
Abstract
Aim:
The aim of this study was to evaluate the influence of dentin surface preparation with coarse diamond, extra-fine diamond, and polishing discs on the shear bond strength (SBS) of two resin cements (RCs) to dentin.
Materials and Methods:
Sixty-six recently extracted human mandibular third molar teeth that were free of cracks, caries, or restorations were collected. Sixty teeth were used for the SBS test. The occlusal part of the crowns was cut to expose mid-coronal dentin. The teeth were divided into three dentin preparation groups: coarse diamond (Meisinger, Germany), extra-fine diamond, and polishing discs (SofLex, 3MESPE, USA), and further conventional RC combined with a self-etch adhesive (Panavia F2.0/ED Primer II, Kuraray, Japan) or self-adhesive RC (Maxcem Elite, Kerr, USA) subgroups (n = 10). Sixty composite resin blocks were prepared (diameter: 3 mm, height: 4 mm) and bonded to the teeth according to the groups. The SBS test was performed with a universal testing device. Six teeth were used for the observation of prepared dentin surfaces and the resin–cement dentin interfaces using field emission scanning electron microscopy (Mira 3 XMU, Tescan). Statistical analyses were performed using the Mann–Whitney U and Kruskal–Wallis tests (P < .05).
Results:
Panavia F2.0/ED Primer II exhibited significantly higher SBS values for coarse and extra-fine diamond than for the polishing discs (P <.05). Regarding Maxcem Elite, no significant difference was observed for the preparation methods (P > .05). Panavia F2.0/ED Primer II had higher bond strength than Maxcem Elite for the dentin surface prepared with the coarse diamond (P <.05). The differences were not significant for the extra-fine diamond and the polishing disc groups (P > .05).
Conclusion:
The use of polishing discs did not increase the SBS of the RCs to the dentin.
Keywords
Introductıon
Recently, as a result of the advances in adhesive dentistry and computer-aided design/computer-aided manufacturing technology, resin cements (RCs) have become more widely used, especially for luting the various types of indirect prosthetic restorations (inlays, onlays, laminate veneers, full ceramic crowns, and bridges) or fiber posts with enhanced bond strength, mechanical properties, and aesthetic features. The first developed RC systems called “conventional RCs” were composed of adhesion agents and resin luting cement. According to the adhesive strategy used, these RCs were classified into two subgroups: etch and rinse or conventional RC combined with a self-etch adhesive. 1 However, the complexity and technique sensitivity of these multistep adhesive cementation protocols has been explicitly mentioned. 2
The technique’s sensitivity and the multistep application procedure of conventional RCs, increased the chair time and costs. For this reason, the uptake of RCs by clinicians was very slow at first. 3 Generally, clinicians prefer user-friendly materials, and ease of use is considered to promote enhancement in clinical performance. 4 Accordingly, self-adhesive RCs have been introduced by combining RCs and adhesive agents in a single material. 1 Although self-adhesive RCs are relatively new materials, they have attracted great interest and have quickly become popular because of their easy application procedure and the many commercial products that are available on the dental market. 5
Self-adhesive RCs are designed to directly adhere to the smear-covered dentin surface without any pretreatment procedure or the requirement of a separate adhesive or etchant application.6, 7 However, the RC–dentin interface is considered to be the weakest part of the adhesive structure. 1 Although the acidic monomer ingredients of self-adhesive RC are expected to dissolve the smear layer and react with the hydroxyapatite of dentin, there is an agreement that the smear layer demineralization or tag formation of self-adhesive RC is very limited.2, 3, 5, 8 Therefore, attention is focused on developing the most appropriate cavity or teeth preparation procedures. Consequently, the effect of the type and thickness of the smear layer on the adhesion and treatment methods of the smear layer has been a matter of many research projects.5, 6, 9–11 Previous studies have shown that treatment of the smear layer with various compounds differently affects the bond strength of the self-adhesive RC based on the pH, composition, and setting characteristics. 12
After the preparation with rotary instruments, the dentin surface is covered with a smear layer of up to 5 µm thickness, which consists of milled organic and inorganic dentin components. 13 The thickness of the smear layer varies depending on the bur type used and the size of the abrasive particles.5, 10 In addition to the smear thickness, the types of burs and other abrasives influence the surface roughness of the prepared dentin. Ren et al. 5 have reported that the bond strength of the self-adhesive RC increased with additional polishing application. However, no consensus is found for the clinical surface preparation protocol.
Therefore, the aim of this study was to evaluate the influence of the dentin surface preparation with coarse diamond, extra-fine diamond, and polishing disc on the shear bond strength (SBS) of two RCs (conventional RC combined with a self-etch adhesive and self-adhesive RC) to dentin. The null hypothesis is that the dentin surface preparation with different abrasives does not affect the SBS of the two different RCs.
Methods
Study Design, Setting, and Sample Size
This in vitro study was approved by the Tokat Gaziosmanpasa University Faculty of Medicine Ethics Committee with registration number 21-KAEK-154. The sample size was calculated considering 80% power and a significance level of 0.05 using data (effect size = 0.96) obtained from the study by Lührs et al. 14 Sixty samples (10 samples per subgroup) were required for the SBS test and six teeth were used for the observation of prepared dentin surfaces and the RC–dentin interfaces. Therefore, 66 recently extracted human mandibular third molar teeth that were free of cracks, caries, or restorations were collected, cleaned, and disinfected in 0.5% chloramine-T for 24 h and then stored in distilled water at 4°C up to six months after extraction.
Cylindrical Composite Resin Block (CRB) Preparation
A microhybrid composite resin (Solare X, GC Corp., Tokyo, Japan) was used for the preparation of the cylindrical CRBs (diameter: 3 mm, height: 4 mm) by inserting composite resin into a silicone mold. Sixty cylindrical resin composite blocks were built up in 2-mm increments and photo activated using an LED light-curing unit at 1000 mW/cm 2 (Valo; Ultradent Products Inc., South Jordan, UT, USA) at a constant distance of 2 mm from the surface. The bottom surfaces of the resin composite blocks were ground flat on a polishing machine (Forcipol 102, Metkon, Bursa, Turkey) with a 400-grit silicon carbide paper (for 5 s, at 200 rpm and at 10 N pressure) under a watercoolant.
Tooth Preparation
The teeth were embedded in a Teflon cylinder with self-cure acrylic resin from 2 mm below the cementoenamel junction. The occlusal part of the crowns was cut to expose the midcoronal dentin surface using a slow-speed diamond saw (Microcut 125 Precision Cutter, Metkon, Bursa, Turkey) under water cooling at 300 rpm. The dentin surfaces were examined under 3× magnification for the presence of enamel or the exposure of pulp tissue. Following that, the teeth were randomly divided into three groups (n = 20), according to the dentin preparation procedures: (a) coarse diamond (107–181 µm, no: 850 FG, Meisinger Dental Burs, Hager & Meisinger GmbH, Neuss, Germany) at high speed (200,000 rpm), (b) extra-fine diamond (10–36 µm, no: 850 FG, Meisinger Dental Burs, Hager & Meisinger GmbH) at high speed (200,000 rpm), and (c) polishing discs (SofLex, 3M ESPE, Seefeld, USA) from coarse-grit (80 µm) to superfine-grit (5 µm) at low-speed (10,000 rpm). All the surface preparation steps were performed by an experienced dentist. Five light strokes were performed with abrasives for the preparation of uniform dentin surfaces according to the method described by Saikaew et al. 15 After the surface preparation, the dentin surface was washed with water spray for 10 s, was blot-dried with paper points (leaving a moist surface), and adhesive cementation was performed immediately.
Adhesive Cementation
The teeth within each surface preparation group were divided into two further subgroups (n = 10) according to the RC used to bond the CRB. The CRBs were bonded to the center of the prepared dentin surfaces with RCs.
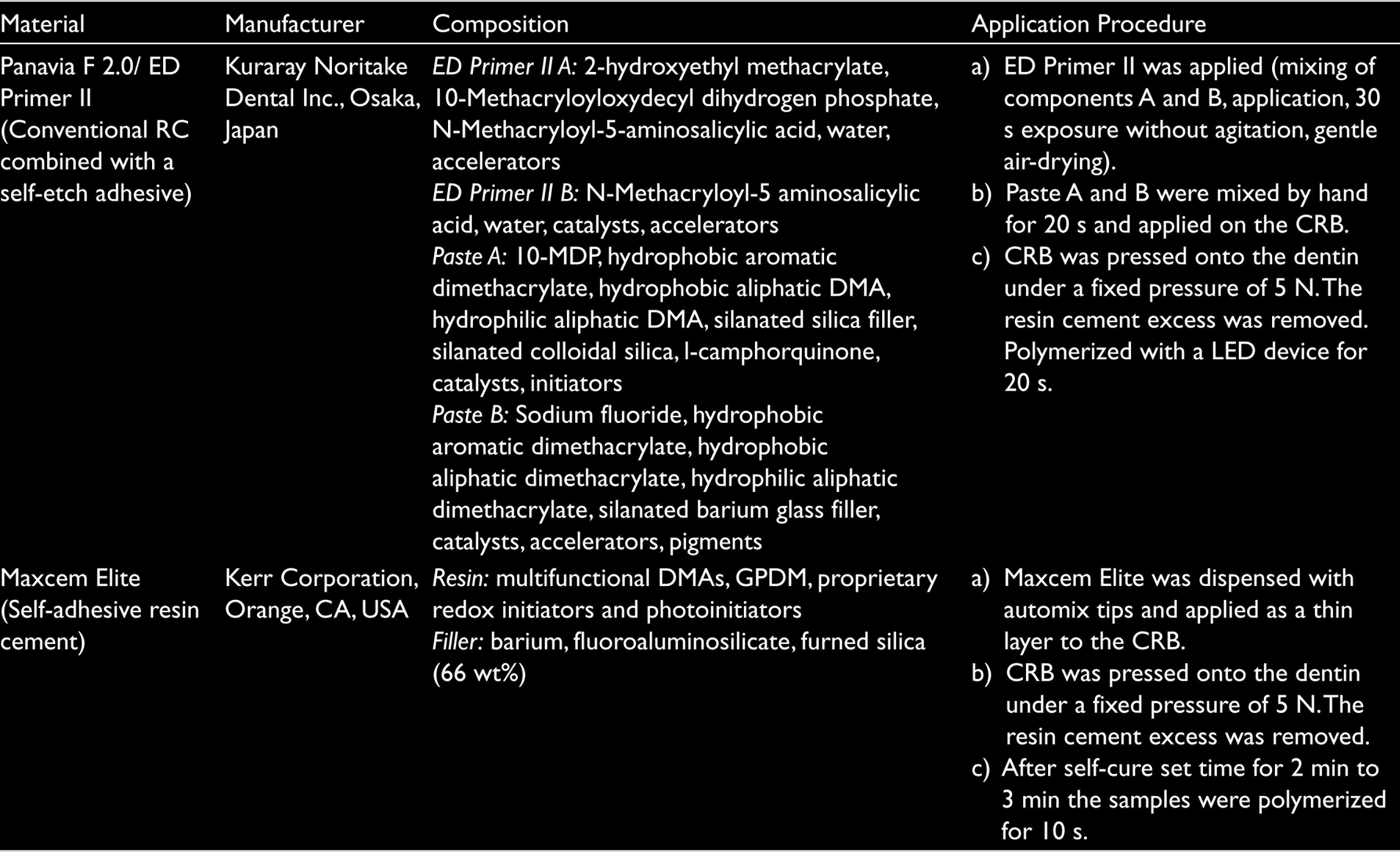
For self-adhesive RC groups, Maxcem Elite (Kerr, Orange, CA, USA) was dispensed with automix tips and applied as a thin layer to the CRB. For the conventional RC combined with self-etch adhesive groups, prior to the application of Panavia F 2.0 (Kuraray, Okayama, Japan), ED Primer II (Kuraray, Japan) was prepared, applied to dentin surface for 30 s without agitation, and gently air-dried. Then Paste A and B of Panavia F 2.0 were hand mixed and applied on the CRB. After the application of RC, the CRB was pressed onto the dentin surface under a 500 g load. The RC excess was removed, and RCs were polymerized according to the manufacturer’s instructions (Table 1). After the cementation, the specimens were immersed in distilled water for 24 h at 37°C. All luting agents were applied by the same researcher according to the manufacturer’s instructions.
Resin Cements, Composition, and Application Procedures
SBS Test and Failure Mode Analysis
The specimens were mounted in the universal testing device (AGS-X Shimadzu Corp., Kyoto, Japan). The distance between the adhesive surface and the crosshead was 0.1 mm, and the specimens were subjected to a shear force at a crosshead speed of 1 mm/min until the failure occurred. The SBS values were calculated in megapascals by dividing the maximum load force by the adhesive surface area. For the determination of the failure modes, both the fractured dentin and the CRB surfaces were examined using stereomicroscopy (Stemi C‐2000; Zeiss, Oberkochen, Germany) at 40× magnification and classified as follows: adhesive interfacial failure, cohesive failure in the resin composite, cohesive failure in the dentin, or mixed failure (partial adhesive failure with some cohesive failure in the RC).
Field Emission Scanning Electron Microscopy (FE-SEM) Observation of the Prepared Dentin Surface
Six teeth were used for the observation of the dentin surfaces that were prepared with abrasives (n = 2). Mid-coronal 2-mm-thick dentin slices were obtained from each tooth using a low-speed diamond saw (Microcut 125 Precision Cutter, Metkon). Afterward, 1-mm-deep transversal grooves were prepared with a high-speed cylindrical bur (Coarse, 852FG Meisinger) on the backside of the prepared dentin surface. The dentin slices were prepared with abrasives in the same way as described for the tooth preparation.
Following this, fixation was performed in 2.5% glutaraldehyde for 24 h, and dehydration was performed twice in increasing concentrations of ethanol (50%, 60%, 70%, 85%, 95%, and 100%) for 15 min each. The specimens were chemically dried with hexamethyldisilazane for 10 min and allowed to air-dry for 10 min, according to the protocol described by Perdigao et al. 16 Finally, the dentin slices were divided into two halves through transversal grooves with a hummer and blade to expose longitudinal sections of dentin discs. The specimens were sputter-coated with platinum–palladium, dentin surfaces, and longitudinal sections were observed using FE-SEM (10 kV, 0.005 Pa, Mira 3 XMU, Tescan).
FE-SEM Observation of the Resin Cement–Dentin Interface
The remaining parts of the six teeth from which the dentin slices were obtained were used for the observation of the RC–dentin interfaces. The teeth were randomly allocated to abrasive-RC subgroups (n = 1). The dentin surfaces were prepared and RCs were cemented in the same way as described for the tooth preparation and adhesive cementation. Afterward, the specimens were sectioned into two halves longitudinally with a diamond saw at a low speed (Microcut 125 Precision Cutter, Metkon, Bursa, Turkey). The teeth halves were fixed to epoxy resin molds in a way that exposed the RC–dentin interface. The specimens were prepared for FE-SEM observation according to the protocol described by Ting et al. 17 as follows: the specimens were ground with 600-, 800-, and 1000-grit silicon carbide papers (Buehler, Lake Bluff, IL, USA) and diamond polishing paste (Ultradent Products, South Jordan, USA). The specimen surfaces were treated with 1 M 5% hydrochloric acid for 30 s, followed by 5% NaOCl for 5 min, and were rinsed with distilled water. After drying, the specimens were sputter-coated and observed using FE-SEM (10 kV, 0.005 Pa, Mira 3 XMU, Tescan).
Statistical Analysis
Statistical analysis was performed using SPSS version 20.0 software (SPSS Inc., Chicago, IL, USA). The Kolmogorov–Smirnov test revealed that the SBS data were not normally distributed. The differences between the RCs were examined using the Mann–Whitney U test with Bonferroni correction. The effect of the dentin surface preparation with different abrasives on the bond strength was analyzed with the Kruskal–Wallis analysis of variance test. The significance level was set at 0.05 for all statistical tests.
Results
SBS Test
No pretest failures occurred in this study. The median and quartiles of SBS values of the study groups are presented in Table 2. The results of the study indicated significant effects of the type of RC and surface preparation method on the SBS (P ˂ .05). The highest SBS was observed in Panavia F 2.0/ED Primer II applied on dentin surface prepared with coarse diamond, and the lowest SBS was observed in Maxcem Elite applied on the dentin surface prepared with the polishing discs.
Shear Bond Strength Values (SBS) ± Standard Deviations (SD) in MPa to Dentin

Note. *p value a, p value b, Mann–Whitney U test results (p < .05);
***The superscript lowercases indicate significant differences in column.**p value b, Kruskal–Wallis analysis of variance test results (p < .05).
When comparing SBS values dependent on the type of RC, Panavia F 2.0/ED Primer II had higher values than Maxcem Elite, irrespective of the preparation method. For the dentin surface prepared with coarse diamond, Panavia F 2.0/ED Primer II had higher bond strength than Maxcem Elite (P ˂ .05). However, the differences were not significant for the extra-fine diamond and the polishing disc groups (P ˃ .05).
Panavia F 2.0/ED Primer II exhibited significantly higher SBS values for the coarse and the extra-fine diamond than for the polishing discs (P ˂ .05). The difference between the coarse and the extra-fine diamond was not significant (P ˃ .05). Regarding Maxcem Elite, no significant difference was observed for the preparation methods (P ˃ .05).
Fracture Mode Analysis
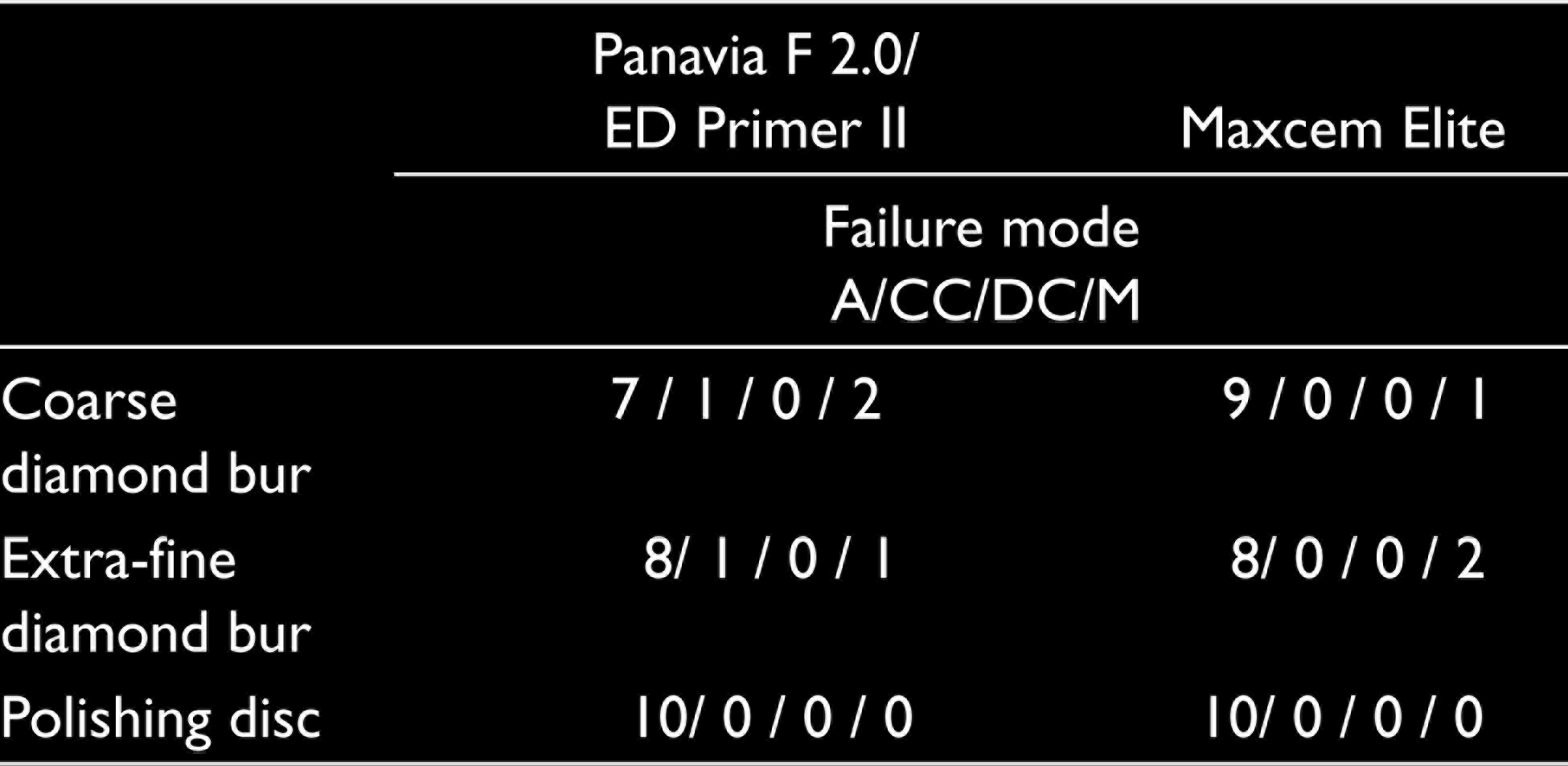
The distribution of the failure modes of the study groups is presented in Table 3. In general, adhesive failure is the common failure type for each group (52/60). No cohesive failures in the dentin were observed. In addition, no cohesive failures were observed in the polishing-disc-prepared groups.
Failure Mode Distribution of the Study Groups
FE-SEM Analysis of Prepared Dentin Surface and Interfacial Structure
Figure 1 presents FE-SEM microphotographs of the dentin surfaces prepared with different abrasives. FE-SEM images revealed that the smear layer covers the dentin surfaces and the smear plugs occlude the orifices of the dentin tubules. The coarse diamond bur produced the roughest surface and the extra-fine diamond produced a rougher surface than the polishing discs.
Representative Fe-SEM Images of Prepared Dentin Surfaces and Longitudinal Sections. A Longitudinal Section of the Dentin Surface Prepared by (a ) Coarse Diamond Bur, (b ) Fine Diamond Bur (c ) Polishing Discs at Magnification of 10,000× (Inserts: 3000×). Dentin Surface Prepared by (d ) Coarse Diamond Bur, (e ) Fine Diamond Bur, (f ) Polishing Discs at Magnification of 10,000× (Inserts: 2000×).
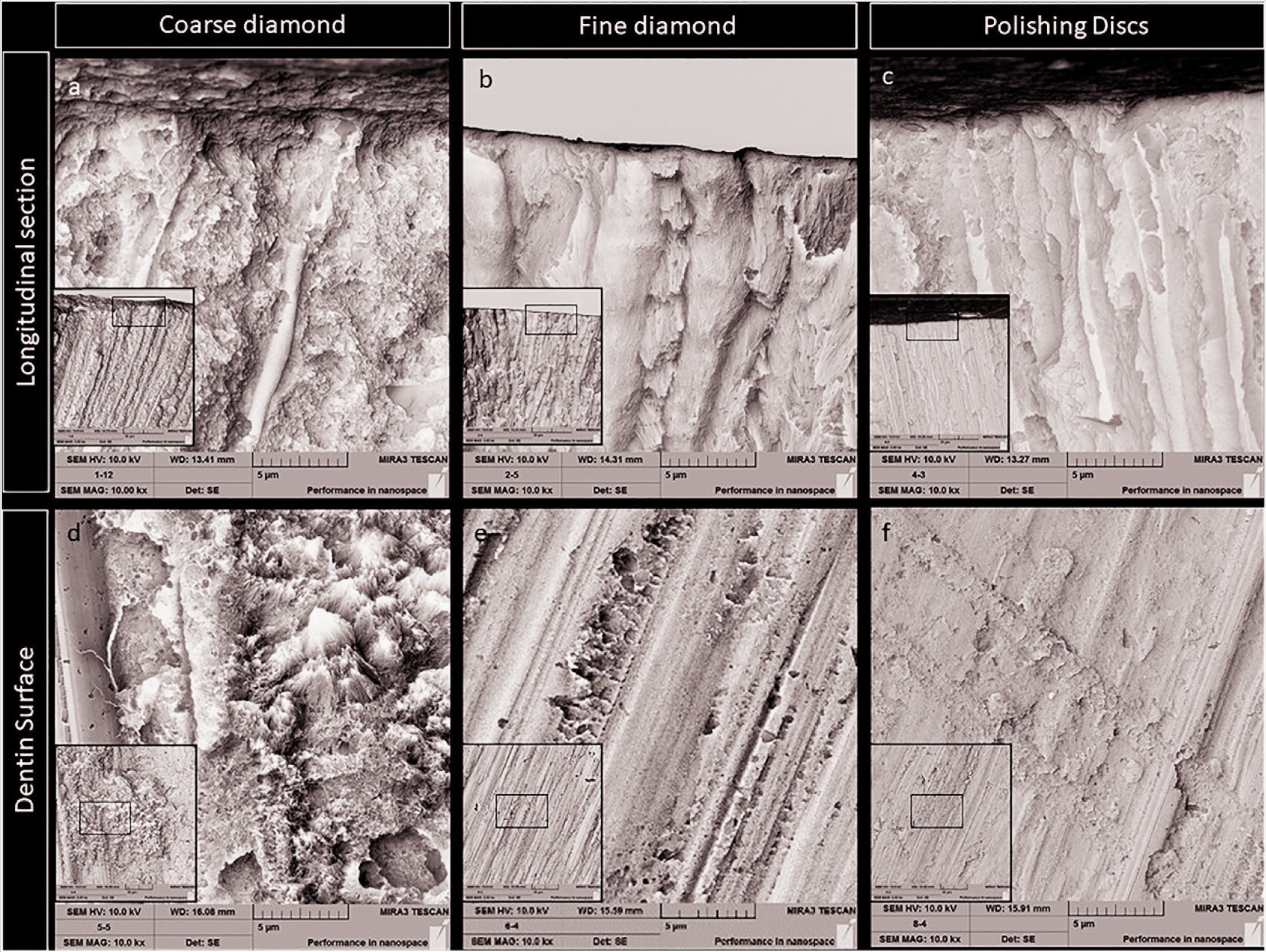
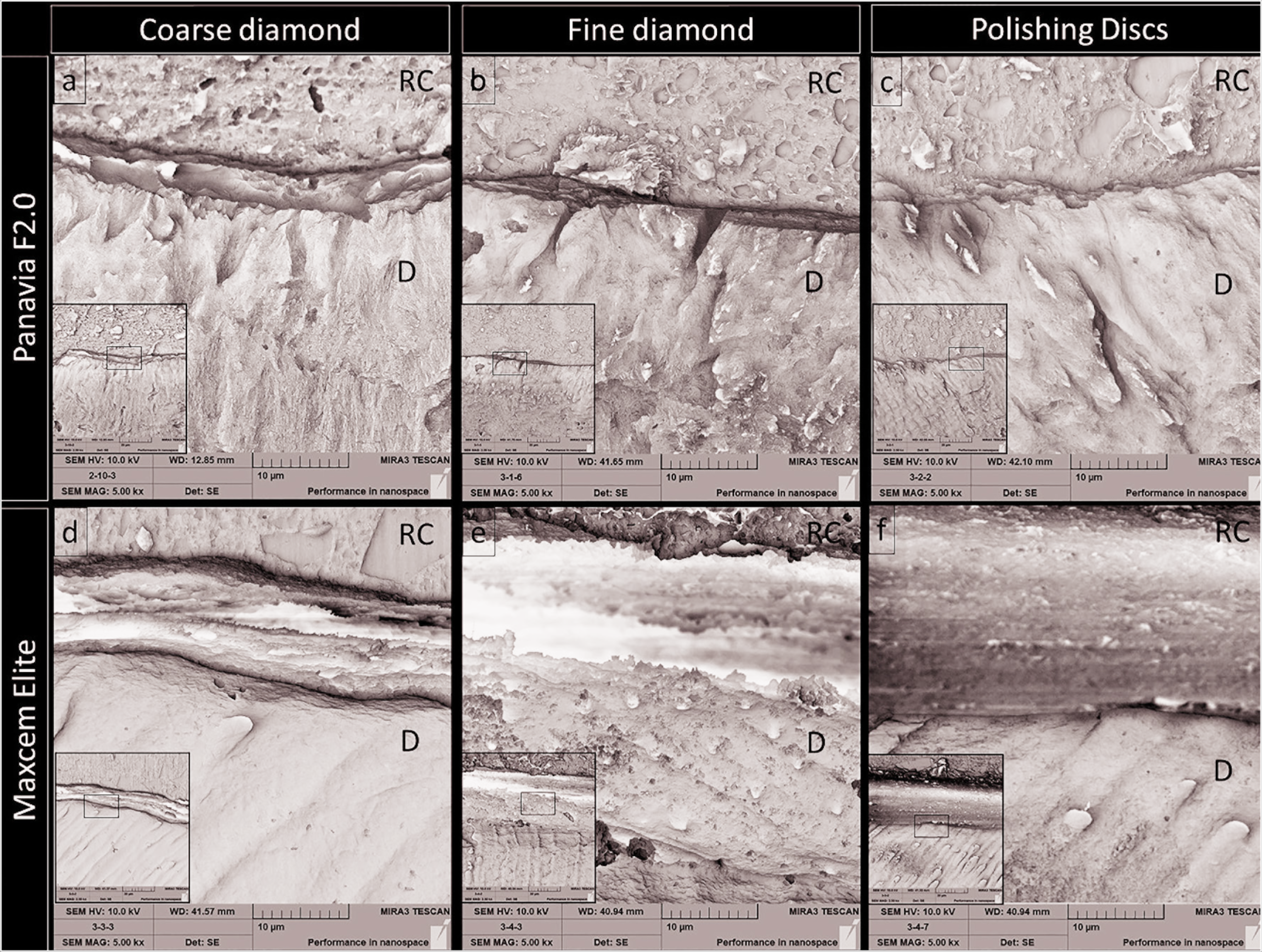
Figure 2 presents FE-SEM microphotographs of the RC–dentin interface. There was some evidence of resin tags and hybrid layer formation for Panavia F 2.0/ED Primer II. However, there was neither a hybrid layer nor resin tags were observed in the Maxcem Elite groups. Additionally, in some areas, separations were detected along with the Maxcem Elite and the dentin surfaces. Interestingly, no residual smear layer was observed, and the orifices of the dentin tubules were visible on the separated areas.
Representative Fe-SEM Images of Resin–Dentin Interfaces of the Tested Groups. (a ) Panavia F 2.0/ED Primer II Bonded to Coarse-Diamond-Prepared Dentin, (b ) Panavia F 2.0/ED Primer II Bonded to Fine-Diamond-Prepared Dentin, (c ) Panavia F 2.0/ED Primer II Bonded to Polishing-Disc-Prepared Dentin, (d ) Maxcem Elite Bonded to Coarse-Diamond-Prepared Dentin, (e ) Maxcem Elite Bonded to Fine-Diamond-Prepared Dentin, (f ) Maxcem Elite Bonded to Disc-Prepared Dentin.
Discussion
The results of this study indicate higher SBS values for the conventional RC combined with a self-etch adhesive than for the self-adhesive RC independent of the type of abrasive used for the dentin surface preparation. In addition, the conventional RC combined with a self-etch adhesive demonstrated higher SBS values when bonded to the dentin that had been prepared, with the coarse or the extra-fine diamond, rather than the polishing discs. However, no significant difference was observed for the self-adhesive RC bonded to the dentin that had been prepared with different abrasives. Therefore, the null hypothesis has to be partially rejected.
The self-adhesive RCs were introduced in order to reduce technique sensitivity by decreasing the number of application steps and shortening chair time. However, the clinical success of adhesively cemented restorations is dependent on the quality of the adhesion and dentin hybridization. 18 The self-adhesive RC tested in this study demonstrated lower SBS values to the coarse-diamond-prepared dentin. In line with the results of this study, previous studies reported a lower bond strength of self-adhesive RCs to dentin.7, 14, 19 In addition, Scholz et al. 20 reported inferior clinical performance after 39 months for self-adhesive resin cement compared to conventional resin cement with universal adhesive regarding retention, marginal adaptation, color stability, and marginal staining.
The adhesion mechanism of self-adhesive RCs depends on the dissolving smear with the initial acidity of phosphoric ester monomers and infiltrating into the dentin and enamel.7, 21 However, hybrid layer formation was not observed in FE-SEM micrographs (Figure 2) of the self-adhesive RC groups in this study, and this corroborates the findings of Stona et al. 22 Moreover, some separation areas were detected along with the self-adhesive RC and the dentin surfaces. Although the desiccation and high vacuum conditions could be blamed for this observation, 13 separation areas were not detected in the conventional RC combined with self-etch adhesive groups. Interestingly, no residual smear layer was observed and the openings of the dentin tubules were visible on these areas. Self-adhesive RCs ideally have a low pH value after mixing to etch enamel and dentin sufficiently, and pH-neutralization is required after the adhesion is achieved. 3 Roedel et al. reported that after mixing Maxcem Elite showed an initial decrease in the pH value (pHmin 3.98), and the pH value increased slowly (after 24 h pH 4.20). 23 Maintaining the acidic pH for longer than 24 h could be successful in dissolving the smear layer but not in the infiltration of the resin monomer into the exposed tubules. Infiltration of the self-adhesive RC could be hindered by the low viscosity of the cement. 2 These findings can also explain the intensity of the adhesive type failures in self-adhesive RC groups.
The chemical composition, pH, and viscosity of the RCs may affect the adhesion and bonding ability of the material. 22 The conventional RC combined with a self-etch adhesive tested in this study contains 10-methacryloxydecyl dihydrogen phosphate (MDP) as a functional monomer. Methacryloxydecyl dihydrogen phosphate can establish chemical bonding with hydroxyapatite and can form nano-layering at the adhesive interface.24, 25 In addition, the conventional RC combined with a self-etch adhesive system has a two-step application procedure: The ED Primer II is applied first to dissolve the smear layer and partially demineralize the dentin. In this regard, Scholz et al. 13 observed more micromorphological interactions at the adhesive interface of Panavia F 2.0/ED Primer II compared to the self-adhesive RCs using low-vacuum SEM. The separate application of the primer and the adhesive cement can create a more stable hybrid layer with enhanced mechanical properties. 26
Appropriate preparation of the dentin surface for indirect restoration is of great importance regarding internal adaptation and adhesive cementation.5, 27, 28 The smoothness and regularity of the prepared dentin surface can influence the precision of the dental impression. 11 In addition, the thickness of the smear layer decreases with the fine grit abrasives.15, 29 Using a finishing bur for the completion of the preparation 30 and the application of additional polishing procedures to preparations 5 have been previously suggested to enhance the wettability and adhesion. However, the use of the polishing disc has a limited extent in posterior complex partial crown preparations. In addition, like the results of the study by Koodaryan et al., 31 the conventional RC combined with a self-etch adhesive showed the lowest SBS in the present study when applied on the dentin surface prepared with polishing discs. Ayad et al. 32 stated that the increasing roughness can improve the bond strength because of the increasing surface area. The decrease in the dentin surface area with the increasing surface smoothness could be responsible for the lower SBS in the present study, as stated previously. 31
The adhesion mechanism of the self-adhesive RCs is mainly chemical instead of micromechanical interlocking. 33 The hybrid layer is not formed in this group because of the insufficient demineralization of the smear layer and the superficial interaction with the dentin. For these reasons, regarding the self-adhesive RC, the preparation methods or the smear layer thickness generated no significant difference on the bond strength. This result corroborates with a previous study conducted by Cerqueira et al. 11
This study investigated the early failures after short-term (24 h) storage in distilled water. Under clinical conditions, the adhesive interfaces are prone to degradation and face various types of stresses including thermal, chemical, and physical stresses. Therefore, the effect of these stresses and the intraoral conditions on the bond strength should be investigated in further studies.
Conclusion
Within the limitations of this study, it can be concluded that:
The use of the polishing discs did not increase the SBS of tested RCs to dentin. Conversely, the use of the polishing discs resulted in lower SBS compared to coarse diamond bur for the conventional RC combined with a self-etch adhesive. The use of coarse or extra-fine diamond burs exhibited similar SBS for the conventional RC combined with a self-etch adhesive. The type of abrasive used for the dentin surface preparation did not have a significant impact on the SBS of the conventional RC combined with a self-etch adhesive. The conventional resin cement combined with a self-etch adhesive exhibited a higher SBS compared to the self-adhesive resin cement when bonded to the dentin prepared by coarse-diamond bur.
Footnotes
Acknowledgements
The authors would like to thank Yunus Emre Kuyucu for his support in statistical analysis.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Author Contributions
Conception: KY-HH; Design: KY-HH; Supervision: KY-HH; Data collection and/or processing: KY-HH; Analysis and/or interpretation: HH; Literature review: KY-HH; Writer: HH-KY; Critical review: HH-KY.
Ethical Statement
This study was approved by the Tokat Gaziosmanpasa University Clinical Research Ethics Committee with registration number 21-KAEK-154.
Data Availability Statement
The data of the study are available for access.