
Abstract
Vertebral compression fractures remain an important cause of pain and debility. Intractable pain may be approached with vertebral kyphoplasty. We herein present a case of symptomatic pulmonary cement embolism following kyphoplasty. Discovery of a paravertebral cement venogram at the time of this procedure prompted a case series review of our institutional experience with kyphoplasty. We found that cement embolization, whether symptomatic or discovered incidentally, was universally associated with a cement venogram at the site of vertebroplasty. We propose that a cement venogram be viewed as a harbinger of cement pulmonary embolism and this possibility be considered in patients with an existing intracardiac shunt or who present with new respiratory symptoms soon after kyphoplasty.
Introduction
Vertebral compression fractures represent half of the osteoporotic bone fracture burden in the United States. 1 Conservative management focused on the bone disease, pain control, and physical therapy targeting core muscles causes improvement in most patients. For intractable pain, vertebral kyphoplasty augmentation may be offered. 2 In this procedure, methacrylate cement is injected to recover vertebral height and bolster bone integrity. We encountered a case of pulmonary cement embolization following vertebral kyphoplasty, which resulted from direct methacrylate migration into the paravertebral venous plexus. We sought to define how often embolization was heralded by the presence of a visible cement venogram
Index case and case series review
A 54-year-old man with a medical history of rheumatoid arthritis, chronic obstructive pulmonary disease (COPD), and vertebral compression deformities had persistent back pain despite conservative therapy. He presented with acute hypoxic respiratory failure following vertebroplasty 3 days before targeting T12, L2, and L5. The patient was tachypneic, tachycardic, and normotensive, with an oxygen saturation of 88% measured by pulse oximeter on a 5-L nasal canula. The patient was noted to have paravertebral cement extravasation on fluoroscopy at the time of the procedure. Computed tomography (CT) angiogram of the chest was obtained, which demonstrated bilateral subsegmental pulmonary artery cement embolization (Figure 1(a) and (b)). The review of the fluoroscopic record demonstrated a “cement venogram” at T12 (Figure 1(c)). The patient was managed conservatively with improvement in oxygenation at discharge.
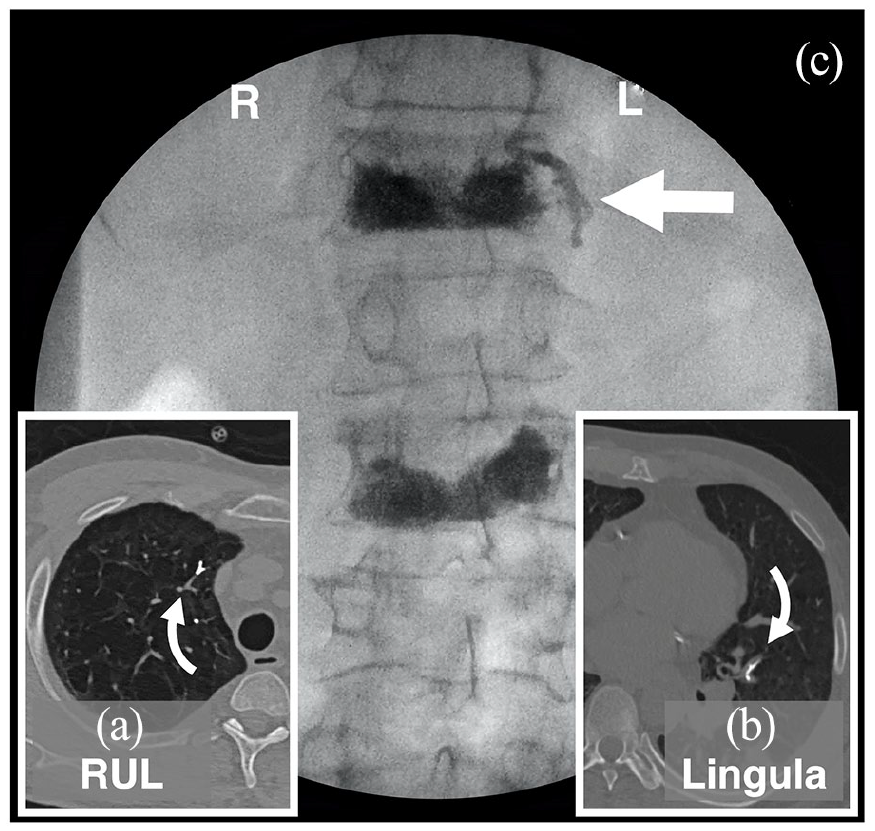
Cement venogram portends methacrylate embolism. The patient underwent kyphoplasty of T12, L2, and L5. He presented with acute hypoxic respiratory failure 3 days later. CT angiogram of the chest demonstrated multiple subsegmental pulmonary artery cement emboli (curvilinear arrows, a and b). He was noted to have cement venogram on fluoroscopy at time of the procedure (straight arrow, c). The patient was managed conservatively with improvement in oxygenation and discharge 2 days later.
Institutional review
A retrospective case series review of University of Iowa Health Care (UIHC) records was completed by Health Center Information Services (HCIS) using institutional-specific codes for kyphoplasty. The search was limited to current electronic medical records over the last 13 years and approved by the institutional review board (HawkIRB #202010430). Records were reviewed for patient demographics, underlying diagnosis, procedure logs, and associated imaging. Charts and outside records from linked healthcare systems (EPIC Everywhere) were scoured for chest CT imaging done from any time after the procedure. Imaging was personally reviewed for evidence of cement venograms and/or embolization. We defined these as linear or branching densities that were radio-opaque on CT scan “bone windows,” fell within the contour of paraspinal veins or pulmonary vessels, and new from prior imaging.
HCIS identified 178 procedures coded as balloon vertebroplasty or kyphoplasty with cement injection; 15 were excluded due to coding errors, duplicate orders, or the procedure having been canceled (Figure 2). The remaining 163 procedures were performed on 145 patients: 129 patients had one, 14 had two, and 2 had three separate procedures. The median age was 73 years, with 64% of patients being female. Over 90% of cases were caused by four comorbid illnesses: osteoporosis (50%), trauma (17%), multiple myeloma (14%), and other malignancies (12%). A total of 246 vertebrae were targeted as a single site in 100, two sites in 44, three sites in 18, and at four separate vertebral levels in a single case. Anatomic distribution of injected vertebrae was not uniform, with almost two-thirds of procedures directed at T11 to L3 (Figure 2).

Kyphoplasty case series from UIHC during 2008 to 2020: patient demographics and levels treated. Among the 93 cases for whom we had post-procedural chest CT imaging, we found 5 instances of pulmonary methacrylate embolism; all 5 were among the 12 cases in which there was a visible cement venogram at the site of injection (p < 0.001 vs no venogram by Fisher’s exact test).
Cement extravasation was either seen in 55 of the 163 procedures documented with fluoroscopy at the time of procedure or seen on follow-up imaging days to years later. The vast majority of these entered the inter- or paravertebral soft tissues. There was no documented cement extravasation into the spinal canal or neural foramina; there were no clinically relevant hematomas or neurologic dysfunction. For 95 cases, we had imaging of the procedure site and some form of follow-up chest CT imaging. In this group, there were 35 cases of documented extravasation of cement with 12 visible venograms. In seven of these cases, the venogram was seen only on CT. All venograms were in the paravertebral venous plexus and, in one case, extended into the azygous vein. There were no overt associations with venogram presence and the spinal level treated, underlying diagnoses, or operator; occurrences were distributed over the entire data collection interval. There was no association with the number of vertebra injected and the absence or presence of a cement venogram (mean ± SD: 1.52 ± 0.77 vs 1.67 ± 0.65, p = 0.48).
We found five cases of visible cement in the pulmonary arteries on chest CT scans. All 5 were among the 12 cases with visible cement venograms; no case of cement embolism was found in the 83 cases without venograms (p < 0.001; Fisher’s exact test). Retrospective chart review suggested these events were well tolerated. Two patients presented with cough and dyspnea days to weeks after vertebroplasty (inclusive of the case above). Both patients improved with empiric therapy aimed at a comorbid illness.
Discussion
Vertebral compression fractures remain important causes of pain and debility, with an aging population and prolonged cancer survival ensuring a persistent supply of cases. 1 Vertebral kyphoplasty remains an important tool in the management of compression fractures with pain intractable to more conservative measures. 2 As confirmed in our 163 cases spanning more than a decade, the procedure has a favorable risk/benefit ratio with no serious complications noted. Among nearly 100 cases with chest CT imaging, we identified 5 cases of cement pulmonary embolism. This is in line with the reported embolism rate of 3%–23%.3,4 All of the pulmonary emboli were associated with a visible, durable cement venogram in the paraspinal region near vertebral injection. Extravasation into the venous system during hip arthroplasty is postulated to result from cement administration pressure and volume rather than a patient-specific anatomic uniquity; procedural documentation in our records did not contain sufficient detail to parse potential contributing technical factors. 5 Pre-operative intraosseous venography with gel foam venous occlusion has been used to reduce extravasation, but is of unproven efficacy in reducing distal embolization.6– 8 This would be an informative area for future research.
Methacrylate embolism to the lung seems to be well tolerated.3,4 We found two cases where new respiratory symptoms occurred suspiciously proximate to kyphoplasty. Each improved with empiric supportive care. However, lethal cement embolization has been reported. 9 In addition, bone implantation syndrome is a multisystem organ failure associated with endovascular exposure to cure methacrylate cement and venous cement embolism. 10 This has been described most often after hip arthroplasty and may be related to a larger cement volume. Furthermore, paradoxical cement embolism to the brain has been described, raising concern in patients with known intracardiac right to left shunts. 11
Conclusion
Vertebral compression fractures are common and an important healthcare burden. Management of intractable debility may require interventions such as vertebral kyphoplasty. Interventional radiologists, neurosurgeons, and spine orthopedists may all perform these procedures, and their literature acknowledges complications associated with cement extravasation including central venous embolism. However, this may be less familiar to primary care providers and respiratory consultants. We propose the cement venogram be viewed as a harbinger of methacrylate pulmonary embolism, and this possibility be considered in patients with an existing intracardiac shunt or who present with new respiratory symptoms soon after kyphoplasty.
Footnotes
Acknowledgements
The authors would like to thank Keith Burrell, Clinical Applications Developer at UIHC HCIS for his tireless work in extracting the data for this study
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval to report this case series was obtained from the institutional review board (HawkIRB #202010430).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.