
Abstract
Background:
There is a common perception among surgeons that Asian tibiae are significantly more varus compared to non-Asians, contributed both by an acute medial tibial proximal angle (MPTA) and diaphyseal bowing. Insight into the normative morphology of the tibia allows generation of knowledge towards disease processes and subsequently planning for corrective surgeries.
Methods:
Computed tomography (CT) scans of 100 normal adult knees, aged 18 years and above, were analysed using a 3-dimensional (3D) analysis software. All tibiae were first aligned to a standard frame of reference and then rotationally aligned to the tibial centroid axis (TCAx) and the transmalleolar axis (tmAx). MPTA was measured from best-fit planes on the surface of the proximal tibia for each rotational alignment. Diaphyseal bowing was assessed by dividing the shaft to three equal portions and establishing the angle between the proximal and distal segments.
Results:
The mean MPTA was 87.0° ± 2.2° (mean ± SD) when rotationally aligned to TCAx and 91.6° ± 2.7° when aligned to tmAx. The mean diaphyseal bowing was 0.1° ± 1.9° varus when rotationally aligned to TCAx and 0.3° ± 1.6° valgus when aligned to tmAx. The mean difference when the MPTA was measured with two different rotational alignments (TCAx and tmAx) was 4.6° ± 2.3°. No statistically significant differences were observed between males and females. Post hoc tests revealed statistically significant difference in MPTA between different ethnic sub-groups.
Conclusion:
The morphology of the proximal tibiae in the disease-free Asian knee is inherently varus but not more so than other reported populations. The varus profile is contributed by the MPTA, with negligible diaphyseal bowing. These implications are relevant to surgical planning and prosthesis design.
Introduction
The concept of anatomic restoration of the knee has gained traction among knee surgeons in recent years. This approach would not necessarily restore the knee to what we regard as normal, but rather to its natural situation or pre-disease state. Indeed, what we conventionally thought of as normal, may contribute to an inferior outcome to a certain fraction of the population today. 1 In the correction of coronal plane deformities to this conceived normality, traditional surgical techniques tend to undercorrect in unicompartmental knee arthroplasty (UKA), 2 fully correct in total knee arthroplasty (TKA), 3 and overcorrect in high tibial osteotomy (HTO). 4 As newer studies argue to re-examine conventional goals, and follow the natural slope of the tibial surface in the coronal plane, 5 –7 a better understanding of normal anatomy is therefore a relevant prerequisite.
However, knowledge of normal mean values and variance in the Asian population is lacking. There is a long-held belief that the Asian tibia has more vara. 8 Recently, data reported described values comparable to Western counterparts. 9,10 These were performed using radiographs, which are dependent on limb positioning and thus subject to measurement errors. In addition, we were interested to know the incidence of diaphyseal bowing in the normal population, as we have come across patients in our clinic who have apparent bowing of their legs (Figure 1), but straight tibiae on radiographs. Asians are also thought to be more likely to have bowing of the tibial diaphysis. 11,12

Photograph of a patient whose tibiae appeared excessively bowed with corresponding radiograph.
Gaining insight into the anatomical orientation of the tibia is helpful in appreciating the load acting across the knee joint and its role in degenerative arthritis. Normative data may also provide some reference to the surgeon in preoperative planning and intraoperative decision-making, especially in patients with bilateral disease. Plain radiographs have limitations due to parallax and errors inherent with positioning. Limb rotation and flexion attitudes affect the radiographic angular measurements of limb alignment. 13 For this reason, recent studies utilise CT. 14
Therefore, the aims of our study were (1) to measure the slope of the tibial surface in the coronal plane, quantified as the medial proximal tibia angle (MPTA), in normal Asian knees using 3-dimensional (3D) computed tomography (CT) scans, (2) to determine the frequency of diaphyseal bowing and (3) to identify the effect of rotational positioning of the tibia on the above two measurements.
Materials and methods
CT scans of 100 knees from 100 patients were retrospectively reviewed and analysed using a 3D analysis software, Mimics version 14.0 (Materialise Inc., Belgium). These patients, who were 18 years old and above, had undergone CT angiogram of the lower limb for vascular disease or injury and had no radiological evidence of osteoarthritis. Prior to commencement of the study, ethics approval was obtained from the medical research ethics committee of our institution. We have a multi-ethnic population that consists of descendants from various regions of Asia and thus our study reflects Asia as a whole. Chinese descendants (East Asia), Indian descendants (South Asia) and the Malays (South East Asia) made up 25%, 38% and 37% of the study population, respectively.
Alignment of the tibia
A standard frame of reference was established at the start for reliable measurement with good reproducibility. The 3D reconstructed tibia was aligned in a constant manner. 15 Firstly, the tibia was aligned to its anatomical axis (TAAx) in the coronal and sagittal planes. To achieve this, the centre of the ankle and the centre of the proximal tibia were defined, its axis being a line which connected these two points. The articular surface of the tibial plafond and the inner articular surfaces of the medial and lateral malleoli of the ankle were marked to locate the centre of the ankle by a best-fit sphere algorithm (Figure 2). The centre of the proximal tibia was determined by projecting a locus of centre points of the endosteal medullary tube of the proximal tibia to the surface of the tibial plateau as a single point (Figure 3).

Determination of the centre of the ankle by a best-fit sphere algorithm.
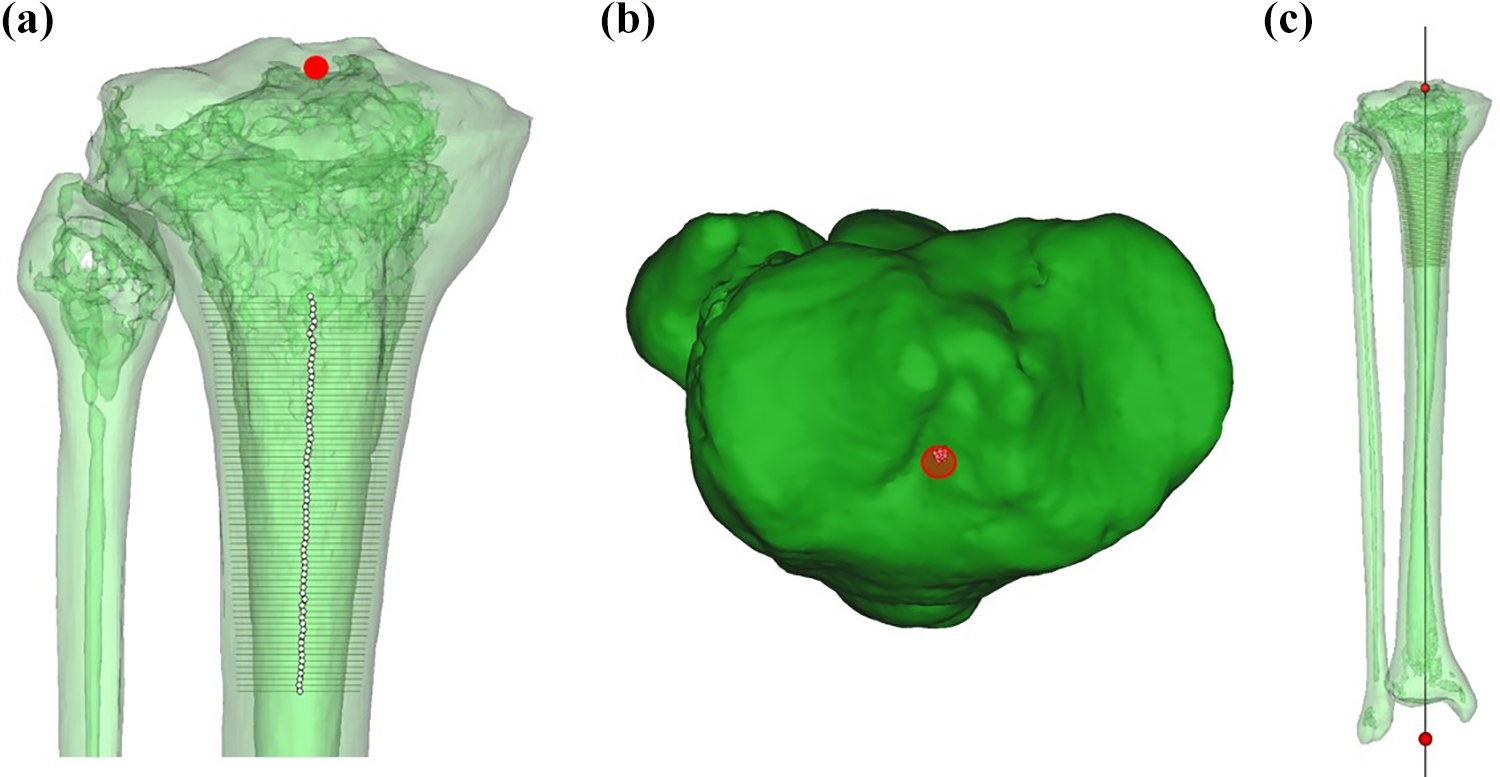
(a and b) Identification of the centre of the proximal tibia. (c) The 3D reconstructed tibia has been aligned to its long axis in the coronal plane.
Once aligned in the coronal and sagittal planes, the tibia was rotationally aligned. Initially, the tibia was aligned to the tibial plateau using the tibial centroid axis (TCAx). The TCAx is a line connecting two centroids, which were calculated by the software from individually marked surfaces of the medial and lateral tibial plateaus (Figure 4(a)). After measurements were made, the tibia was then rotationally aligned to the ankle using the transmalleolar axis (tmAx), which is a best-fit line connecting the inner surfaces of the medial and lateral malleoli. This aligned the tibia in such a way that the ankle points forward, a common reference used in surgery (Figure 4(b)). Thereafter, measurements were repeated.

(a) Rotational alignment of the tibia to the tibial plateau: After the tibia is aligned to the tibial centroid axis (TCAx), a line perpendicular to the TCAx points directly anterior. (b) Rotational alignment of the tibia to the ankle: A line (line d) perpendicular to the transmalleolar axis (tmAx) is derived from the confluence of two planes passing through the centre of the ankle. Once rotationally aligned, line d points directly anterior.
Measurements
MPTA was measured as the medial angle between the proximal tibial joint line and the axis of the tibia. The proximal tibial joint line, which is the tangent of the articular surface of the proximal tibia, was derived from planes which were created by best-fit algorithm to the combined marked surfaces of the medial and lateral tibial plateaus (Figure 5).
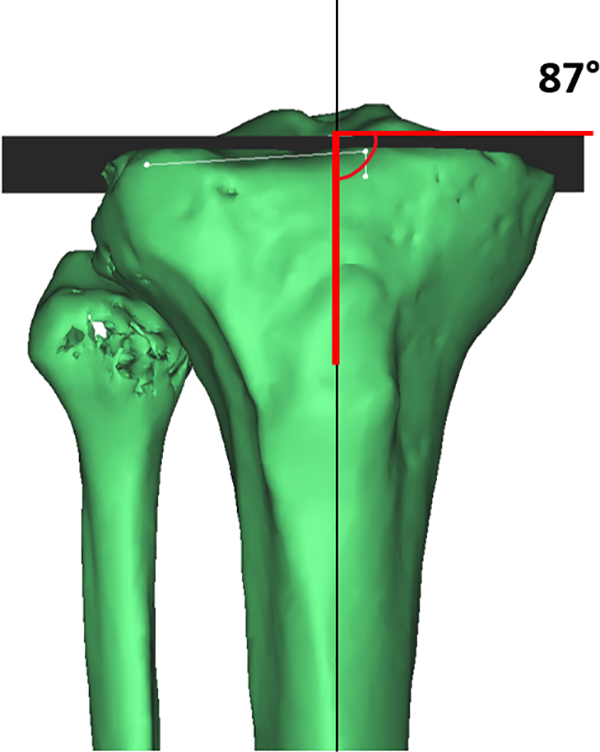
Measurement of the medial proximal tibial angle (MPTA).
Extra-articular tibial bowing or tibial bowing arising due to angulation at the diaphysis was determined in our CT study using a method adapted from that of a radiographic study by Yau et al. 12 To identify the tibial diaphysis, the rule of the square was applied, whereby a square whose sides are the same length as the widest part of the epiphysis was drawn at the proximal and distal ends of the tibia. These squares defined the proximal and distal metaphyseal segments of the tibia 16 and the area in between was the tibial diaphysis (Figure 6(a)). Subsequently, the tibial diaphysis was divided into three equal portions and a line that equally bisects the endosteal canal was drawn in the proximal and distal thirds (Figure 6(b)). Bowing was then expressed as the angle between the axes of the proximal and distal thirds of the tibia.

Measurement of diaphyseal bowing. (a) Identification of the tibial diaphysis by the rule of square method. (b) The tibial diaphysis has been divided into three equal portions. Bowing was measured as the angulation between two lines that bisects the proximal and distal segments, respectively.
Statistical analyses
Data was analysed using SPSS (version 21, IBM, Chicago, IL, USA) and statistical significance was defined as p < 0.05. Normality testing was performed, and variables of both datasets were compared and examined with the appropriate statistical tests. The relationship between variables was determined using the Pearson correlation coefficient (r). Intraclass correlation coefficient (ICC) was applied to measure interobserver agreement. A co-author repeated the entire process from alignment to measurement in 30 subjects.
Results
There were 52 men and 48 women (100 individuals; mean age 54 years, range, 18 to 81) who contributed 100 knees in this study. The mean MPTA was 87.0° ± 2.2° (mean ± SD) when rotationally aligned to the tibial plateau (TCAx) and 91.6° ± 2.7° when aligned to the ankle (tmAx). The mean difference when the MPTA was measured with two different rotational alignments (TCAx and tmAx) was 4.6° ± 0.8° and this was statistically significant (p = 0.001).
The mean diaphyseal bowing in our study population was 0.1° ± 1.9° varus when rotationally aligned to the tibial plateau (TCAx) and 0.3° ± 1.6° valgus when aligned to the ankle (tmAx). The mean difference when diaphyseal bowing was measured with two different rotational alignments (TCAx and tmAx) was 0.4° ± 1.4° and this was statistically significant (p = 0.006) but small. Further details for both MPTA and diaphyseal bowing are given in Table 1. MPTA and diaphyseal bowing were variable in our study population (Figure 7).

Histograms depicting MPTA (a) and diaphyseal bowing (b).
Measurement results of MPTA and diaphyseal bowing.a
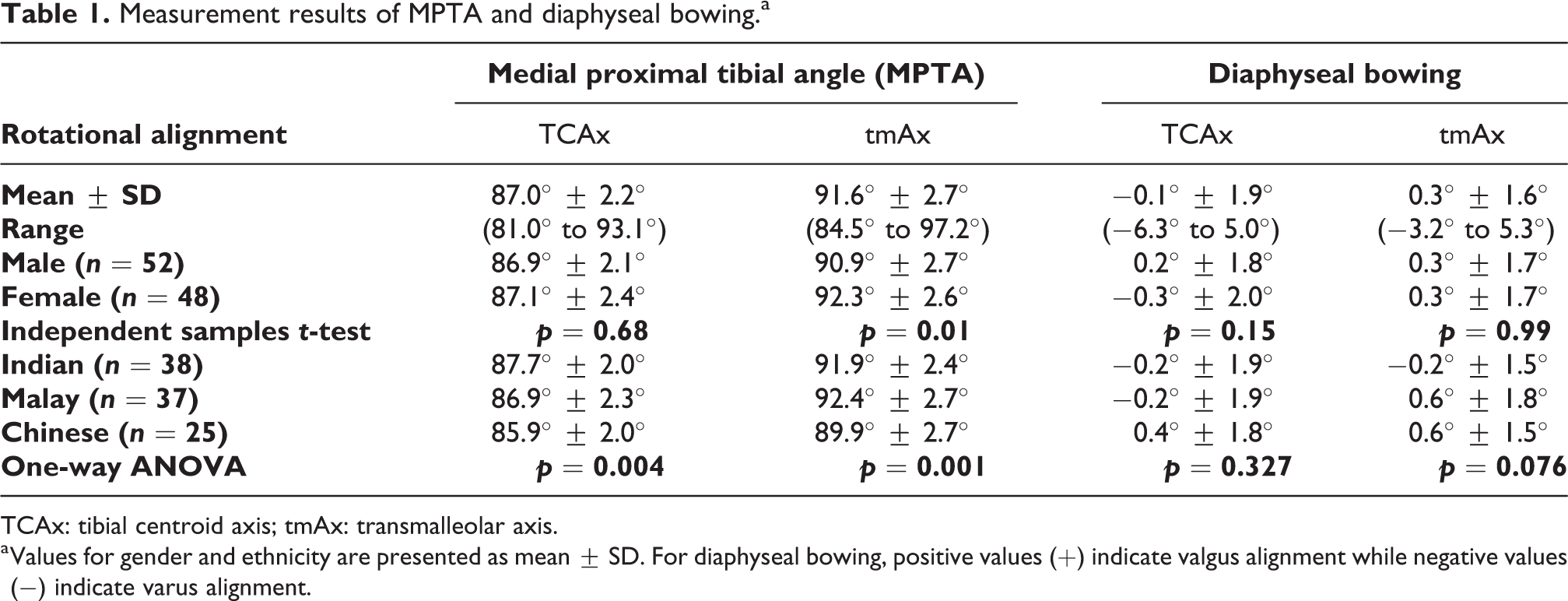
TCAx: tibial centroid axis; tmAx: transmalleolar axis.
a Values for gender and ethnicity are presented as mean ± SD. For diaphyseal bowing, positive values (+) indicate valgus alignment while negative values (−) indicate varus alignment.
Comparison with other published works.a

CT: computed tomography; TAAx: tibial anatomical axis; TCAx: tibial centroid axis; NA: not available; TMAx: tibial mechanical axis; PCA: posterior condylar axis; M: male; F: female.
a For diaphyseal bowing, positive values (+) indicate valgus alignment while negative values (−) indicate varus alignment.
No statistically significant differences were observed between males and females for all measured values with the exception of MPTA when rotationally aligned to the ankle (tmAx, p = 0.01). There was no correlation found between all these variables and age. When ethnicity was compared for measured MPTA values, there was significant difference between groups, as determined by one-way ANOVA (p = 0.004 (TCAx), p = 0.001 (tmAx)). Post hoc tests using the Bonferroni correction revealed that the MPTA among the Chinese in our study population was significantly less than the Indians (p = 0.003) but not the Malays (p = 0.157), when rotationally aligned to the tibial plateau (TCAx). When rotationally aligned to the ankle (tmAx), the MPTA among the Chinese was significantly less than both the Indians and the Malays (p = 0.008, p = 0.001 respectively). However, there was no difference observed between ethnic groups for diaphyseal bowing (p = 0.327 (TCAx), p = 0.076 (tmAx)).
All of the interobserver repeated measurements were within 2°. The Intraclass Correlation Coefficient (ICC) for all measurements were 0.96 which show excellent agreement.
Discussion
Procedures involving the modification of knee alignment, either through osteotomies or joint arthroplasty requires a lot of thought and planning. Unlike the other weightbearing joints, the range of target angles for the desired alignment around the knee is small and hence the propensity for errors is larger. The knee joint is also more dependent on soft tissues to provide strength, flexibility and stability, so the effect of these alignment changes on the soft tissues needs to be taken into account.
This study has several limitations. First, the sample size was 100 subjects and this should be accounted for when interpreting the results. However, the study population has equal proportions of subjects according to gender, age and ethnicity. Second, this is an observational study performed on normal, healthy knees and thus includes no correlation with diseased knees. Third, a direct comparison between Asians and Caucasians would require further study utilising similar methodology. Previous studies employ different rotational standardisation methods, and as we have shown, different rotational alignment results in different readings. Finally, although there are statistically significant differences shown in our results, most of these differences are too small to be clinically significant. This should be kept in mind when utilising the data for analysis or for surgical consideration.
The general impression is that Asian patients have more varus of the tibia, therefore have a higher risk of eccentric loading and arthrosis of the knee. Multiple studies have shown that the prevalence of knee osteoarthritis (OA) is higher among the Asian population. 17 –20 Bellemans et al. 1 reported that out of 500 limbs studied in normal, healthy, Caucasian subjects between the age of 20–29 years old, had a mean MTPA of 87.04 ± 2.07°. The Asian equivalent study by Tang et al. 8 studied the Chinese population and demonstrated that the mean MPTA was more acute by about two degrees. More recently, Shetty et al. 10 analysed the long limb radiographs of 388 healthy, adults between the age of 20–40 years old. Their sample consisted of 100 Indian participants and 94 Korean participants. They found that the MPTA was 86.7 ± 1.9° in this population. The mean MPTA (using TCAx as the rotational reference) in our study was 87.0 ± 2.2°, with males having more varus compared to females, which is consistent with previously reported data (see Table 2). In fact, our mean MPTA is less acute when compared to a study on western population by Jamali et al. 14 In their study however, reference for the coronal plane and hence the rotational axis of the tibia was based on the most posterior aspect of the greater trochanter and femoral condyles, akin to resting the femur on a virtual table top.
The presence of tibial bowing also influences the tibial inclination, in addition to limiting the surgical options available for the patient. Previous studies 11,12 reported that 30–43% of tibia in ethnically Chinese patients had bowing of more than two degrees. Ko et al. 21 demonstrated that a 8 mm wide, 25 cm long intramedullary rod could not be templated onto 54% of patients due to presence of varus tibial bowing. Our sample patients demonstrated minimal, clinically insignificant tibial bowing, even when measured in different rotational references. Our study, with a high degree of certainty demonstrates that the tibia in our population is straight.
Radiographic studies have a higher likelihood of measurement error as radiographs cannot accurately measure or correct for inconstant positioning of the limb during the study. Our study utilises 3D CT images and hence we are able to standardise rotation of the images by post-processing and realigning the tibia to fixed landmarks. Lonner et al. 13 demonstrated statistically significant changes in the perception of limb alignment. Limb radiographs projected in more external rotation causes more apparent varus and vice versa. This was again demonstrated by Jamali et al., 14 by measuring limb alignment angles from different rotational profiles. The posterior tibial slope is projected onto the coronal plate with rotation and thus the MPTA will appear more acute with the incorporation of the medial posterior tibial slope (external rotation) and less so with the lateral slope. Similarly, our results show that with a different rotational reference (tmAx), the MPTA will read more valgus than when measured using TCAx.
When critically analysing ethnic breakdown, the ethnic Chinese individual has a larger varus inclination among the three ethnicities. This is consistent with our anecdotal impression that the prevalence of OA is higher in the Chinese population. It has been postulated that vitamin D deficiency is a risk factor for the development of knee deformities. However, results from multiple cross-sectional studies have shown that Chinese patients have significantly less risk of hypovitaminosis D both during adolescence or adulthood. 22,23 This warrants further study to examine the correlation between vitamin D deficiency and tibia vara.
Clinically, when considering osteotomies around the knee, planning of the desired correction traditionally relies heavily on the correction of the resultant Mikulicz line to cross the tibial spine. 24 However, for significant varus malalignment, large corrections can result in excessively high MPTA, which may lead to an overly vertical joint line. 25 Coventry proposed an acceptable knee joint line obliquity to be less than 10° to prevent excessive shear stresses on the joint. 26 Analysis of preoperative joint line obliquity is essential in the planning of an osteotomy in order to prevent an overly oblique joint line. An acceptable resultant MPTA after an osteotomy should not excessively deviate from that of the normal population. Thus, in our population setting, it would be wise not to exceed a postoperative MPTA of 92 degrees, two standard deviations from our mean MPTA. Simultaneous osteotomies of the femur and tibia may be considered to ensure that in realigning the Mikulicz line, the resultant joint line obliquity is in the acceptable range during single leg stance.
The implications in TKAs are multiple, one of which is the rotational alignment of the femoral component. In order to create a rectangular flexion gap, surgeons need to consider the medial inclination of the tibial plateau and the integrity of the collateral ligaments. 27 The customary component position is at three degrees external rotation, signifying the alteration of the ‘native’ tibial inclination from three degrees to zero degrees for the tibial component. In our population sample, the mean tibial inclination as demonstrated from the MPTA shows that the average rotation needed for symmetrical collateral ligament tension in flexion will follow the conventional three degrees.
When performing TKAs, there may be an argument to accept more varus angulation of the tibial component in a certain subset of patients. Lee et al. 28 has studied the effects of malalignment on survivorship of total knee arthroplasties (TKAs) and they found that placement of femoral component in varus has a larger influence on the long-term outcome of TKAs. Nevertheless, excessive varus malalignment of a TKA has been shown to be detrimental to its longevity 29 although the exact acceptable range remains controversial. 30 –32 Based on our findings, if the intention is a more kinematically or anatomically positioned component reflective of the pre-diseased state, we found no reason to alter the desired coronal alignment for the planning of TKAs in Asians.
Similarly, certain recent TKA prosthetic designs have intended to restore normal knee kinematics by replicating the normal pattern of tibiofemoral motion throughout the range of motion of the knee and increasing the sagittal plane stability throughout knee flexion. 33,34 One of the features of these designs is a more physiological joint line, whereby the lateral tibial compartment is thicker and more convex than the medial compartment. The complementary femoral condyle is less thick laterally than the medial side, which effectively creates a three degrees medially sloped joint line. Considering the mean magnitude of tibial varus inclination in our population is comparable to others, these implant designs principles can be applied to prosthesis targeting the Asian knee.
Intraoperatively, when rotationally aligning the tibial cutting jig, referencing different rotational axes can significantly affect the varus cut angle. In our study, the mean difference when the MPTA was measured with two different rotational alignments (TCAx and tmAx) was 4.6° ± 0.8°. Determining the coronal placement of the jig, especially when re-creating the posterior tibial slope in cruciate retaining knees, requires one to be wary of the rotational placement of the cutting jig. Excessive external rotation of the jig may impose a ‘posterior’ slope into the coronal plane, which may result in errors of the cut surface of the tibia. 35 Using the centre of the ankle is akin to using the tmAx as a rotational landmark for the coronal plane, and this effectively external rotates the position of the cutting jig. A cut surface which appears perpendicular in this plane will be in fact, slightly more varus when redressing the rotation based on the proximal tibial anatomy.
With respect to diaphyseal bowing of the tibia, multiple authors have described presence of significant angulation between the proximal and distal diaphyseal axes of the tibia. 12,36 These studies imply that the utilisation of intramedullary guidance for placement of tibial cutting jig may lead to higher rates of unacceptable deviation in prosthesis alignment. In addition to that, this implies that surgeons need to be especially careful not to cause a distal fracture when using long stemmed implants in Asian patients.
The tibiae in our population did not display any significant bowing therefore use of intramedullary alignment guidance for tibial cuts should provide accurate jig placement with minimal errors. However, we do recognise that Asians tend to present a lot later in the disease process and in arthritic patients with severe varus deformities of more than 10 degrees, there is a discrepancy in the anatomical and mechanical axis of the tibia. 37,38 Further studies is warranted to determine the frequency of such deformities and whether it develops as part of the disease process of osteoarthritis.
Conclusion
The MPTA of the normal, non-degenerated adult Asian knee is 87° with a reference range of 85°–91° (mean ± 2 standard deviations). The contributors of tibia vara in Asians are the MPTA, with no observed diaphyseal bowing in our study population. This CT based study thus contributes to existing studies of normative data of coronal inclination of the proximal tibia.
Footnotes
Acknowledgement
The authors thank Shuen Yu Mo who contributed towards the acquisition of data.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the University of Malaya (RG476-12HTM).