and neck.
Background
Neuroendocrine tumors (NETs) are thought to be a rare entity; however, with improved diagnostic parameters, the incidence and prevalence of these cases are increasing. 1 These tumors arise from the neuroendocrine cells and most commonly occur in the gastrointestinal tract, lung, and pancreas although they can appear in various organs within the body. 2 NETs are best known for their ability to secrete bioactive peptides causing symptoms like diarrhea and flushing; however, the majority of NETs do not secrete hormones and have non-specific symptoms. 3 Due to low incidence, nonspecific symptoms, and variable organ involvement, delays in the diagnosis of NETs are frequent. 4 Biochemical testing with chromogranin-A, imaging with computed tomography and magnetic resonance imaging scans, along with the help of functional imaging like the somatostatin receptor (SSTR) scintigraphy, which takes advantage of the overexpression of the SSTRs and positron emission tomography (PET) scan using radiolabeled somatostatin analogues like the 68Ga-DOTATATE help in the diagnosis of NETs. 68Ga-PET DOTATATE have high sensitivity and specificity for the diagnosis of suspected NET. In this article, we present a case of a suspected NET, which was initially diagnosed as a metastatic NET by virtue of a positive 68Ga-DOTATATE PET scan; however, on biopsy it was revealed to be a squamous cell carcinoma originating from the head and neck.
Case Description
A 70-year-old man with a past medical history of coronary artery disease, hypertension, hyperlipidemia, obstructive sleep apnea, and remote history of renal cell carcinoma with prior radical nephrectomy. During a surveillance scan for his prior renal cell carcinoma, an incidental pulmonary embolism was noted as well as a cystic lesion on the pancreas. He was referred to gastroenterology for further workup of the pancreatic cystic lesion. As part of the assessment, a chromogranin-A level was obtained. Chromogranin-A was elevated at >600 ng/mL with normal 5-hydroxyindoleacetic acid. Octreotide scan was negative and endoscopic ultrasound was negative for any solid component of the pancreatic lesion. It was postulated that the patient had elevated chromogranin-A levels related to his chronic kidney disease, recent thrombosis as well as being on a proton pump inhibitor (PPI). The patient was asymptomatic from the pancreatic lesion without complaints of diarrhea or flushing. A repeat chromogranin-A level a few months later decreased to 157 ng/mL after PPI was held but remained elevated beyond the upper limit of normal. Over the next several years he continued surveillance for the pancreatic cyst and elevated chromogranin-A level. On surveillance scans he was noted to have an increase in the size of cystic lesions on the pancreas as well as a peripancreatic lymph node enlargement. The chromogranin-A rose to 400 ng/mL.
After nearly 5 years of surveillance, a 68Ga-DOTATATE PET scan was obtained for a suspected NET. This showed an abnormal bifocal uptake in the left neck with a maximum SUV (standardized uptake value) 9, with an additional focus of abnormal uptake in the left neck more medially with a maximum SUV 7. Another abnormal focus of uptake was also appreciated in the right neck with maximum SUV 3.1 (Figures 1 and 2). Due to a high suspicion for metastatic NET, the patient was referred to a medical oncology specialist in gastrointestinal cancers. The patient was thought to have metastatic NET based on laboratory tests and imaging. He was sent for a biopsy of the lymph node for confirmation. To much surprise, the abnormal area on 68Ga-DOTATATE PET scan showed squamous cell carcinoma on a core biopsy. ENT evaluation showed a left tonsillar primary lesion. The patient was referred to a head and neck oncology specialist and was not found to have any evidence of a NET.

Coronal maximal intensity projection (MIP) image from patient’s Ga-68 DOTATATE PET magnetic resonance imaging scan demonstrates abnormal foci of radiotracer uptake in the left neck in the left palatine tonsil medially and left cervical lymph node chain laterally (long white arrow). Subtle increased focus of radiotracer uptake also visualized in the right cervical lymph node chain (short white arrow). Physiologic radiotracer uptake is seen elsewhere in the body, with absence of the right kidney.
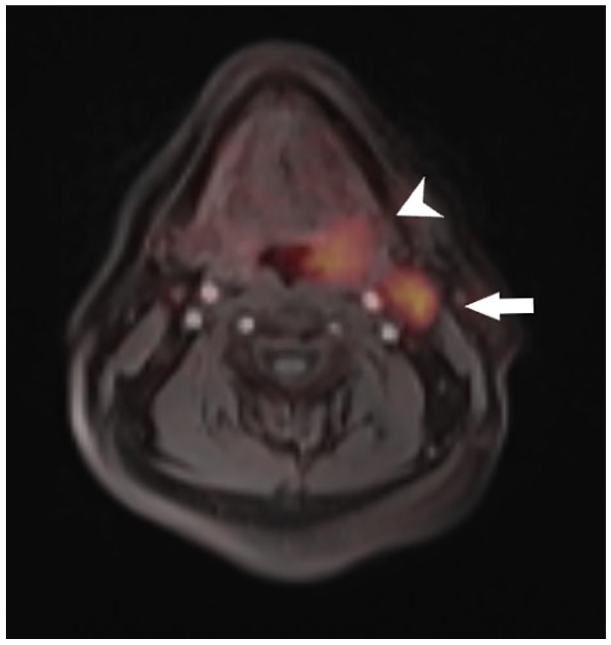
Axial fused DOTATATE PET magnetic resonance imaging image demonstrates asymmetrically increased radiotracer uptake in the left palatine tonsil measuring up to 3.1 cm (short white arrow) and left cervical lymph node chain (long white arrow), with largest cervical lymph node measuring up to 2 cm in the short axis.
Discussion
NETs encompass a group of neoplasms that are very rare. These tumors express SSTR, a defining characteristic of NETs. 5 A combination of clinical signs and symptoms such as diarrhea, flushing, and laboratory test results showing elevated chromogranin-A provides a diagnostic sensitivity approaching 70% to 85%. 6 However, it is not sufficient for the identification of tumor sites and it is not specific as false-positive chromogranin-A elevations are common with conditions such as atrophic gastritis, renal insufficiency, heart failure, usage of PPI, and gastrointestinal disorders. 6 Previously, octreotide scans, using a long-acting somatostatin analogue, were used in the evaluation and diagnosis of NETs.7,8 However, there were many limiting factors which led to the low specificity of the test such as low image quality, increased physiological uptake restricting detection of smaller lesions, prolonged imaging protocol, and high-dose radiation.9-12
With the availability of 68Ga-DOTATATE PET using radioisotope-labeled somatostatin analogues, the diagnosis of SSTR expressing tumors like NETs has dramatically improved and shown a higher specificity.13,14 In addition to improvement in the spatial resolution, lesion detectability, it is also more convenient as the test takes about 2 hours rather than 2 days and has less radiation exposure compared with the octreotide scan.13,15-17 Multiple authors evaluated the role of 68Ga- DOTATATE PET in diagnosis of suspected primary or metastatic NETs and correlated with gold standard pathology results.18-20 The sensitivity of the 68Ga-DOTATATE PET in the diagnosis of NETs is 80% to 90% and the specificity is 82% to 90% compared with the pathology. 14 However, the specificity is found to be low with high false positives in patients with no clear clinical symptoms or borderline elevated tumor markers. 19
SSTRs are highly expressed in NETs including the pituitary adenoma, endocrine pancreatic tumors, carcinoid of the gastrointestinal tract and lung, small cell cancer but are also present in non-NETs of the prostate, breast, lung, brain tumors, and so on. 21 Interestingly, studies have shown SSTR expression in squamous cell carcinoma of the lung, head, and neck.22-24 Currently, the pathophysiologic role of the SSTR expression in squamous cell carcinoma is unclear. Due to expression of the SSTR in other cancers, there may be a false positive result for a NET. It is therefore very important to follow the gold standard and obtain a biopsy to establish the final diagnosis.
In our case, in which the patient had no clear clinical symptoms, and the abnormal elevation and a fluctuation of chromogranin-A could be explained by other factors, the specificity of 68Ga-DOTATATE PET becomes low. Clinicians need to be aware of sensitivity and specificity of each test and cautiously interpret the results.
Conclusion
68Ga-DOTATATE PET scan has high specificity for detecting NETs. The specificity decreases with high false positives in patients with who have no clear clinical symptoms of NETs or have only borderline elevated tumor markers such as chromogranin-A. Tumors not classically thought to have high expression of SSTRs may show positive findings on 68Ga-DOTATATE PET and providers cannot use 68Ga-DOTATATE PET scan only to make diagnostic conclusions. A tissue biopsy should always be pursued to confirm the diagnosis.
Footnotes
Author Contributions
Sanjana Mullangi: Conception of the idea, acquisition of data, manuscript writing, and final approval.
Manidhar Reddy Lekkala: Conception of the idea, critical revision, manuscript writing, and final approval.
Charumathi Raghu Subramanian: Conception of the idea, critical revision, and final approval.
Omar Nemer: Critical revision, manuscript writing, and final approval.
Jagmeet Singh: Critical revision, acquisition of data, and final approval.
Asim Kichloo: Critical revision, acquisition of data, and final approval.
Bahar Moftakhar: Conception of the idea, critical revision, manuscript writing, and final approval.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Verbal informed consent was obtained from the patient(s) for their anonymized information to be published in this article.