
Abstract
Focal fibrocartilaginous dysplasia is an uncommon benign bone condition that predominantly affects children and typically leads to varus deformities in the proximal tibia. It was first described by Bell in 1985. The etiology remains unknown and the diagnosis is radiological; biopsy is not necessary. We present a case of a 2-year-old child who presented to our department for a right limb varus deformity caused by focal fibrocartilaginous dysplasia.
Introduction
Focal fibrocartilaginous dysplasia (FFCD) is a relatively uncommon benign bone condition that predominantly affects children. While there are limited cases documented in the literature, various bones such as the tibia, femur, ulna, humerus, radius, phalanx, and vertebra have been reported as sites of occurrence. 1 Among these, the tibia is considered the most frequently affected location, often resulting in varus deformities. The exact causes of FFCD and the mechanisms underlying the deformities are not yet fully understood.
In some patients, spontaneous resolution of the condition may occur, while in others, the deformities persist or progress over time. The optimal treatment approach, whether surgical or conservative, remains a subject of debate. In this report, we present the case of a two-and-a-half-year-old child who presented with a progressively worsening varus deformity in the proximal right tibia.1,2
Case
We present the case of a 2-and-a-half-year-old boy born to non-consanguineous parents via vaginal delivery without any reported traumatic incidents. The child has shown normal psychomotor development and has no history of trauma or infection. However, the parents observed a deformity in the right limb as their child learned to walk.
Upon clinical examination, a unilateral varus tibial deformity was observed in both standing and lying positions, with a shortening gap of 3 cm and an inter-malleolar distance estimated at 6 cm, with no tibial torsion. The rest of the somatic examination was unremarkable (Figure 1).
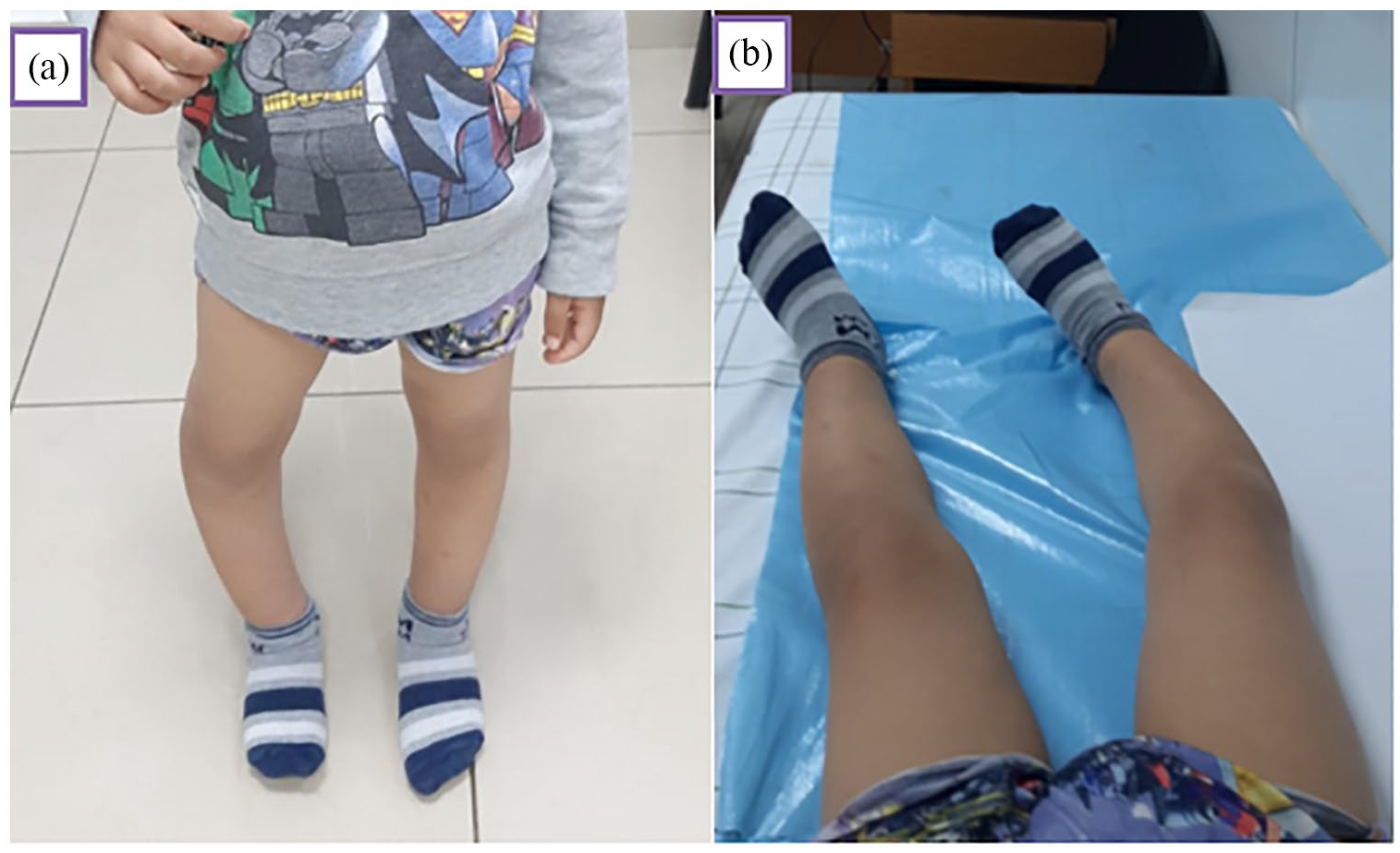
Standing (a) and supine (b) photos of a two-and-a-half-year-old child depicting the varus deformity in the right lower limb.
Radiographic alignment analysis revealed a right genu varum (hip–knee angle 146°).
The varus was tibial. The center of rotation of the angulation (CORA) was around a medial diaphyseal–metaphyseal level.
At the CORA level, there was a lacunar zone surrounded by a halo of cortical condensation (Figure 2).

Standing X-rays (a) and axial, coronal section of a scan (b, c) of both lower limbs revealed a varus deformity in the right tibia, characterized by a medial defect surrounded by osteocondensation in its proximal third ( white arrow). The deformity measured 34°, and the right tibia was found to be 6 mm shorter compared to the contralateral side.
Further CT scans revealed at the CORA level a lacunar lesion surrounded located by a marginal sclerosis, while maintaining the integrity of the adjacent soft tissues; the bone structure was otherwise normal (Figure 2).
Our patient underwent orthopedic treatment with an articulated anti-varus cruropedic orthosis for 12 months, with a slow, gradual reduction in the varus angle. X-rays are scheduled until the end of his treatment.
Discussion
This is a case of fibrocartilaginous dysplasia (FCD) in a 2-year-old boy. This case is unique as the diagnosis was made early, allowing us to perform orthopedic treatment with satisfactory results.
FCD is a rare form of fibrous dysplasia, primarily affecting long bones and was initially described by Bell et al. in 1985. It is a rare condition that accounts for unilateral tibia vara in children, typically involving the medial aspect of the tibial metadiaphysis. Children with FFCD usually present between the ages of 12 and 24 months. The main pathological feature of this condition is the presence of a thick fibrotic band that extends from the epiphysis to the metaphysis on one side of the bone. It is believed that this band acts as a tether, causing asymmetric growth and angulation. According to Bell et al., there is a suggestion that the mesenchymal anlage of the tibial metaphysis develops abnormally, resulting in excessive fibrocartilage production. 3 This abnormal fibrocartilage formation then disrupts the normal bone growth on the medial aspect of the proximal tibia.
Until now, a limited number of cases have been documented in the available literature. These cases involve various bones such as the tibia,1,4 femur,5,2 ulna,6,7 humerus, 7 radius, 8 phalanx, 5 and vertebra. 9 Among these reported cases, the proximal tibia is recognized as the site that is most commonly affected.
Children typically exhibit symptoms of unilateral tibia vara, slight leg shortening, and distinct walking abnormalities, as reported by parents, between the ages of 12 and 24 months. In cases where they have reached the age of standing, hyperextension of the knee may also be observed. However, patients with involvement of the upper limbs generally present at later stages, usually at older ages. 10
The signs observed on conventional radiography are typically clear enough to eliminate the need for additional investigations. A characteristic finding is an obliquely directed medial cortical gap located in the metaphyseal–diaphyseal region of the upper third of the tibia. This gap does not appear well-defined on its superior-medial side, while its lateral side is surrounded by reactive marginal sclerosis that extends to the upper two-thirds of the bone shaft. Varus angulation often occurs at the location of the cortical gap. 11
Histopathologically, there exists a range of features, varying from purely fibrous lesions to those that contain hyaline and fibrocartilage. However, the radiographic features often exhibit distinctive characteristics, which typically eliminate the need for a biopsy. 12
In certain patients, the deformity can be resolved through treatment methods such as splints, braces, or shoe elevation. 13 However, spontaneous resolution is also observed in some cases without any intervention. 14
In the majority of patients who underwent surgical treatment, including procedures such as fibrous band release, curettage, guided growth, osteotomy, or a combination of different surgical techniques, clinical and radiological healing was achieved at the last follow-up.14,15 However, in some cases, incomplete correction or overcorrection occurred following osteotomy or guided growth procedures. 14 Ultrasonic osteotomes, due to their ability to selectively cut hard bony tissue rather than soft tissue, were chosen to minimize adverse effects. 16
Conclusion
Focal fibro-cartilaginous dysplasia of the tibia is a rare, benign condition that causes proximal tibial varus. Radiological findings are sufficient to make the diagnosis.
Treatment includes orthopedic methods (orthoses, etc.) with good progression, while surgical treatment may be considered in complicated cases.
Footnotes
Acknowledgements
I would like to express my gratitude to my professors and all the colleagues who participated in the completion of this work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the parents of the patient for the publication of this case report.
Guarantor of submission
The corresponding author is the guarantor of submission.