
Abstract
Objective:
To evaluate the efficacy and safety of preoperative embolization and vertebroplasty in the treatment of aggressive hemangioma.
Methods:
A retrospective clinical review of patients diagnosed with aggressive vertebral hemangiomas was conducted. All the patients were assigned to three groups according to the treatment strategies: patients in Group A underwent embolization and decompression with internal fixation, patients in Group B underwent vertebroplasty and decompression with internal fixation, patients in Group C received all three treatments. Clinical indexes were compared within three groups.
Results:
There were 16 patients received embolization and decompression (Group A), 19 patients underwent decompression with vertebroplasty (Group B) and 16 patients in Group C. The operative duration of patients in group A (198.33 ± 38.43 min) were less than another two groups (p = 0.001). The intraoperative blood loss of patients in group C was 713.33 ± 165.13 mL, which was significantly less than group A and group B (p = 0.045). Patients in group C exhibited the lowest volume of drainage on POD 1 (178.33 ± 66.76 mL), which showed significant difference compared with group A (368.33 ± 191.15 mL, p = 0.01). There was no significant difference of preoperative and postoperative VAS and JOA score among three groups, as well as drainage on POD 2, total volume and hospital duration.
Conclusion:
Both embolization and vertebroplasty are efficient and safe measures to reduce blood loss in the surgical treatment of aggressive vertebral hemangiomas, combination of all three methods is also competent.
Introduction
Vertebral hemangioma is a benign angiogenic tumor that accounts for 2–3% of all spinal tumors. 1 In the majority of patients, it is asymptomatic and does not require any treatment other than follow-up. 2 However, in 0.9–1.2% of patients, these lesions can cause clinical symptoms of nerve compression due to bone dilation, cortical erosion, fracture, or hematoma, which is known as aggressive vertebral hemangioma. 3 In contrast to the asymptomatic ones, aggressive vertebral hemangiomas may involve the entire vertebra and extend to the rear of the vertebra, presenting as an irregular honeycomb with a zone of radiolucency. 4 The symptoms depend on the tumor’s location and the degree of compression of the spinal cord or nerve root. 5 Aggressive vertebral hemangioma is more common in adults, but has also been reported in children. 6,7
Symptomatic aggressive vertebral hemangioma often requires clinical treatment; however, there is great controversy over the treatment plan. The treatment of this disease mainly includes surgical resection, vertebroplasty, endovascular embolization, and radiotherapy. 8 –10 Due to the abundant blood supply of an aggressive vertebral hemangioma and more bleeding during surgery, traditional total vertebral resection is no longer regarded as the mainstream approach. 11 Therefore, an increasing number of scholars recommend perioperative measures to control bleeding, such as radiotherapy, embolization, and vertebroplasty. 8,12 –14 Through these methods, surgeons can reduce vascularity of the lesions and improve safety of surgery effectively.
In the treatment of aggressive vertebral hemangiomas, we adopted various strategies of preoperative embolization and selective decompression after intraoperative vertebroplasty, which not only effectively reduced intraoperative bleeding but also achieved good clinical effects. In this study, we retrospectively evaluated the efficacy and safety of different methods in the treatment of aggressive vertebral hemangioma.
Materials and methods
We retrospectively analyzed all neurosurgical interventions on the spine performed at the spine surgery department of Qingdao university hospital from 2012 to 2019, and identified all patients with stage 3 vertebral hemangioma. All relevant clinical data of these patients, including imaging, laboratory findings, surgical options, and histopathology results, were collected. The data collection was approved by our ethics committee and informed consent was signed by all patients.
Based on the treatment strategies, the patients were assigned to one of three groups: Group A with patients who underwent embolization before decompression and pedicle screws fixation; Group B, who underwent decompression with pedicle screws fixation and vertebroplasty; and Group C, who received all three treatments.
Surgical technique
In this study, 25 patients received surgery because of rapid neurological deterioration, 18 patients with vertebral fracture and eight patients was because of severe kyphotic deformity with intractable pain.
All procedures of endovascular embolization were performed under local anesthesia around the right femoral artery with lidocaine. The operation was performed under the guidance of fluoroscopy with patient in a prone position. After successful puncture of the right femoral artery with Seldinger technology, 5F artery sheath was inserted and a catheter was sent to the abdominal aorta to perform angiography, which showed abnormal staining of the diseased vertebral body. Under fluoroscopy, the microcatheter was channeled into the supplying artery and injected with spring coil and polyvinyl alcohol (PVA) particles for embolization. Local compression was required after the catheter and arterial sheath were dropped out, and the compression could be relieved 24 h later.
In the posterior decompression surgery, the patients were in the prone position. We first performed pedicle screw implantation, and then, under the guidance of fluoroscopy, we slowly injected polymethyl methacrylate (PMMA) with appropriate viscosity through the bilateral pedicle. The tip of the injection sleeve was kept as close as possible to the ventral side of the vertebral body, to increase the proportion of filling of the vertebral body and achieve the vasoconstriction in the affected vertebral body. After filling the diseased vertebral body with bone cement, the blood supply was reduced and the tumor volume decreased. 7,12 At this point, the posterior lamina was resected, as well as a part of the medial wall of the pedicle if necessary, revealing the normal dural sac in the decompressed vertebral canal. Bipolar electrocoagulation was used to fully stop bleeding and clean up the residual tumor tissue. After full decompression, the posterolateral fusion was performed with allograft.
Intraoperatively, the lesion was taken for histopathologic examination; histopathology assessment revealed features of aggressive vertebral hemangioma: complex vascular pathways, extensive reactive changes, osteoblastic activity, rare mitosis, and extensive CD31 immunoreactivity. At 3, 6, and 12 months after the surgery, ortholateral radiograph of the spine was performed to detect possible complications, such as kyphosis, local instability, or failure of internal fixation, whereas the tumor recurrence was monitored by magnetic resonance imaging (MRI) examination. If recurrence or residual lesions had been suspected during reexamination, adjuvant radiotherapy was performed.
We estimated intraoperative blood loss based on the weight of the soaked surgical sponges and volume in suction canisters subtracting irrigation fluid added to the surgical field. At the end of the operation, we placed a deep drainage below the fascia. The amount of drainage on postoperative day 1, postoperative day 2, and the total drainage volume were recorded.
The drainage was routinely removed when the drain output was less than 100 mL per 24 h. Recorded clinical data include age, operative duration, surgical level, intraoperative blood loss, postoperative drainage, related complications, length of hospital stay, and recurrence rate.
Four parameters were compared among the three groups: (1) surgical duration and blood loss; (2) volume of drainage on the first postoperative day (POD 1), volume of drainage on the second postoperative day (POD 2), and total volume of drainage; (3) hospitalization duration; and (4) complications and recurrence rate.
Statistical analysis
All of the data analyses were performed with the SPSS 23.0 software package. Pearson’s chi-square test was used to analyze categorical variables. Anderson–Darling test was used to identify whether the data were normally distributed. Measurable variables were presented as means and standard deviations if the data were normally distributed; otherwise, they were presented as median and range. The differences in measurement data among the groups were analyzed by homogeneity test of variances. One-way ANOVA was used when variances were homogenous, whereas in case of uneven variances, Welch test and Brown-Forsythe test were performed. The level of statistical significance was set at p < 0.05.
Results
From 2011 to 2019, 51 patients (29 women and 22 men) diagnosed with aggressive vertebral hemangioma received treatment in our hospital. The average age at the time of surgery was 60.9 years (age range, 39–75 years), and the average follow-up was 5.3 ± 2.1 years. All patients suffered from neurologic deficits or severe back pain attributable to vertebral fracture or kyphotic deformity; eight patients exhibited syndrome of cauda equina, and seven patients presented with worsening spastic paraparesis. Thirty vertebral hemangiomas were located in the thoracic and 21 in the lumbar spine. For three patients with multiple lesions, we only performed surgery at the level of compression. In general, pedicle screws were inserted to vertebral pedicles from one level above to one level below the diseased vertebra; however, in three patients (two from the group B, and one from the group C) stabilization was extended to two levels cranially and caudally because of a severe vertebral fracture.
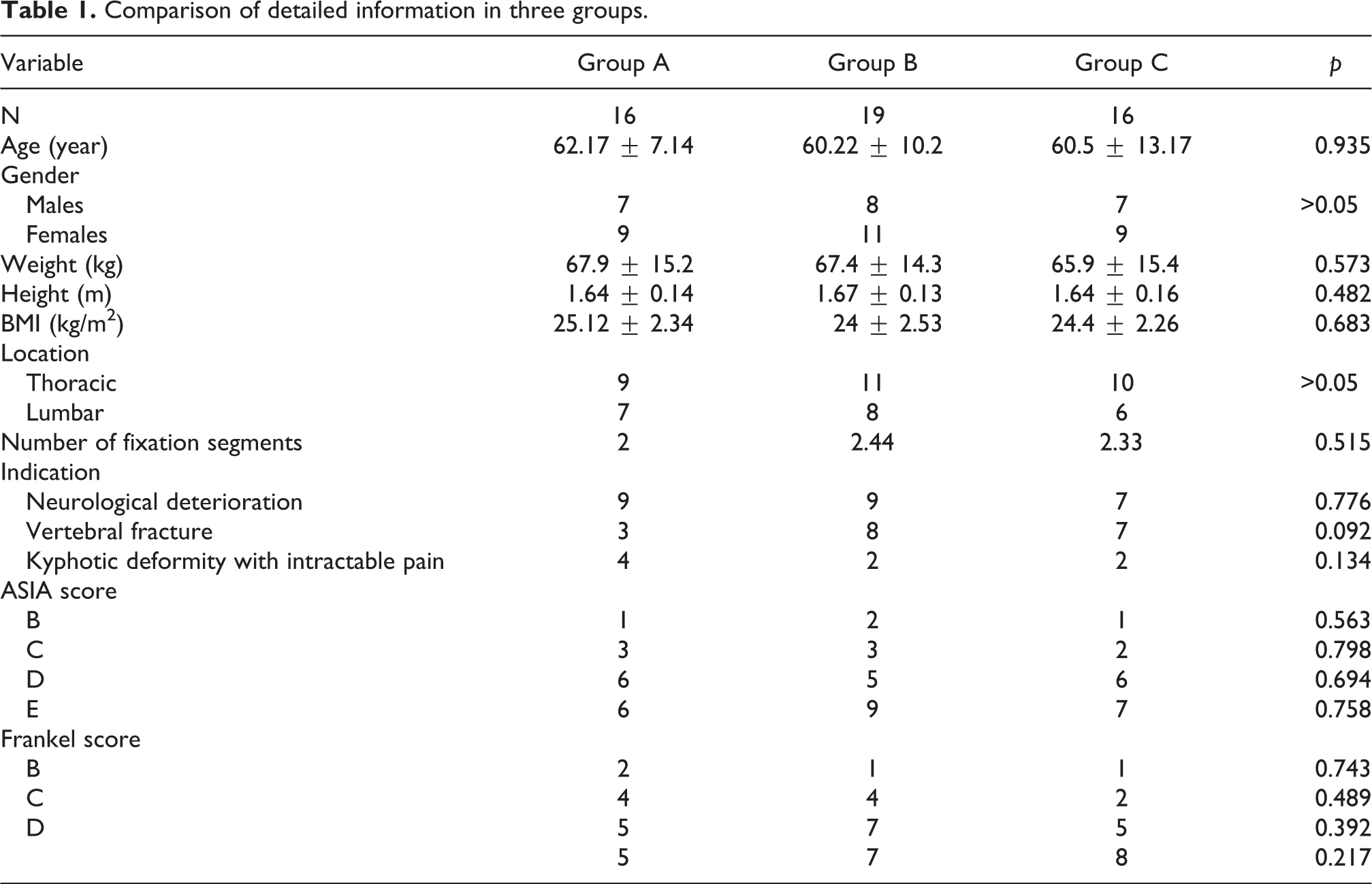
There were 16 patients who had received embolization and decompression (group A), 19 patients who had undergone decompression with vertebroplasty (group B), and 16 patients in group C. The basic information of patients in these three groups is listed in Table 1. No significant differences in sex, age, body mass index (BMI), tumor location, number of fixation segments, ASIA score and Frankel score were detected between the groups (p > 0.05).
Comparison of detailed information in three groups.
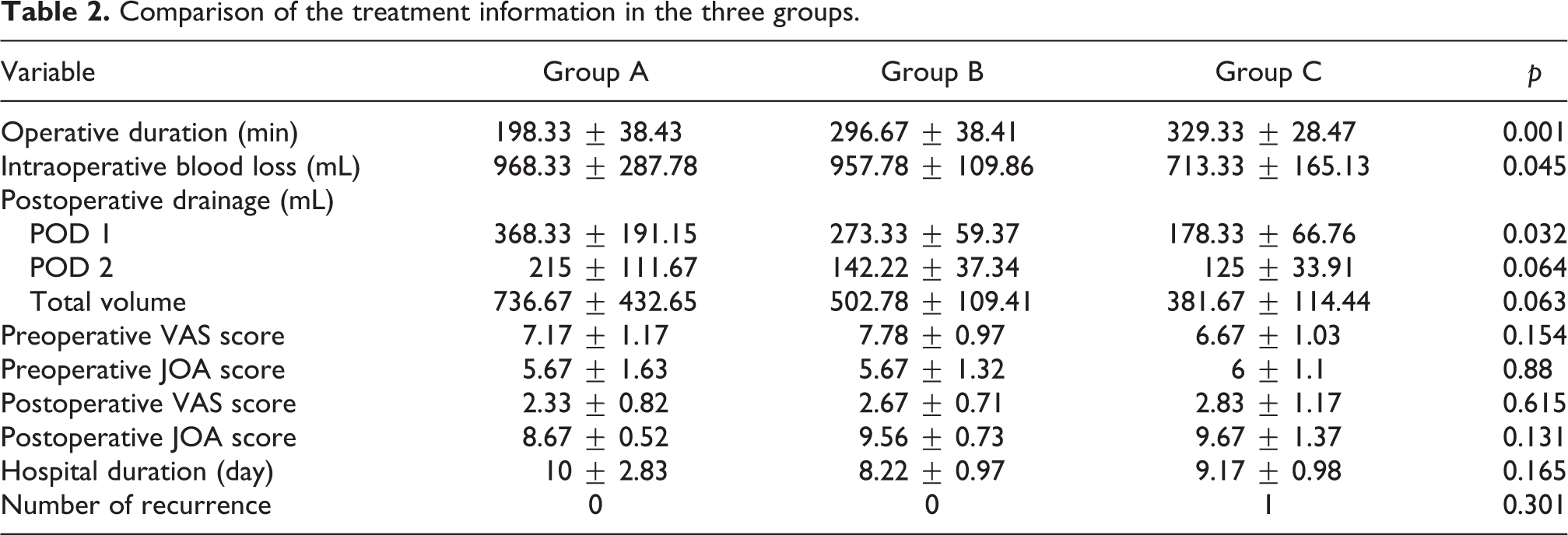
The operative duration of patients in group A (198.33 ± 38.43 min) was significantly lower (p = 0.001) than in other two groups (296.67 ± 38.41 min in group B, and 329.33 ± 28.47 min in group C). Intraoperative blood loss of patients in group C was 713.33 ± 165.13 mL, which was significantly lower than in group A (968.33 ± 287.78 mL) and group B (957.78 ± 109.86 mL) (p = 0.045). In addition, patients in group C exhibited the lowest volume of drainage on POD 1 (178.33 ± 66.76 mL), which showed significant difference compared with group A (368.33 ± 191.15 mL, p = 0.01) and no significant difference compared with group B (273.33 ± 59.37 mL, p = 0.131).
All of the patients experienced significant pain and neurological deficits, with the preoperative visual analog scale (VAS) score of 7.29 ± 1.1 and preoperative JOA score of 5.76 ± 1.3. After surgery, the VAS score decreased significantly to 2.62 ± 0.87 (p = 0.001), and JOA score improved to 9.33 ± 0.97 3 months later (p = 0.001). However, there were no significant differences in preoperative and postoperative VAS and JOA scores, drainage on POD 2, total volume, and hospital duration among three groups (Table 2).
Comparison of the treatment information in the three groups.
Typical case 1
A 71-year-old male suffered from severe back pain and numbness in both lower limbs for 1 month. On examination, the patient presented with paresthesia and reduced muscle strength in his extremities, whereas all of the reflexes in the lower limbs were exaggerated with extensor plantar response. The CT scan and MRI revealed a vertebral compression fracture of the eighth thoracic vertebra (T8), and an aggressive vertebral hemangioma centered within the vertebral body of the fourth thoracic vertebra (T4) with bony and soft tissue extension into the spinal canal and neural foramen. The patient underwent preoperative embolization, vertebroplasty, and T4-level decompressive laminectomy, followed by decompression of the epidural component, and the internal fixation from T2 to T6. One week after the operation, his VAS score improved from 7 to 4, and JOA score improved from 5 to 8 (Figure 1).

Images obtained in Case 1, which involved a 71-year-old man who presented with pain and paresthesia in both lower limbs. Preoperative images (panels A–D) show an expansive lytic lesion at the T4 vertebral body with posterior epidural component compression; sagittal MR (panels A and B) images show the vertebral lesion as hyperintense on fat saturation phase. Lateral and antero-posterior fluoroscopic images (panels E and F) after the operation depicted that the bone cement filled up the T4 vertebral body with posterior spinal stabilization from T2–T6 levels. The sagittal T1W1 (panel G) showed the spinal cord compression had been removed.
Typical case 2
Only one recurrence case in our study was recorded, which was a 75-year-old woman with a history of numbness from the region of the umbilicus down to the lower limbs. Preoperative thoracic MRI showed that the hemangioma located at the centre of T9 vertebral body. After preoperative embolization, she received vertebroplasty, decompression, and instrumentation from T8 to T10 in 2016. The operation was successful, and her clinical symptoms were relieved. Three years later, she suffered from numbness of the lowers limbs again, and subsequent imaging studies demonstrated hemangioma recurrence with paraspinal and pedicle extension (Figure 2).
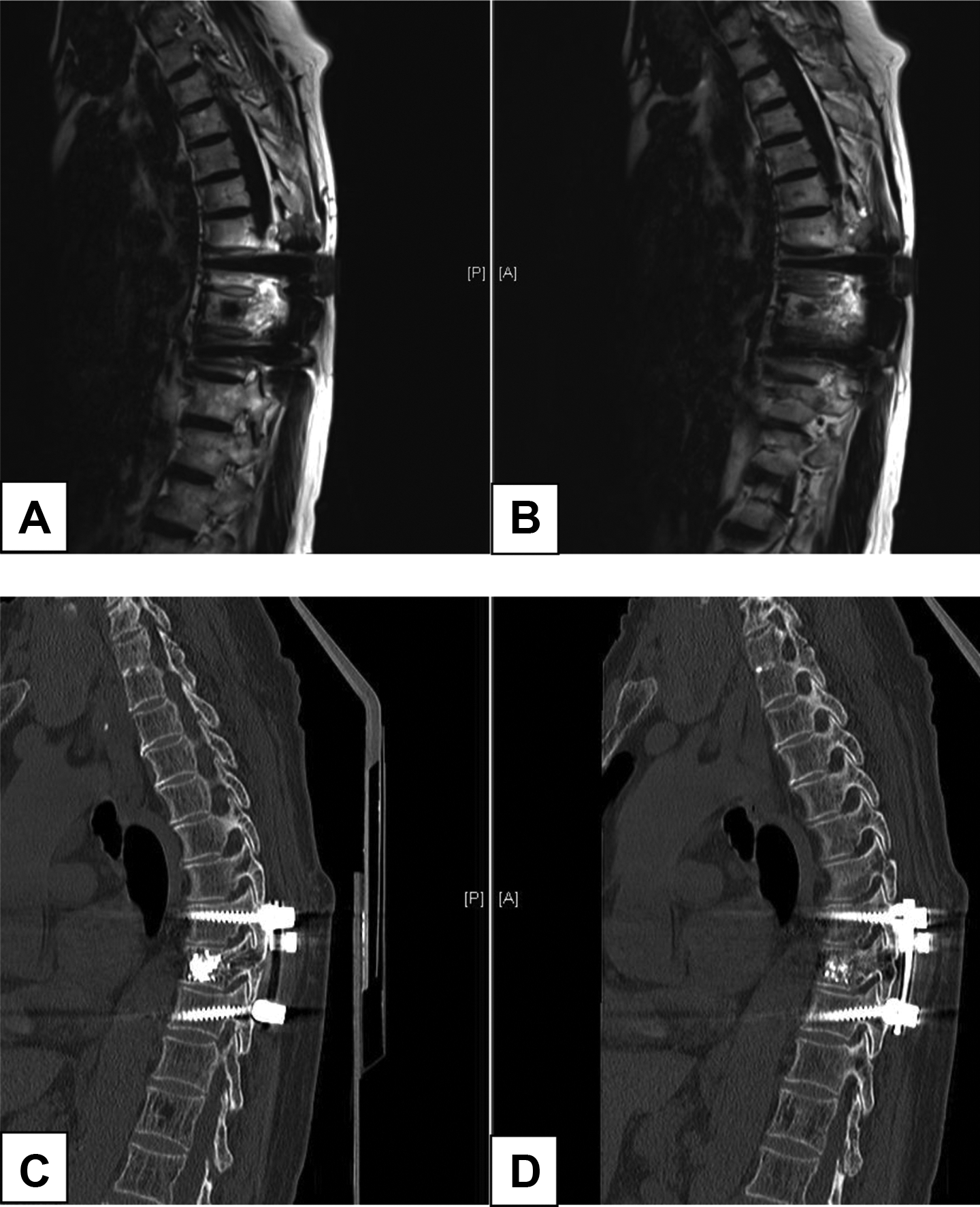
Images obtained in Case 2, which involved a 75-year-old woman who presented with paresthesia in both lower limbs. T9 hemangioma recurred after the operation that had included preoperative embolization, vertebroplasty, decompression, and internal fixation from T8 to T10 3 years ago. Sagittal MRI (panels A and B) and CT (panels C and D) images demonstrate a recurrent, aggressive, vertebral hemangioma involving the entire vertebral body and extending through both pedicles into the posterior elements.
Discussion
Clinically, the majority of vertebral hemangiomas are asymptomatic and discovered by chance, and usually no treatment is required. However, aggressive vertebral hemangioma could destroy the vertebral structure, and cause pain, local malformations, and even spinal cord compression. 15 In 1927, Makrykostas reported a case of spinal stenosis due to aggressive vertebral hemangioma that led to neurological symptoms. 16 Therefore, active treatment is usually required for patients with significant spinal instability and spinal nerve compression. At present, there are many treatment methods for aggressive vertebral hemangioma, including total vertebral resection and decompression surgery, partial vertebral resection, preoperative radiotherapy, vascular embolization, and intraoperative vertebroplasty with bone cement. 17 Most of those methods achieve certain effects, but selection of the optimal treatment strategy is still controversial. For aggressive vertebral hemangiomas, the aim of surgery is to relieve compression and restore spinal stability to improve symptoms while minimizing recurrence. Although total vertebral resection can effectively reduce tumor recurrence, it is limited by its complications, such as massive intraoperative blood loss, high risk of nerve injury, and other complications. Chen et al. 8 reported a case series of patients with compressive vertebral hemangioma, and showed that blood loss for the en bloc procedure was around 1200 mL and the surgical duration was 2.3 h. He stated that for aggressive vertebral hemangioma with incomplete paralysis, total en bloc spondylectomy should be considered. However, his article included only one patient who had undergone en bloc spondylectomy. Ogawa et al. 18 described a patient ith aggressive vertebral hemangioma with spinal cord compression; the patient received total en bloc spondylectomy, preceded by arterial embolization, and lost 2232 g of blood after 413 min of surgery. In a multicenter study, Goldstein et al. 3 explored the results of surgical treatment for spinal hemangiomas. By analyzing 68 patients who had undergone surgical treatment, he concluded that it is unnecessary to perform total en bloc resection to achieve a wide surgical range, as total resection would lead to more intraoperative bleeding and higher surgical morbidity. Ji et al. 4 reported 23 patients with vertebral hemangiomas treated with total en bloc spondylectomy. The mean operation time of patients with preoperative embolization was 426.6 ± 104.3 min and the mean blood loss was 1883.3 ± 932.1 mL. Neurological deficits improved in all cases, without recurrences. As surgery alone can lead to significant blood loss and mortality, it can be combined with various preoperative or intraoperative measures. With the improvement of surgical techniques, it would be possible to relieve neurological function and restore spinal stabilization.
Aggressive vertebral hemangioma is rich in blood supply and often accompanied by massive bleeding during surgical resection. Endovascular embolization is one of the effective non-surgical methods for treatment of aggressive vertebral hemangioma. Sokol Trungu 19 reported five vertebral hemangioma patients with neurological symptoms. At first, embolization was attempted for them, and if the symptoms persisted, decompressive laminectomy would be performed. Two of them received embolization as the only treatment, and after 18 and 36 months of follow-up, they achieved remission of symptoms without recurrence. Hurley et al. 13 reported on Onyx embolization of two aggressive vertebral hemangiomas, wherein the postoperative CT confirmed the desired results of Onyx distribution through the body with good visibility, good control, and shorter injection times. However, there were also some negative experiences, such as lower effective rate and higher frequency of relapse. In Smith et al’s 20 research, two patients who received embolization as a sole treatment did not improve clinically. Kiroglu et al. 21 reported a case of a pregnant woman suffering from T4 vertebral hemangioma and used endovascular embolization as sole treatment. Her symptoms and neurologic deficits improved quickly after the embolization, but restarted 2 years later, so that she had to receive intraoperative vertebroplasty and internal fixation at last. Therefore, endovascular embolism is not only an independent treatment but also an efficacious adjunctive procedure to reduce bleeding and improve surgical safety.
Just as endovascular embolization, vertebroplasty with bone cement is an independent treatment of aggressive vertebral hemangioma, as well as an aid to surgical resection and decompression. It can further embolize small vessels and destroy the tumor tissue while enhancing the strength of the vertebral body. At the same time, vertebroplasty is also an effective method to reduce the risk of recurrence and relieve local pain. 22 Spinal cord compression caused by leakage or expansion of bone cement is the most common complication of this procedure. 23 Moreover, vertebroplasty makes the spine segment stiffer and could cause adjacent segment fracture. This risk was more frequent with older generations of bone cement. Issa et al. 24 reported two cases of aggressive vertebral hemangiomas treated with vertebroplasty. Under biplanar fluoroscopic guidance, acrylic cement was injected in the vertebral body without leakage, and the clinical efficacy and safety were satisfactory at 2-year follow-up. Wang et al. 12 retrospectively reviewed 39 patients diagnosed with aggressive (Enneking stage 3, S3) vertebral hemangiomas, including 17 patients who had undergone decompression alone and another 22 patients who had received decompression along with intraoperative vertebroplasty. The average estimated blood loss of decompression group was higher than of decompression plus vertebroplasty group (1764.7 mL vs. 1068.2 mL), and vertebroplasty helped in minimizing recurrence after decompression.
Here, we presented different surgical managements of aggressive vertebral hemangioma, which involved preoperative embolization, vertebroplasty, decompression, and internal fixation. We demonstrated that the combination of embolization and vertebroplasty can be carried out with less blood loss and improvement in pain and neurological function. Only one patient recurred after the treatment. Considering high local infiltration and rapid growth characteristics of aggressive vertebral hemangioma, this recurrence rate is acceptable, which proves the effectiveness and durability of the treatment strategy in this study. However, it was surprising that the only recurrence case was in group C, which showed that even the comprehensive treatment including canal decompression, endovascular embolization, vertebroplasty, and internal fixation does not mean absolute cure.
Conclusion
In our study, we explored the clinical effect of preoperative embolization, vertebroplasty, decompression, and internal fixation for the treatment of aggressive vertebral hemangioma with more than 5 years follow-up. So far, much experience is available with different treatments of aggressive vertebral hemangioma, and treatment approaches continue to improve. However, due to the great difficulty in operation, massive blood loss, high risk of recurrence, and other reasons, the therapeutic strategy has always been controversial. Radiotherapy, vertebroplasty, intravenous injection, embolization, and total en bloc spondylectomy, or any combination of them, have achieved varying degrees of success. According to our results, we believe that the treatment strategy of combined embolization, vertebroplasty is efficient and safe enough for most of patients. For special patients with severe fracture or instability, if such a strategy cannot be adopted, simple embolization with decompression, or vertebroplasty with decompression, is also competent. There were also some limitations in our study. First of all, this is a retrospective research and all patients came from a single center. In addition, the sample size was relatively small and there was inevitable bias from different choice of surgical methods for patients. Future, prospective, multicenter studies including more cases are needed to verify our results.
Footnotes
Acknowledgement
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work received support from National Natural Science Foundation of China (grant no. 81871804).