
Abstract
Takotsubo cardiomyopathy (TC) is a syndrome characterized by acute and transient regional systolic myocardial dysfunction. TC often mimics myocardial infarction without obstructive coronary disease. We present a case of a 48-year-old woman who developed TC following the onset of polymorphic ventricular tachycardia in the setting of methadone intoxication.
History of Presentation
A 48-year-old woman with a past medical history of malnutrition, alcohol use disorder, and opiate use disorder (OUD), who was on a methadone maintenance program (30 mg/day), was brought to the emergency department for altered mental status after accidental methadone overdose. At the initial evaluation, the blood pressure was 90/60 mm Hg, and the heart rate was 120 beats per minute. The respiratory rate was 32 breaths per minute, and the oxygen saturation was 91% on 6 L of oxygen per minute by nasal cannula. The temperature was 37 °C. Laboratory investigations demonstrated normocytic normochromic anemia with hemoglobin of 7.5 g/dL. She had normal renal and liver functions except for a low albumin level of <1.5 g/dL. High sensitivity troponin-I level was elevated at 135 ng/L. The electrocardiogram (ECG) showed sinus tachycardia with corrected QT (QTc) prolongation to 638 ms (Figure 1). The patient was intubated and admitted to the intensive care unit (ICU) due to hypoxic hypercapnic respiratory failure that did not respond to naloxone therapy. Her cardiac rhythm then transformed into sinus bradycardia with polymorphic ventricular tachycardia (PMVT; Torsade de pointes [TdP]), which lasted for 3 minutes (Figure 2). The patient received magnesium infusion to abort the PMVT and isoproterenol infusion to keep the heart rate above 100 beats per minute, aiming to shorten the QT interval and to avoid PMVT recurrence. Transthoracic echocardiogram (TTE) was performed to exclude underlying structural heart disease. TTE showed a newly reduced ejection fraction (EF) of 20% to 25% with mid to apical segments severe hypokinesis (Supplementary Video 1, available online). Contractility was relatively preserved in the basal segments. The distribution of regional dysfunction raised suspicion of TC. However, no obstructive coronary lesions were seen on the angiography (Figure 3). Over the next 3 weeks, the patient continued to have bradycardia and prolonged QTc interval, likely due to slow methadone clearance given the history of malnutrition and underlying hepatic dysfunction. Therefore, permanent pacemaker insertion was needed. However, due to the underlying poor nutritional status and debility, there was a concern about poor wound healing with increased risk of skin erosion and infection with any subcutaneous device. Therefore, the Micra leadless transcatheter pacemaker (Medtronic Inc) was a suitable device in her situation (Figure 4). 1

The electrocardiogram (ECG) showed sinus tachycardia with corrected QT (QTc) prolongation to 638 ms.

Telemetry monitor showing the polymorphic ventricular tachycardia.
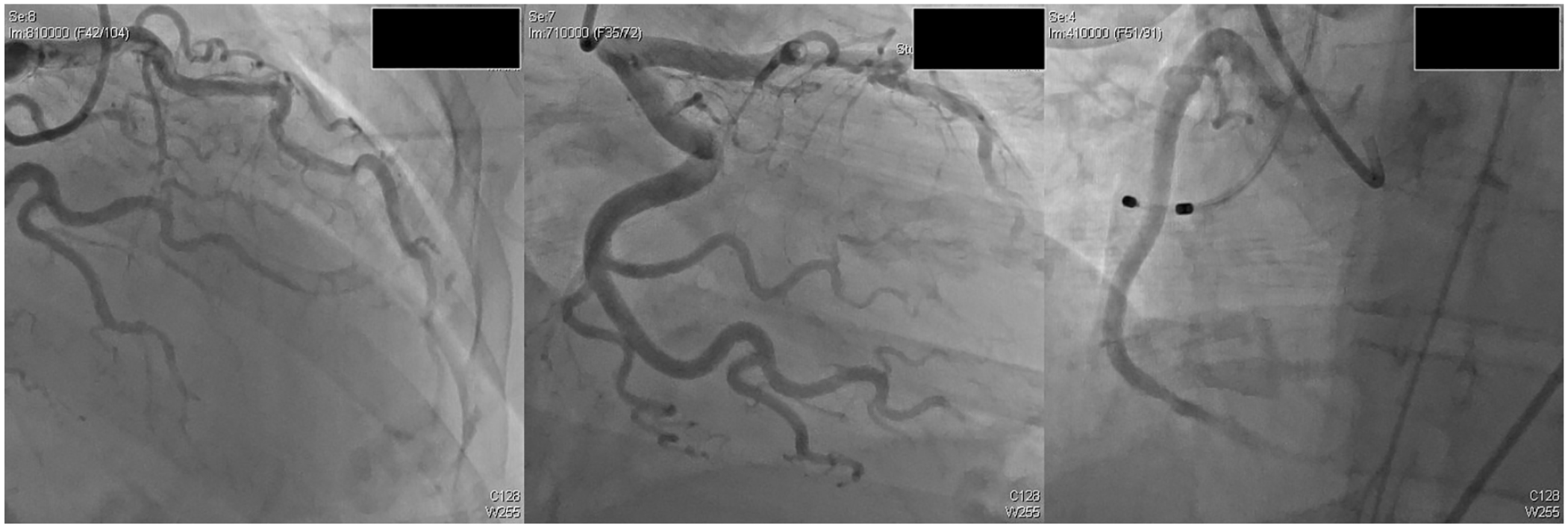
The patient coronary angiography showing no obstructive coronary lesions.

Micra pacemaker placement.
Discussion
Methadone is a synthetic long-acting µ-opioid receptor agonist that prevents opiate withdrawal symptoms. 2 Unfortunately, the increased methadone use for OUD has coincided with a significant increase in adverse events, including cardiotoxicity. 2 Methadone can prolong the QT interval by blocking the cardiac IKr potassium channel encoded by the HERG gene. 3 Furthermore, methadone can cause QT prolongation through a negative chronotropic effect. 2 Therefore, it increases the risk of TdP and sudden death. We present a case of patients on methadone maintenance therapy who developed bradycardia-mediated TdP complicated by TC after accidental methadone overdose.
Our patient has multiple factors that increased her risk of methadone-induced TdP, including the following:
Accidental administration of a higher methadone dose 4
Impaired hepatic methadone metabolism with alcohol use disorder and malnutrition
Marked QTc prolongation >500 ms 4
Female sex 4
Patients with multiple risk factors usually pose a greater TdP risk. 4 Interestingly, the most frequent risk factor for drug-induced TdP is female sex. 5 Compared with males, females have a longer baseline QTc and higher sensitivity to drugs that block the IKr potassium channel. Therefore, females have a lower threshold for developing TdP. 6 The higher sensitivity to the IKr blockers may be mediated by the effect of estrogen on IKr channel expression. 6 Furthermore, estrogen enchases QT prolongation induced by bradycardia and the development of TdP. 6
The association of ventricular arrhythmias with TC was reported in 4% to 9% of TC cases.7,8 Nevertheless, there has always been an ongoing discussion on whether TC is the cause or effect of ventricular arrhythmia in light of cases reported where there was TC evolution after discrete episodes of ventricular tachyarrhythmia. 7 Akashi et al 9 reported a patient presented with recurrent syncope with no other cardiac history and was found to have a PMVT. TC was demonstrated on TTE after PMVT was documented, 6 hours after admission. Tsuchihashi et al 10 conducted a retrospective analysis of 88 cases with TC for the years 1991 to 2000, and only one case was hypothesized to be secondary to ventricular tachycardia.
While it is difficult to conclusively establish causation ex post facto, several factors support PMVT as a possible inciting factor. Our patient presented with a marked QTc prolongation of 638 ms without any other ECG changes suggestive of TC like ST-segment depression, or deep and widespread T-wave inversion. 8 Subsequently, she developed bradycardia-mediated TdP, which can be explained in the view of the long-term methadone maintenance therapy, the accidental overdose, and the previously mentioned TdP risk factors. Therefore, TC might have been induced by altered catecholamine dynamics after the occurrence of PMVT. In support of this are reported autonomic changes induced during defibrillation threshold testing, ventricular fibrillation, and ablation of AV node reentry tachycardia. 7 Furthermore, as our therapeutic interventions (pacing and magnesium infusion) prevented any further PMVT, the patient EF reverted to normal.
However, the fact that our patient has developed TC could have contributed to the prolonged duration of QT prolongation and increased her risk of developing further episodes of TdP. The electrocardiographic changes that accompany TC are often associated with the prolongation of the QT interval. Furthermore, TdP complicating TC is observed in the setting of QT interval prolongation >500 ms. Therefore, our team was in favor of permeant pacemaker insertion to protect against bradycardia-mediated QT prolongation and TdP.
Follow-up
Two weeks after the Micra pacemaker placement, the patient continued to improve, and the repeated TTE showed EF of 65% to 70% with a resolution of the regional wall motion abnormality (Supplementary Video 2, available online).
Conclusion
When a young female with OUD presents with TdP, followed by a new regional wall motion abnormality on echocardiogram, the differential diagnosis needs to include TC. Given the significant population of OUD patients that are on methadone maintenance, clinicians should be aware of this complication in patients coming to the emergency room presenting with an overdose.
Supplemental Material
sj-docx-1-hic-10.1177_23247096211005100 – Supplemental material for Methadone-Induced Polymorphic Ventricular Tachycardia Complicated by Takotsubo Cardiomyopathy in a Malnourished Patient
Supplemental material, sj-docx-1-hic-10.1177_23247096211005100 for Methadone-Induced Polymorphic Ventricular Tachycardia Complicated by Takotsubo Cardiomyopathy in a Malnourished Patient by Mohammed Ali, Omeralfaroug Adam, Ahmed Subahi, Abdalaziz Awadelkarim, Lubna Fatiwala, Manmeet M. Singh, Rashid Alhusain and Randy Lieberman in Journal of Investigative Medicine High Impact Case Reports
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Verbal informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.