
Abstract
Study Design:
Retrospective database.
Objectives:
Although posterior decompression is the most common approach for surgical treatment of degenerative thoracic spine disease, anterior approach is gaining interest due to its advantage in disc visualization. The objective of this study was to compare the intra- and postoperative medical complication rates between anterior and posterior decompression for degenerative thoracic spine pathologies.
Methods:
A national US insurance database was queried for patients with degenerative diagnoses who had undergone anterior or posterior thoracic decompression. Incidence of intra- and postoperative complications were evaluated on the day of surgery and within 1 and 3 months. Two subgroups were matched based on age, gender, and comorbidity. The association of decompression approach and complications was assessed using logistic regression.
Results:
A total of 1459 patients were included, consisting of 1004 patients in posterior and 455 patients in anterior group. Respiratory complications were the most common complications on the day of surgery (8.57%) and within 30 days (17.75%). Matched analysis showed that anterior approach was associated with organ failure, gastrointestinal, and device-/implant-/graft-related complications in all follow-up periods; and with cardiovascular, deep venous thrombosis/pulmonary embolism, and respiratory complications in at least 1 follow-up period. Among respiratory complications, anterior decompression was significantly associated with noninfectious etiologies on the day of surgery (odds ratio [OR] = 1.72), within 30 days (OR = 2.05), and within 90 days (OR = 1.92).
Conclusions:
Anterior approach was associated with increased rates of several complications. High rates of respiratory complications necessitate comprehensive preoperative risk stratification to identify those who may benefit more from posterior approach.
Keywords
Introduction
Thoracic spine is unique in terms of biomechanical properties when compared with other spinal regions, particularly owing to differences in zygapophyseal joint angulation and the stability provided by rib cage in all primary movement directions. 1 -3 Despite the large number of studies on pathophysiology, epidemiology, and burden of degenerative disorders in cervical and lumbar spine, the literature on thoracic spine is scarce. Early reports estimate the annual incidence of thoracic disc herniation to be 1 per million capita. 4 Despite the relative rarity of symptomatic thoracic spine disorders, their diagnosis and treatment are challenging. Thoracic disc herniation commonly presents with radiculopathy and nonspecific pain, which are due to neural compression and increase in inflammatory cytokines. 5,6 However, atypical manifestations such as chronic abdominal pain, gastrointestinal symptoms, and cardiopulmonary presentations are not uncommon. 7 -10 These unusual presentations often overlap with other thoraco-abdominal pathologies and hinder a timely diagnosis. 7 -10
Historically, direct posterior decompression with laminectomy was used for surgical treatment of thoracic disc herniation. 5 This technique was associated with increased risks of iatrogenic spinal cord injury due to limitation of the space available for thoracic cord. 5,11 -13 Therefore, this approach was abandoned in favor of other methods. Current techniques for surgical decompression of thoracic spine are broadly categorized to posterior and anterior approaches, the former being the most common approach and the latter gaining increasing interest due to its advantage in disc visualization. Minimally invasive techniques have recently shown promise in reducing morbidity while offering similar exposure compared with conventional transthoracic approaches. 12,14,15 However, these techniques have been criticized due to their “steep learning curve,” in addition to the risk of iatrogenic injury to thoracic organs inherent to all transthoracic interventions. 12,16,17
Current literature on surgical treatment of thoracic pathologies is mostly limited to single approach studies, hindering in-depth comparison of outcomes and complications between different techniques. A recent meta-analysis of the literature showed that anterior and posterior approaches yield comparable results in terms of neurological worsening, re-operation rates, and overall neurological improvement, including the American Spinal Injury Association score, myelopathy, radiculopathy and pain. 18 Yet selecting the optimal surgical approach for treatment of thoracic degenerative pathologies is a dilemma. Considering the similarity of neurological outcomes, medical morbidity rates seem to be the key determinants of optimal approach. Therefore, the objectives of this study were to describe the incidence of complications following thoracic decompression for degenerative spinal pathologies, and to compare anterior and posterior decompression in terms of intra- and postoperative medical complications.
Materials and Methods
Patient Database
A private insurance database (Humana) was queried using the PearlDiver Patient Records Database (PearlDiver Technologies). This database covers over 68 million patient encounters in the United States and contains the medical records, including demographic characteristics, comorbidities, procedural data, drug prescription, outcomes and reimbursement data. Although the PearlDiver contained the patient data from 2007 to 2016, we restricted our query to the second quarter of 2015, in order to allow sufficient follow-up period. Current Procedural Terminology (CPT) codes were used to identify the potentially eligible patients who had undergone the surgical procedures of interest. International Classification of Diseases, Ninth Revision (ICD-9) codes were used to apply additional eligibility criteria (ie, the diagnoses), and to evaluate the risk factors, comorbidities and outcomes.
Eligibility Criteria
Details of the eligibility criteria and corresponding ICD-9 and CPT codes are presented in Supplemental Material 1. Patients who had undergone surgical decompression for degenerative pathologies in thoracic spine were eligible for inclusion. Those included posterior decompression with or without laminectomy, laminotomy, foraminotomy, or discectomy; posterolateral decompression including the transpedicular and costovertebral techniques; and anterior/anterolateral approach, including transthoracic, thoracolumbar, transperitoneal, and retroperitoneal approaches for corpectomy and anterior discectomy. Lateral extracavity approach was initially included in the query. However, after examination of the preliminary data, it was excluded due to small number of patients. Additionally, patients with combined anterior-posterior decompression were excluded. Surgical approaches were combined to make 2 cohorts of patients with either posterior or anterior decompression. Consequently, patients were screened based on the diagnostic criteria, and the following diagnoses were deemed eligible for inclusion: thoracic spondylosis, degenerative disc disease, spondylolisthesis and stenosis (Supplemental Material 1). Patients diagnosed with spinal infection, trauma, fracture, and benign or malignant spinal neoplasms were excluded (Supplemental Material 1).
Matched Cohorts
In order to eliminate the effect of potential confounders, 2 subsamples were matched one-on-one, based on age, gender, and the Charlson Comorbidity Index (CCI). CCI was used as a broad measure of comorbidity, and covers several categories of conditions, such as cardiovascular diseases, malignancies, and metabolic disorders. 19 Each comorbid condition receives a weighted score based on its severity, and scores are summed to generate a total comorbidity score. 19 Other background characteristics were initially considered for matching. However, addition of more factors in matching process would significantly decrease the sample size and thereby analytical power of matched comparisons. Therefore, logistic regression analysis was utilized to account for potential confounding effect of 3 clinically sensible factors: (1) smoking, which is the foremost risk factor for early complications following orthopedic and spine surgery 20,21 ; (2) diabetes as a systemic comorbidity with known association with complications following spine surgery 22 ; and (3) chronic obstructive pulmonary disease (COPD), due to its remarkable impact on complications of transthoracic surgery and emphasis of current literature on respiratory complications following anterior thoracic decompression. 23,24
Risk Factors, Comorbidities, and Complications
The database was queried for the following risk factors within 1 year prior to the index surgery: smoking, diabetes, and COPD (Supplemental Material 1). Intraoperative complications included accidental puncture/laceration of organs during surgery, excessive hemorrhage, surgical emphysema, and accidental dural laceration. Postoperative complications were assessed on the day of surgery, within 1 month, and within 3 months after the operation. These complications were categorized into the following groups: respiratory, cardiovascular, organ failure, central nervous system, wound, device-/implant-/graft-related, infectious, gastrointestinal, and deep vein thrombosis/pulmonary embolism. Respiratory complications were further classified to infectious and noninfectious subcategories.
Statistical Analysis
Statistical analysis was performed using R statistical package. Incidence of complications was reported using count and percentage. Other variables were described using mean and standard deviation (SD) or median (Mdn) and interquartile range (IQR) based on distribution. Comparison of CCI between the 2 cohorts was performed using the Mann-Whitney U test. Two subsamples were matched one-on-one, based on age, gender, and CCI. In order to evaluate the association of surgical approach with complications, logistic regression was performed using the data from matched groups, controlling for diabetes, smoking, and COPD as covariates. Odds ratios (ORs) with 95% CIs were calculated and Hosmer and Lemeshow test was used for assessment of goodness of fit. Models with P values >.05 for this test were considered well-calibrated. Other analyses were considered to be statistically significant if the P value was less than .05.
Results
Our database query initially identified 3365 patients who had undergone thoracic decompression. After exclusion of patients with combined anterior-posterior approach and application of diagnostic criteria, a total of 1459 patients (729 men, 49.97%) were included (Figure 1). The most common age group was 65 to 69 years with 317 patients (21.73%), and 810 individuals (55.52%) were older than 65 years. The surgical approach was posterior in 1004 (68.81%) and anterior in 455 (31.19%) patients. Cohorts were comparable with regard to history of COPD. Anterior group had a significantly higher number of smokers. However, the proportion of men, patients 65 years of age or older, diabetics, and patients with mean CCI score were significantly lower in this group (Table 1). Two subgroups from the study population were matched based on age, gender, and overall comorbidity (CCI), each consisting of 358 subjects. In each subgroup, 219 patients (61.17%) were men, and patients between 65 and 69 years of age constituted the most common age group (Figure 2). The proportion of patients with COPD was comparable between matched cohorts, and there was a trend toward significance with regards to smoking and diabetes status (Table 2).
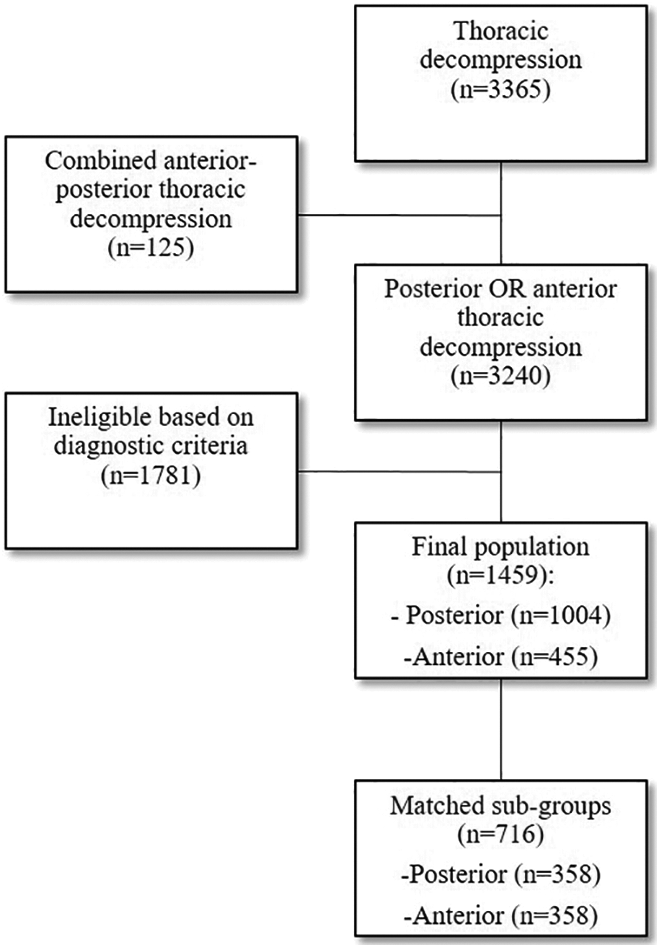
Patient selection process.
Demographic Characteristics and Comorbidities in Patients Undergoing Thoracic Decompression for Degenerative Thoracic Spine Diseases.
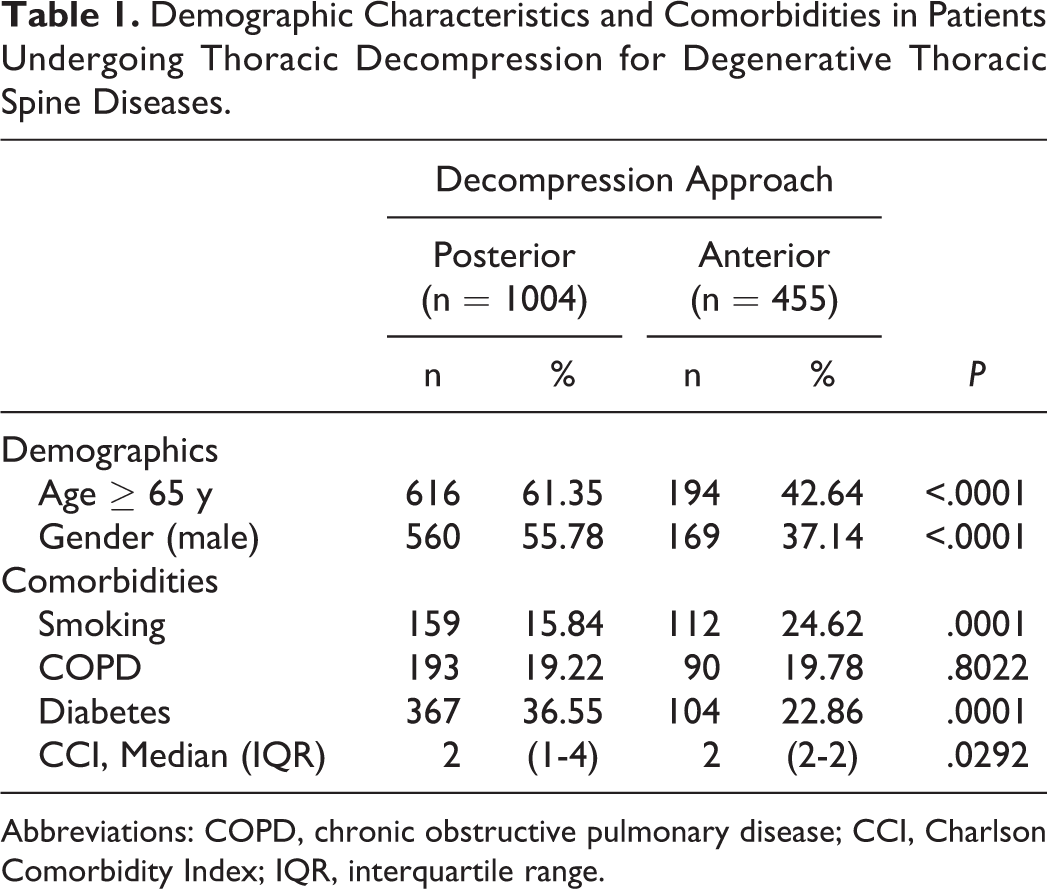
Abbreviations: COPD, chronic obstructive pulmonary disease; CCI, Charlson Comorbidity Index; IQR, interquartile range.
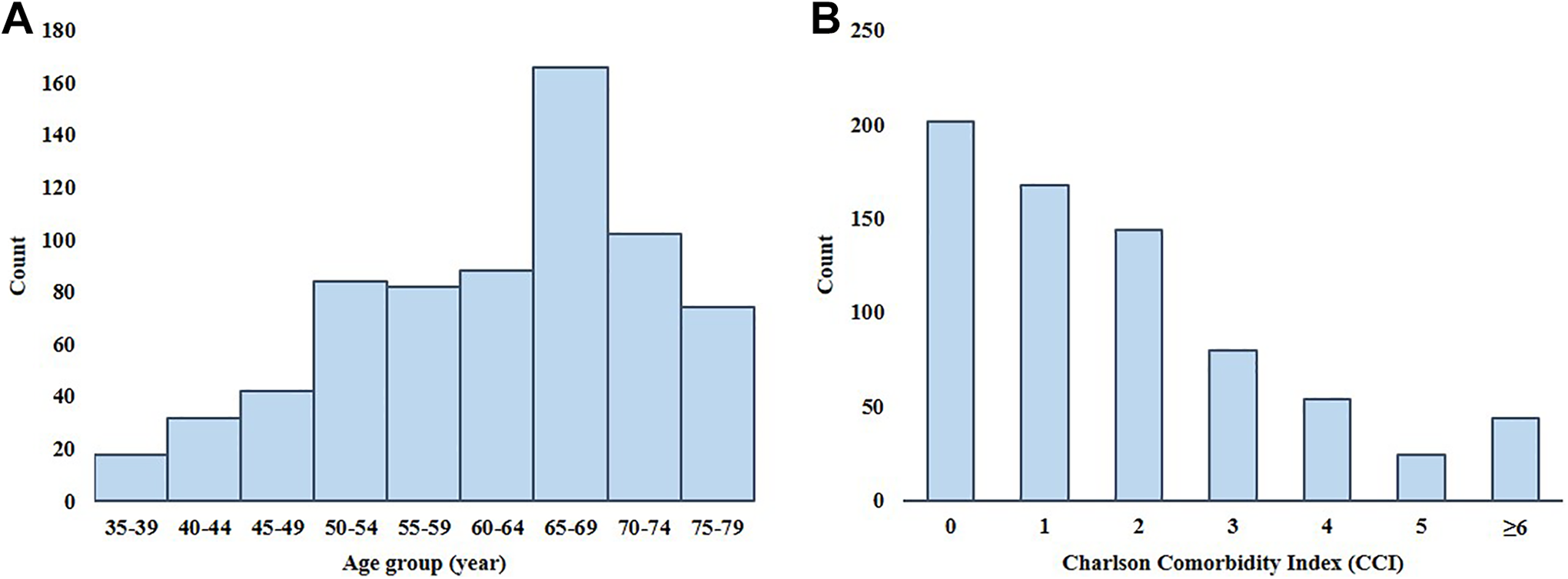
Distribution of age and Charlson Comorbidity Index in matched cohorts.
Comparison of Chronic Obstructive Pulmonary Disease, Diabetes, and Smoking Status Between the Matched Cohorts.
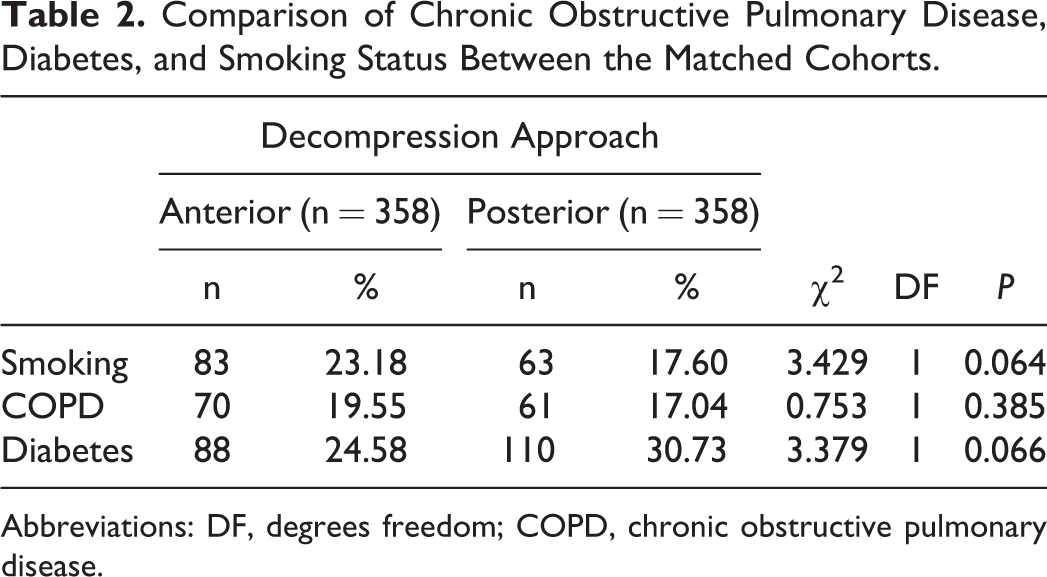
Abbreviations: DF, degrees freedom; COPD, chronic obstructive pulmonary disease.
Incidence of Complications
Incidence rates of complications following each surgical approach are presented in Table 3. Intraoperative complications occurred in 64 patients (4.39%), most commonly due to accidental dural laceration (n = 40, 2.74%). Among medical complications, respiratory complications were the most common adverse events on the day of surgery and within 30 days, with incidence rates of 8.57% and 17.75%, respectively. With 296 cases (20.29%), infectious complications were the most common category of adverse events within 90 days of surgery, followed by respiratory complications (n = 290, 19.88%) and major organ failure (n = 208, 14.26%). Hemodynamic complications were rare during the whole follow-up period.
Incidence of Intraoperative and Postoperative Medical Complications in Patients Undergoing Thoracic Decompression.
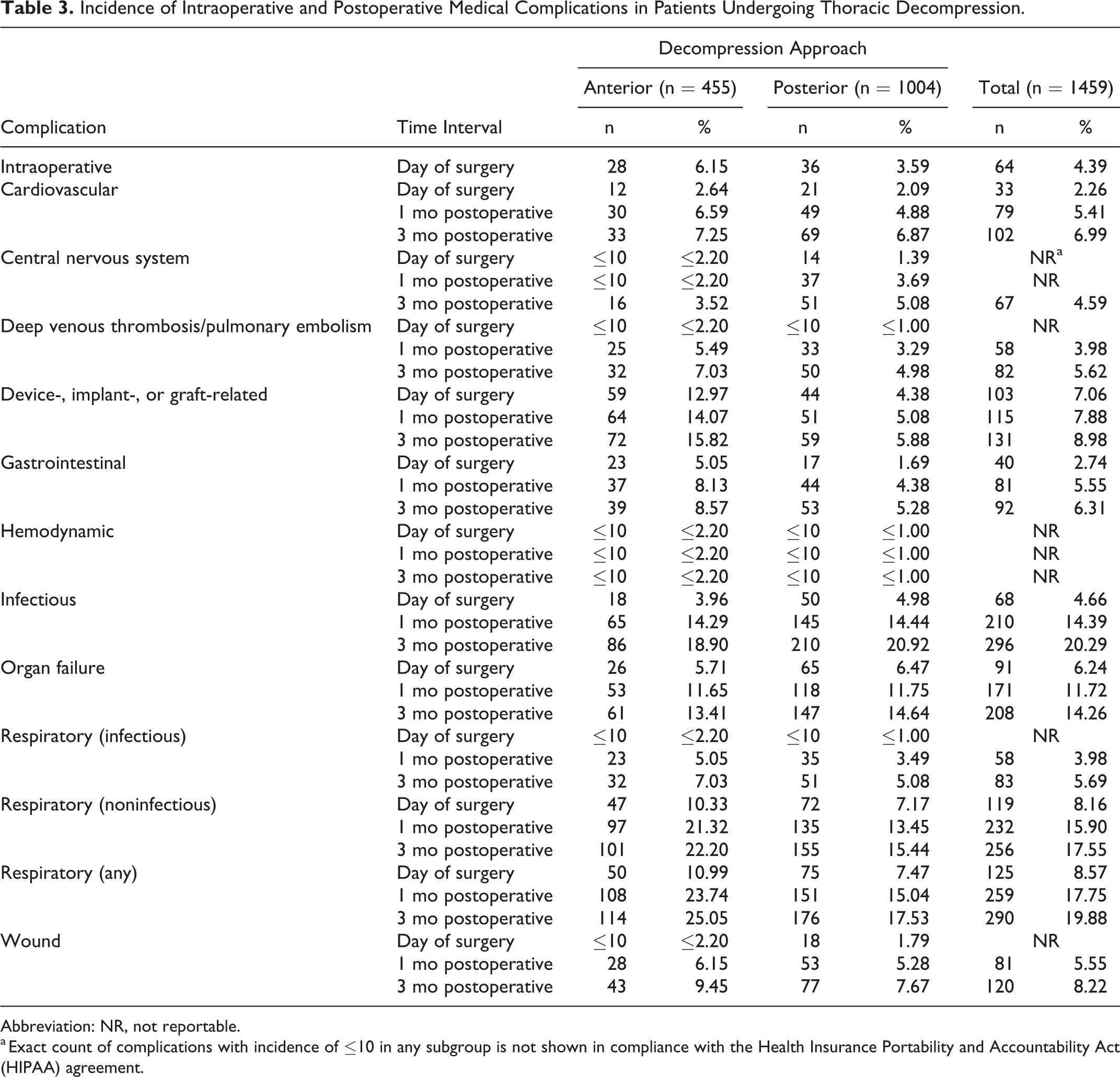
Abbreviation: NR, not reportable.
a Exact count of complications with incidence of ≤10 in any subgroup is not shown in compliance with the Health Insurance Portability and Accountability Act (HIPAA) agreement.
Association of Decompression Approach With Complications (Matched Cohorts)
Logistics regression analysis was performed with decompression as independent variable, complications as dependent variables, and diabetes, COPD and smoking history as covariates. In all three follow-up points, logistic regression revealed a significant association between the anterior decompression approach and organ failure, gastrointestinal, and device-/implant-/graft-related complications (Table 4). Furthermore, there was a significant association between anterior approach and cardiovascular, deep venous thrombosis/pulmonary embolism and total respiratory complications in at least one follow-up point (Table 4).
Association of Decompression Approach With Intraoperative and Postoperative Medical Complications in Matched Cohorts.a
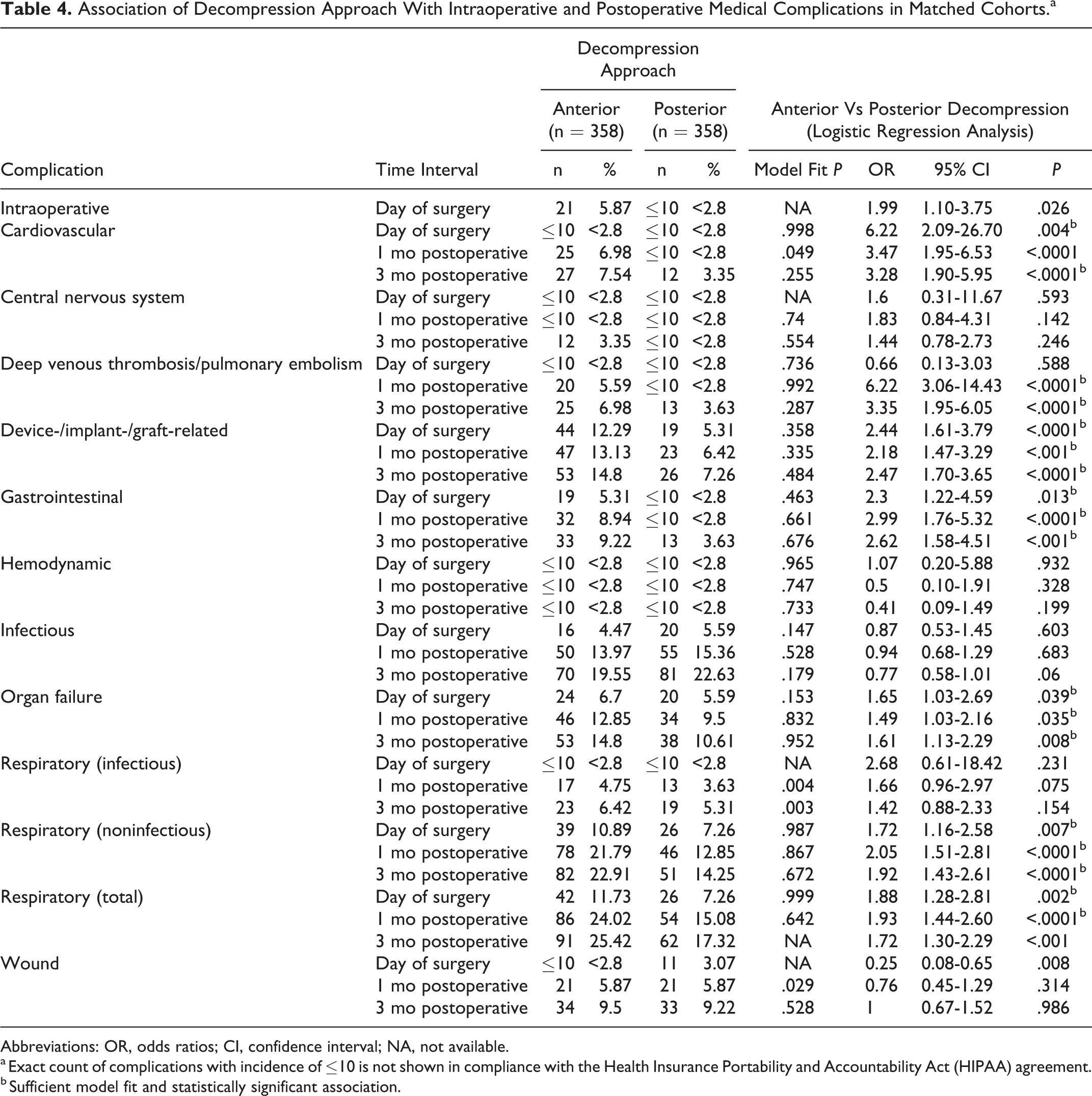
Abbreviations: OR, odds ratios; CI, confidence interval; NA, not available.
a Exact count of complications with incidence of ≤10 is not shown in compliance with the Health Insurance Portability and Accountability Act (HIPAA) agreement.
b Sufficient model fit and statistically significant association.
Among all complications, cardiovascular complications on the day of surgery and deep venous thrombosis / pulmonary embolism within 30 days of operation had the largest ORs following anterior decompression (both ORs = 6.22, P < .05). With regard to respiratory complications, anterior decompression was significantly associated with noninfectious respiratory complications on the day of surgery (OR = 1.72, 95% CI 1.16-2.58, P = .007), within 30 days (OR = 2.05, 95% CI 1.51-2.81, P < .0001), and within 90 days (OR = 1.92, 95% CI 1.43-2.61, P < .0001) following surgery. The model was underpowered to assess the association of surgical approach with infectious respiratory complications.
Discussion
Various surgical approaches are available for treatment of thoracic degenerative conditions. However, on account of low incidence rate of symptomatic thoracic degeneration and paucity of literature on this topic, selecting the optimal approach is challenging. The present study described the incidence of complications following thoracic decompression and revealed that anterior approach is associated with several major complications.
In agreement with current literature, posterior approach (68.81%) was the most common approach for thoracic decompression in this study. 18,23,24 This approach is considered advantageous in terms of neurological outcomes, safety, and length of hospital stay. 5,25 However, it can require extensive paravertebral muscle dissection and substantial bone resection, leading to increased postoperative morbidity. 12,25 Moreover, the posterior approach does not provide sufficient access for ventral dural decompression in central disc herniations. 25 -27
Anterior transthoracic approaches, including the trans-sternal, trans-pleural, and retro-pleural techniques 23 provide enhanced disc visualization, lower the risk of iatrogenic spinal cord injury, and preserve the integrity of posterior elements. 5,12,18,25 However, our study showed that patients undergoing anterior surgery are at significant risk of cardiovascular, gastrointestinal, respiratory, and device-/implant-/graft-related complications, as well as deep vein thrombosis/pulmonary embolism and organ failure. In a similar study focused on thoracic disc herniation, Yoshihara et al 24 compared the complications of anterior and nonanterior decompression using discharge data from the Nationwide Inpatient Sample (NIS) database. In their study, anterior approach was associated with higher overall rates of intrahospital complications (26.8% vs 9.6%). 24 Similar to our findings, they showed the association of anterior approach with several categories of complications, such as cardiac, respiratory, and gastrointestinal complications, as well as pulmonary embolism. 24 Furthermore, they found that anterior approach is more costly, and it is associated with higher mortality and longer hospital stay. 24 In both anterior and posterior groups, complications rates in our study were generally higher than Yoshihara et al. 24 This difference is in part due to dissimilarity of inclusion criteria and broader definition of complications in our study. Considering the short length of hospital stay of patients undergoing thoracic decompression, our longer follow-up seems to better estimate the true incidence of complications compared with the discharge data from the study by Yoshihara et al. 24
In this study, respiratory complications occurred in 19.88% of the whole study population within three months of operation. Postoperative pulmonary complications are estimated to cost up to $120 579 in surgical patients, and result in $7233 of additional costs in patients with spinal conditions. 28,29 Furthermore, respiratory complications are associated with significant increase in postoperative mortality, length of stay, and health care utilization. 30 The odds of respiratory complications on the day of surgery was 1.88 times larger in anterior group compared to the age-, gender- and comorbidity-matched cohort who had undergone posterior surgery, and this association remained significant within one month after surgery. This finding is in line with the fact that surgical interventions involving the thoracic cavity are inherently associated with higher risk of respiratory morbidities. 18 Surprisingly, the incidence of respiratory complications was considerably high in the posterior approach (17.53% within 3 months after posterior decompression), signifying the importance of preemptive respiratory measures in both approaches. Noninfectious etiologies constituted the majority of respiratory adverse events in both groups (Table 3) and included potentially life threatening complications such as pulmonary embolism and infarction, acute respiratory failure, lung edema, pulmonary collapse, and pneumothorax. The morbidity associated with pulmonary complications can be reduced by preoperative risk stratification, early detection, and intensive postoperative care. Even though several risk assessment measures exist, usefulness of current measures for thoracic spine surgery is unknown.
Limitations
Retrospective design is an important limitation of this study. Also, only few factors were considered in the matching process. However, addition of other potential confounders would decrease the sample size and thereby the power of our statistical comparisons. Three additional potential confounders were accounted for using logistic regression analysis.
Conclusion
Overall, anterior approach was associated with higher risks of postoperative morbidities, especially respiratory complications. Our future steps are to identify the predictive factors of respiratory compromise following thoracic decompression; to assess the morbidity, mortality, and costs associated with respiratory complications; and to develop a risk assessment score which may be used to identify the patients at risk of respiratory complications who may benefit from posterior decompression.
Supplemental Material
Supplementary_material_1 - Anterior Versus Posterior Decompression for Degenerative Thoracic Spine Diseases: A Comparison of Complications
Supplementary_material_1 for Anterior Versus Posterior Decompression for Degenerative Thoracic Spine Diseases: A Comparison of Complications by Aidin Abedi, Blake Formanek, Raymond Hah, Zorica Buser and Jeffrey C. Wang in Global Spine Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosures outside of submitted work: ZB-consultancy: Cerapedics, Xenco Medical (past), AO Spine (past); Research Support: SeaSpine (past, paid to the institution), Next Science (paid directly to institution); North American Spine Society: committee member; Lumbar Spine Society: Co-chair Research committee, AOSpine Knowledge Forum Degenerative: Associate member; AOSNA Research committee- committee member; JCW – Royalties – Biomet, Seaspine, Amedica, DePuy Synthes; Investments/Options – Bone Biologics, Pearldiver, Electrocore, Surgitech; Board of Directors - North American Spine Society, AO Foundation (20,000 honorariums for board position, plus travel for board meetings), Cervical Spine Research Society; Editorial Boards - Spine, The Spine Journal, Clinical Spine Surgery, Global Spine Journal; Fellowship Funding (paid directly to institution): AO Foundation; RH - NuVasive (consultant), The Spine Journal, Global Spine Journal, Clinical Spine Surgery (editorial board), North American Spine Society, Lumbar Spine Research Society (committees).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
The supplemental material is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.