
Abstract
Penile squamous cell carcinoma is a rare diagnosis in the United States; however, the incidence is significantly higher in developing countries. This cancer is categorized into human papilloma virus (HPV)-associated and independent disease. In this article, we present a rare case of HPV-independent penile squamous cell carcinoma. Our patient was a 75-year-old Caucasian male who initially presented with a penile ulcer which was managed with partial penectomy and adjuvant chemotherapy. The patient was monitored on surveillance and did not pursue lymph node dissection. He was noted to have recurrence with metastatic disease 5 years after his initial presentation. Due to the aggressive nature of his disease, the patient was admitted to the hospital and treated with chemotherapy and immunotherapy.
Introduction
Penile squamous cell carcinoma (PSCC) is a rare diagnosis in the United States and accounts for approximately 0.4% to 0.6% of all malignancies in males in both the United States and Europe. 1 In 2020, the American Cancer Society estimated a total of 2200 new cases of penile cancer in the United States and 440 deaths. 2 Epidemiological studies have found that the incidence of penile cancer is significantly higher in developing countries, specifically in Asia and Africa. 3
Multiple prognostic markers have been studied over the past few decades; however, it has been shown that the main prognostic factors with respect to survival of patients with penile cancer is the presence and extent of lymph node involvement. Metastases in regional lymph nodes lead to a poor prognostic outcome. 4 The 5-year survival rate in patients without lymph node involvement is greater than 85%, 29% to 40% in patients with positive lymph nodes, and 0% for those with pelvic lymph node (PLN) involvement. 5
Classification of squamous cell carcinoma of the penis has recently changed and is now further classified into human papilloma virus (HPV)-associated and HPV-independent disease. 6 The prevalence of HPV-associated penile cancer is approximately 50%, with the most commonly associated type being HPV16, followed by HPV6 and HPV18, respectively. Human papilloma virus–associated penile cancer was also found to have a high percentage of p16 positivity (79.6%) compared to 18.5% p16 positivity in HPV-independent SCC of the penis. 7 Studies have shown that men with p16-positive or HPV-associated penile cancer have a significantly better disease-specific survival than p16-negative or HPV-independent penile cancer. 8 It is still not entirely clear why this is the case, but it has been speculated that HPV-associated cancers may promote increased immune surveillance, thus making it a less-aggressive cancer; however, further research needs to be conducted regarding these findings.
Penile squamous cell carcinoma is a rare malignancy to begin with, and unfortunately those with metastatic disease have limited treatment options. Platinum-based regimens have historically been used in this setting; however, patients who progress following initial chemotherapy tend to have a medial overall survival of less than 6 months. 9 Here, we present a patient who has a history of squamous cell carcinoma of the penis and presented with distant metastatic disease.
Case Presentation
This is a case of a 75-year-old male with no significant past medical history who had first noted to have a penile ulcer for which he underwent partial penectomy that showed poorly differentiated squamous cell carcinoma, pT3N3M0, 7 years prior to his hospital admission. The patient had palpable inguinal lymph nodes bilaterally with a positron emission tomography (PET) scan showing bilateral inguinal nodes and a 6-mm noncalcified pulmonary nodule not thought to be metastatic. The patient underwent bilateral superficial and deep bilateral inguinal debulking that showed metastatic poorly differentiated squamous cell carcinoma with the largest node measuring 2.4 cm with extracapsular extension. Immunohistochemistry showed that the tumor was positive for p63 and cytokeratin 5/6 and negative for GATA-3, cytokeratin 20, and uroplakin II. The patient underwent partial penectomy followed by bilateral inguinal lymph node debulking. He subsequently underwent adjuvant chemotherapy with TIP (paclitaxel, ifosfamide and cisplatin). He followed up with urology and decided against lymph node dissection (LND) and was being monitored with surveillance scans. The patient was continued on long-term surveillance due to opting against lymph node dissection. Five years after the initial diagnosis, his scans showed metabolically active nodes in the chest and abdomen on PET scan, and biopsy of a left infrahilar node showed poorly differentiated carcinoma with immunostains consistent with squamous cell carcinoma. The histopathology did show resemblance to the patient’s prior squamous cell carcinoma of the penis, and this lymph node was thought to represent metastatic disease from the patient’s prior cancer. However, the immunostain was also GATA-3 positive, which was not seen on the prior biopsy (Figure 1). The patient was found to have high tumor mutation burden (TMB) and was started on pembrolizumab.

(A) Hematoxylin and eosin, magnification 100×. Biopsy cores from the left infrahilar lymph node show metastatic poorly differentiated carcinoma. (B) Hematoxylin and eosin, magnification 400×. Intercellular bridging is seen focally between tumor cells. (C-G) Cytokeratin AE1/AE3, CK5/6, GATA-3, p40, and p63 immunostains, magnification 100×. The tumor cells are positive for cytokeratin AE1/AE3, CK5/6, and GATA-3. There is focal weak staining for p40 and p63.
Six months after the initiation of pembrolizumab, the patient presented to the emergency room with worsening shortness of breath and increased oxygen requirements. He underwent computed tomography angiography (CTA) of the thorax, which was negative for pulmonary embolism and showed large bilateral pleural effusions, cardiac/Aortopulmonary (AP) window region masses with mass effect on the left heart measuring 6.3 to 7.5 cm along with retroperitoneal and mediastinal masses (Figure 2). The patient subsequently underwent image-guided biopsy and fine needle aspiration (FNA) of mediastinal mass, which showed poorly differentiated carcinoma with morphology resembling left infrahilar lymph node biopsy performed 2 years ago, consistent with metastatic carcinoma of penile primary (Figure 3). Pathology showed sheets and clusters of cells with pleomorphic nuclei and foci of intercellular bridges. P63 and p16 were negative. The patient underwent left-sided thoracocentesis, and fluid studies were performed, which showed a borderline exudative effusion. Cytology of the pleural fluid showed malignant cells similar in morphology to the mediastinal biopsy.

Computed tomographic angiography of the thorax in the axial (top row), coronal (bottom left), and sagittal (bottom right) planes. The enlarged aortopulmonary lymph node is visualized measuring 3.5 cm in the greatest transverse diameter. A large, isodense mass of the pericardial space is visualized with central calcifications and necrosis. There is encasement of the left atrium/ventricle and left main pulmonary artery and its segmental branches. No atrial appendage or pulmonary artery compression is visualized. Airspace opacities are visualized in the inferior portion of the left upper lobe with surrounding large left-sided pleural effusion.

(A) Hematoxylin and eosin, magnification 100×. Biopsy cores from the mediastinal mass show metastatic poorly differentiated carcinoma. (B) Hematoxylin and eosin, magnification 400×. Intercellular bridging is seen focally between tumor cells.
Oncology was consulted, and the patient was started on inpatient chemotherapy with paclitaxel and carboplatin given high tumor burden. Unfortunately, the patient had rapid accumulation of his pleural effusions and required pleurodesis. His functional status continued to decline while being an inpatient along with the chemotherapy side effects; therefore, further cycles of chemotherapy were held. Radiation oncology was consulted, given continued symptoms from the mediastinal mass, and the patient underwent 10 fractions of radiation treatment. Given his high TMB and declining performance status, the decision was made to try nivolumab. Repeat CT scans showed some improvement of metastatic disease following the initiation of treatment; however, the patient continued to deteriorate and unfortunately passed away during the hospitalization.
Discussion
We present a case of p16-negative metastatic PSCC in a 75-year-old male. Our patient was first diagnosed 7 years prior to presentation to our hospital and had PLN involvement, a poor prognostic indicator in this disease.
Squamous cell carcinoma of the penis is a rare disease in the United States, representing less than 1% of all male cancers, although it is more prevalent in other areas of the world. Squamous cell carcinoma is most commonly diagnosed in elderly patients, but prevalence in patients younger than 50 years is increasing. 10 Squamous cell carcinoma can be further characterized by the presence or absence of p16 positivity. Two different pathogenic pathways exist for the development of penile carcinoma. The first is through HPV-associated infection, and the second is chronic inflammation secondary to phimosis or lichen sclerosis. 11 Chronic cigarette smoking has also been shown to increase the risk of developing PSCC. 11 Our patient’s pathology was reported as p16 negative, which has been shown to be associated with poorer outcomes. 8
The clinical presentation of penile cancer often involves a patient noticing a mass on the penis or a change in the color of the glans. Patients may also describe painless lymphadenopathy. Due to patient-related factors regarding the perception of the disease, the diagnosis of penile cancer may often be delayed. However, early suspicion and biopsy are necessary to avoid delays in diagnosis and treatment as this may significantly increase mortality. 11
The diagnosis of penile cancer requires a biopsy, and the disease is classified based on the tumor-node-metastasis staging classification (Figure 4). Once the diagnosis is made histopathologically, it is important to assess the extent of the tumor growth and spread. Figure 4 shows a table from the American Cancer Society that outlines the Tumor, Node, Metastases (TNM) staging for penile cancer. In our patient’s case, he had mediastinal mass metastasis along with bilateral inguinal lymph nodes and an infrahilar lymph node with similar immunohistology to his prior PSCC metastases; therefore, he would be categorized as stage IV disease patient by virtue of distant spread of metastases.
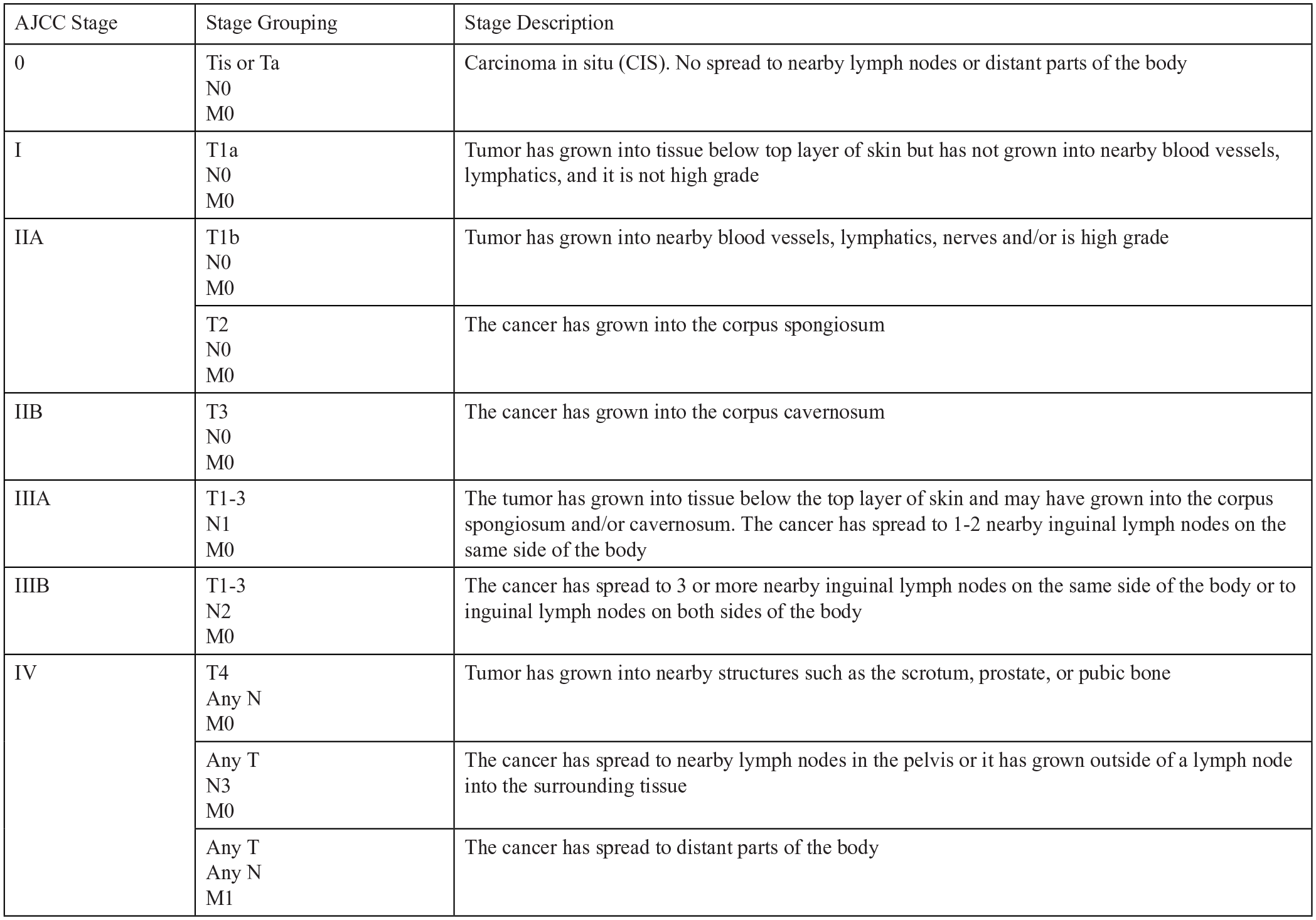
TNM staging for penile cancer.
The landscape for the management of penile cancer has changed significantly over the years. In the past, penile cancer was managed with aggressive radical surgery; however, this carried a significant morbidity burden to the patient. 12 Early-stage superficial disease can be treated with focal chemotherapy or immunotherapy, laser ablation, radiation therapy, or surgery. 11 Guidelines for surgical treatment have been modified to allow a smaller negative margin to improve organ preservation.
Patients with higher stage extensive disease may need partial or radical penectomy, as in our patient’s case. The National Comprehensive Cancer Network (NCCN) consensus guidelines for penile cancer recommend neoadjuvant chemotherapy prior to lymph node dissection in patients with inguinal lymph nodes larger than 4 cm. 1 Our patient was initially treated with the TIP regimen per NCCN guidelines. 1 Our patient was then recommended to have surgical PLN dissection; however, he declined and was monitored with surveillance CT scans. Five years after receiving chemotherapy, the patient was found to have disease recurrence on PET scan, with metabolic activity demonstrated in lymph nodes in the thorax and the abdomen. He underwent a biopsy of a left infrahilar lymph node which was consistent with metastatic carcinoma. His tumor was sent for foundation-1 study testing and showed a high TMB at 68 Muts/Mb; therefore, he was started on pembrolizumab. A recent study evaluated the impact of HPV status on immune checkpoint inhibitor-related biomarkers and found that patients with HPV-associated PSCC have distinct molecular genetic tumors compared with HPV-independent tumors. 13 Interestingly, the results showed that a high TMB was exclusive to HPV-associated tumors, which was not the case with our patient. Further studies are required for follow-up with a larger sample size.
5-Fluorouracil, combined with cisplatin, has historically been used for metastatic penile cancer, but this regimen’s toxicities have been limiting. There is no current consensus for subsequent line systemic therapy, and the NCCN recommends either clinical trial or treatment with pembrolizumab if the patient has a microsatellite instability–high (MSI-H) or mismatch repair deficient (dMMR) tumor that has progressed on initial treatment or if the TMB is high. 1
Penile squamous cell carcinoma is a rare disease which may develop from HPV-associated infection or through chronic inflammation. The marker p16 is important for prognostic factors, with a p16-negative status having poorer prognosis. Treatment may include surgery with neoadjuvant chemotherapy. In cases of metastatic PSCC, treatment with chemotherapy and immunotherapy may be employed, but prognosis remains poor.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Informed consent for patient information to be published in this article was obtained from the patient’s family.