
Abstract
Squamous cell carcinoma (SCC) of the lung, a subtype of nonsmall cell lung cancer (NSCLC), uncommonly causes pericardial effusion. Pericardial effusions occur in 10% to 12% of lung cancer cases but are rarely the initial presentation. We report a case of a 68-year-old male with type II diabetes mellitus and chronic obstructive pulmonary disease who presented with right upper quadrant pain, dyspnea, and anorexia, suspicious of hepatobiliary disease. Imaging incidentally revealed a large pericardial effusion causing cardiac tamponade. Cytology of pericardial fluid identified malignancy, and biopsy of a mass found on subsequent chest computerized tomography diagnosed SCC of the lung. The patient experienced respiratory failure accompanied by bilateral pneumothorax, leading to the decision to initiate hospice care. Pericardial effusion warrants prompt echocardiography and pericardiocentesis with cytology. NSCLC-related effusions signify stage IV disease, managed palliatively with immunotherapy and chemotherapy. This case emphasizes the critical importance of evaluating pericardial effusions for malignancy, even in instances where the presentation may be atypical. We present a case of malignant cardiac tamponade that was obscured by underlying hepatobiliary disease. Maintaining a high level of suspicion for malignant effusions is essential, as failure to do so may lead to increased morbidity in patients with undiagnosed malignancies.
Keywords
Introduction
Lung cancer is the second most common cancer, with an estimated 234 580 new cases and 125 070 deaths in 2024. 1 Lung cancer is further categorized as small cell carcinoma or nonsmall cell carcinoma. Squamous cell carcinoma (SCC) of the lung, a type of nonsmall cell lung cancer (NSCLC), commonly presents with cough, dyspnea, and hemoptysis. Pericardial effusions from lung cancer are relatively common, with a prevalence of 10% to 12% at autopsy. 2 However, SCC, which prefers the central airways3,4 seldom initially presents as a pericardial effusion, as seen in only a few case reports.3,5 Pericardial effusions generally represent end-stage disease and often go undiagnosed as they may remain asymptomatic. 6
Pericardial effusions can progress to cardiac tamponade, which classically presents as Beck’s triad of hypotension, jugular venous distension, and muffled heart sounds. 7 The emergence of cardiac tamponade is often how metastatic pericardial effusions are diagnosed; however, it is a late-stage finding with a poor prognosis. 8 This is potentially due to the hemodynamic compromise; therefore, early and repeated treatment is often indicated, though conservative management may be appropriate in select cases of patients with limited life expectancy. 9 We present a case of a patient initially presented with hepatobiliary disease, which led to the finding of a cardiac tamponade secondary to SCC. We elucidate the clinical presentation and management of this atypical presentation.
Case Presentation
A 68-year-old male with a history of type II diabetes mellitus and chronic obstructive pulmonary disease presented to the emergency department with right upper quadrant abdominal pain, lethargy, nausea, and anorexia. Initial laboratory findings showed leukocytosis (19 000/cm²), elevated liver enzymes – Aspartate Aminotransferase (AST) of 916 U/L, Alanine Aminotransferase (ALT) of 1616 U/L, total bilirubin 3.2 mg/dL, lipase 537 U/L, and lactic acid 4.4 mmol/L, consistent with pancreatitis, and mixed hepatocellular/cholestatic disease. Imaging with right upper quadrant ultrasound revealed cholelithiasis, choledocholithiasis, gallbladder wall thickening, and pericholecystic fluid, concerning acute cholecystitis. Computerized tomography of the abdomen was performed to evaluate for gastrointestinal tract complications, and a large pericardial effusion was incidentally identified.
Echocardiography confirmed a large-volume pericardial effusion with right ventricular diastolic collapse, consistent with cardiac tamponade. Electrocardiogram findings of low-voltage QRS complexes and right axis deviation supported this diagnosis. Pericardiocentesis was performed, draining hemorrhagic fluid, and a pericardial drain was placed. Cytology (Figure 1) of the pericardial fluid revealed malignant epithelial cells (Ber-EP4 positive) with a background of mesothelium (calretinin positive), suspicious of malignancy. Immuno-histochemistry performed on the cell block was cytokeratin 7 positive and thyroid transcription factor-1 negative, confirming the SCC.
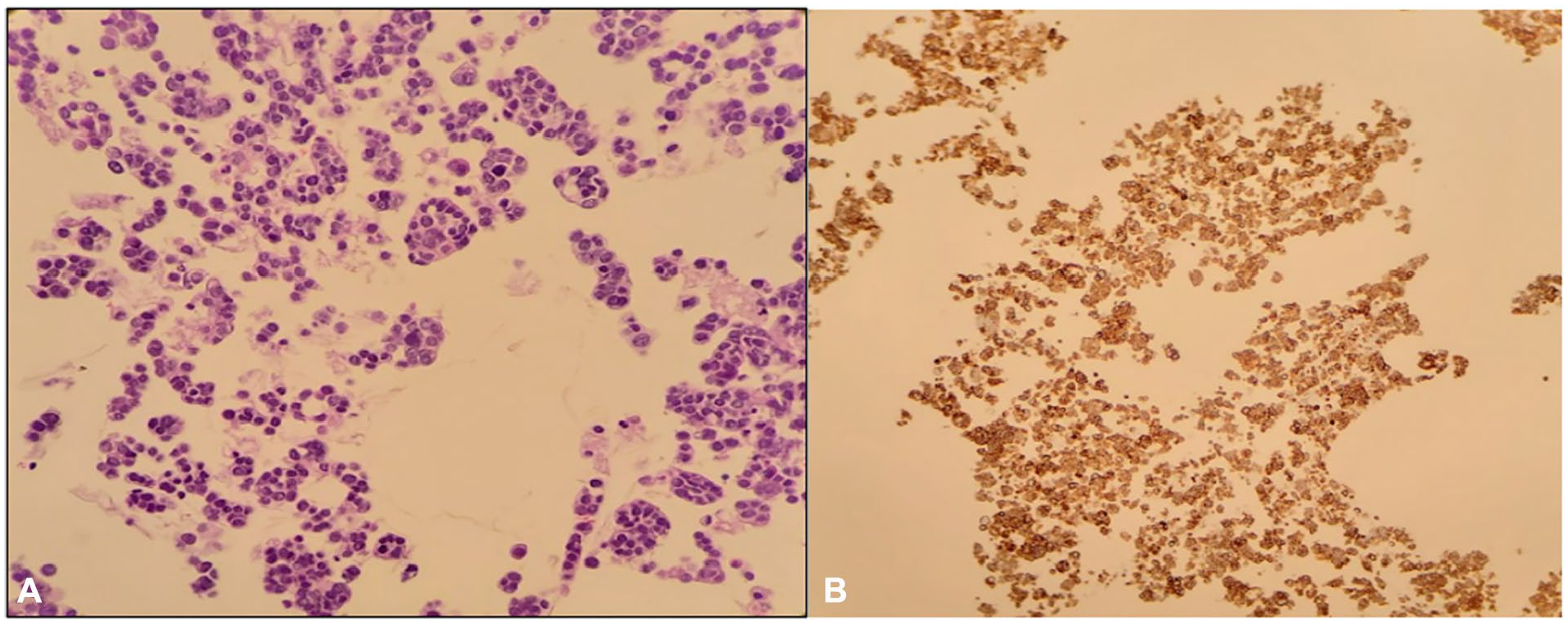
Photomicrograph of histopathologic specimen of pericardial fluid. (A) H&E, 400× consists of a few clusters of malignant epithelial cells. (B) Positive immunohistochemical stain for CK7, consistent with metastatic carcinoma. CK7, cytokeratin 7; H&E, hematoxylin-eosin.
Subsequent chest computerized tomography identified a mass-like infiltrate in the right upper lobe, mediastinal lymphadenopathy, and bilateral pleural effusions. Transbronchial biopsy (Figures 2 and 3) confirmed SCC of the lung. Further staging revealed cerebellar metastases, which were managed with whole-brain radiation.
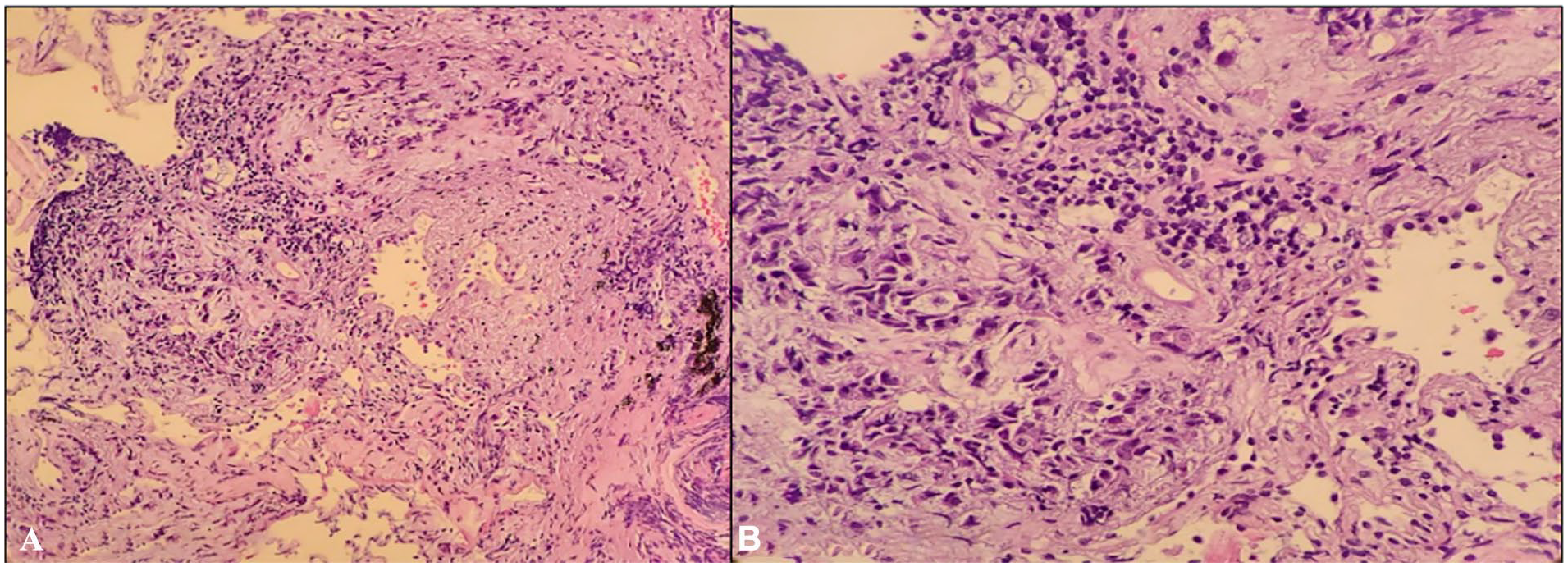
Histopathologic evaluation of the right upper lobe lung biopsy (transbronchial approach). (A) H&E stain at 200× magnification shows tumor nests and keratinization, consistent with squamous cell carcinoma. (B) Higher magnification (400×) confirms the presence of malignant squamous cells with intercellular bridges and keratin pearls. H&E, hematoxylin-eosin.

Immunohistochemical characterization of right upper lobe lung biopsy. (A) Tumor cells demonstrate diffuse nuclear positivity for p40, supporting squamous differentiation. (B) CK7 is positive in rare tumor cells. (C) TTF-1 is negative. These findings support the diagnosis of primary squamous cell carcinoma of the lung. CK7, cytokeratin 7; TTF-1, thyroid transcription factor-1.
During subsequent hospitalization, the patient developed acute-on-chronic respiratory failure, likely due to volume overload, hospital-acquired pneumonia, and pleural effusion-induced atelectasis. The patient was started on average volume-assured pressure support, but his condition continued to decline despite aggressive diuresis and broad-spectrum antibiotics. Repeat imaging revealed bilateral pneumothorax and segmental lung collapse. The patient elected for hospice care following the goals of care discussion. The patient was transitioned to comfort care and passed away under hospice support.
Discussion
Pericardial effusion occurs relatively frequently due to lung malignancy, 2 often presenting in the advanced stages of the disease, but it is rarely the initial presentation of SCC of the lung.3,5,10-13 Furthermore, the prognosis of malignant pericardial effusion is poor, with mean survival after diagnosis reported at 3 months. 9 Recurrence occurs in up to 90% of cases in the setting of NSCLC, 9 and progression to cardiac tamponade is common. Cardiac tamponade is a medical emergency with a 75% 12-month mortality. 2 Diagnosing tamponade in patients with multiple comorbidities, as in our case, can be challenging. Features of cardiac tamponade—hypotension, jugular venous distension, and muffled heart sounds (Beck’s triad) 7 —are often masked by overlapping symptoms of underlying illnesses.
It is rare for pericardial effusion to be a presenting feature of SCC. In large series of pericardial effusions, metastatic SCC accounts for a small minority of malignant pericardial effusions, with bronchogenic (lung) SCC being the most common source when it does occur. For example, in a 15-year review of 251 pericardial effusions, only 4 cases (about 1.6%) were due to metastatic SCC, all from a bronchogenic primary. Similarly, pericardial involvement from head and neck SCC is described as a rare event, with only isolated case reports documenting such presentations.14-16 The majority of malignant pericardial effusions are associated with adenocarcinomas of the lung, breast cancer, and hematologic malignancies, while squamous cell histology is distinctly uncommon as an etiology.3,17-19
Our case presents an unusual presentation—an incidental finding of cardiac tamponade while working up hepatobiliary disease leading to a NSCLC diagnosis. All patients with findings of pericardial effusion should undergo an echocardiogram to identify the degree of the effusion and structural or hemodynamic compromise triggered by the fluid collection. 20 Furthermore, pericardiocentesis with cytology is crucial to determine the characteristics of the effusion.21,22
Acute treatment of malignant effusion and cardiac tamponade includes fluid drainage or formation of a pericardial window if recurrent. 23 However, treatment should be guided by the clinical picture. In this case, given the patient’s extensive metastatic disease and poor functional status, therapeutic interventions were not pursued. Instead, the management shifted toward palliative care, which aligned with the patient’s preference and addressed the clinical futility of aggressive treatment. 24 This management strategy is supported by the fact that NSCLC metastasis to the pericardium indicates stage IV disease; standard management recommendations are all palliative in nature.25-28 A common regimen used, for example, is pembrolizumab (immunotherapy), carboplatin, and paclitaxel (chemotherapy).29,30 It is important to note that these regimens are generally not started in an inpatient setting. The rationale for this is that oncologic pharmacotherapy is not usually started until underlying medical conditions, for example, sepsis, tamponade, or respiratory failure, as in our patient, are controlled.30-32
This case provides several teaching points. First, clinicians should consider malignancy in all cases of pericardial effusion, regardless of other symptoms. Early use of diagnostic tools, such as echocardiography and cytologic analysis of pericardial fluid, is crucial in identifying malignant etiologies. Second, this case highlights the complexity of diagnosis and management of cardiac tamponade in patients with multiple comorbidities, where symptoms can mimic other conditions. Finally, this case underscores the importance of individualized patient care, balancing the benefits of aggressive interventions against quality-of-life considerations and patient preferences. Efficient diagnosis can lead to prompt management of malignant cardiac tamponade and its complications. Although complete remission is improbable, early pharmacologic palliation can improve patients’ quality of life.
Conclusion
This case highlights how an unexpected finding can completely change a diagnosis and treatment plan. What started as a workup for suspected hepatobiliary disease revealed a life-threatening cardiac tamponade caused by metastatic NSCLC. It’s a powerful reminder of how critical it is to keep an open mind and consider malignancy when evaluating pericardial effusion, even in unusual clinical scenarios. Timely echocardiography, pericardiocentesis, and fluid analysis can make all the difference in recognizing malignant causes early. Ultimately, focusing on the patient’s goals and quality of life guided our decision to prioritize comfort care. This case emphasizes the need for thoughtful, individualized care that balances aggressive treatment options with what’s truly in the patient’s best interest.
Footnotes
Acknowledgements
We sincerely thank the Research Committee of the Internal Medicine Department, Marshall University, WV, for their invaluable support and guidance throughout the development of this manuscript.
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Consent for Publication
Verbal informed consent was obtained from the patient for their anonymized information to be published in this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.