
Abstract
Background:
Infantile tibia vara is an acquired form of tibial deformity associated with tibial varus and internal torsion. Several methods have been described for orthotics treatment. The purpose of this study was to determine the effectiveness of orthotics treatment in infantile tibia vara.
Study design:
Controlled trial.
Objective:
The aim of this study was to compare the effect of different types of orthoses and correction methods on decreasing the curve in children with severe genu varum.
Methods:
Three different types of knee–ankle–foot orthoses were applied to 35 lower extremities of 22 pediatric participants who were 19–38 months of age. The same orthotic design principles were used to correct the femur, while different designs were applied to correct the tibia. The orthoses used on 20 participants were evaluated for differences among them and their effects on the treatment process. In addition, methods used in the treatment, problems encountered, production of different types of orthoses, convenience of application of the orthoses, and degree of patients satisfaction are discussed in this article.
Results:
The mean duration of treatment of the participants until completion of treatment was 25.3 ± 9.7 weeks with a minimum of 9 weeks and a maximum of 41 weeks. No statistically significant correlation was found between the duration of orthotic use in patients with a successful outcome and percentile height and percentile weight. When the duration of treatment using the different types of orthoses was analyzed, significant differences were found between Type 1 and Type 2, and Type 1 and Type 3 orthoses (p < 0.05), while no difference was observed between Type 2 and Type 3 orthoses (p > 0.05).
Conclusion:
We found that bracing is an effective form of treatment for infantile tibia vara up to 38 months of age. We conclude that full-time use of knee–ankle–foot orthoses exerting corrective forces from five points along the full length of the limb was effective.
Clinical relevance:
The localization of the distal tibial correction, the quality of the midtibial correction band, and the importance of the application of corrective forces from five points with rigid methods were found.
Introduction
Infantile tibia vara (ITV) was first reported by Erlacher in 1922, and was identified by Blount in 1937 as a varus deformity associated with the proximal tibia.1–3 Studies on the surgical correction, orthosis application, and spontaneous healing of ITV have been performed since the 1960s.3–11 The studies are mostly radiographic evaluations of ITV, and discuss metaphyseal–diaphyseal (MD) proximal tibial angles and the progression of distal femoral deformity.4,12,13 Body weight and early walking were determined as factors for the development of the disease, which is not seen in nonambulatory participants. Ligamentous laxity and the lateral thrust of the knee in the stance phase of gait have been referenced as determining factors in the studies performed.3,14
In addition to studies suggesting that the tibiofemoral angle in genu varum can spontaneously improve until 3 years of age, a few studies suggest that orthotic treatment is helpful in varus deformities smaller than Langenskiöld Stage II.5,15–18 However, there are many studies on the surgical approach and the results of surgery for cases that have not resolved after 3 years of age.9,16–19 In 1982, Levine and Drennan described the use of the MD angle to distinguish between Blount’s disease and physiologic varus. The MD angle is the angle created by the intersection of a line through the transverse plane of the proximal tibial metaphysis with a line perpendicular to the long axis of the tibial diaphysis. This angle represents the degree of deformity of the proximal end of the tibia and the physiologic bowleg, before the appearance of the radiographic changes of tibia vara. An initial MD angle of more than 11° is indicative of the risk of progression. 20
Orthotic approaches to ITV cases have not been as widely applied as surgical treatments, since the outcome and follow-up of orthotic treatment has not been widely reported, and there is scarce written text on the topic. Only a few types of orthoses have been described until now, and it is unclear which type is more effective. There is insufficient design knowledge on orthotics manufacture and fitting, the treatment periods, and the physical application of the orthosis. The technical difficulty in the application of the corrective forces of the orthosis in small children on short-length lower extremities has not been adequately discussed yet.
The aim of this study is to identify the objective criteria for orthotic treatment, the duration of treatment for different knee–ankle–foot orthoses (KAFOs) in cases with ITV, and the specifications of corrective bands, and to discuss their efficacy. A classic ITV orthosis is a KAFO with a single medial bar. In this study, the orthoses were designed to apply corrective forces from five different points and by various methods.
Material and methods
A total of 22 participants with ITV between the ages of 1.5 and 3 years (minimum 19 months and maximum 38 months) who were referred by an orthopedic surgeon to Ankara University Prosthetics and Orthotics Laboratory to receive orthotic treatment were included in this study in 10 years. Human subject approval from the ethical board committee of Ankara University and informed consent were obtained before any study procedures were initiated.
A radiographic diagnosis of the children prior to orthotic use was performed according to the Langenskiöld criteria, which is used for ITA . According to this classification, most of the participants were Langenskiöld Stage II.
The outcomes for a total of 35 extremities were evaluated, including 13 bilateral and 9 unilateral extremities. None of the deformities were due to traumatic, congenital, metabolic, or infectious causes. Three different types of KAFOs were applied to the participants.
The aim of this study was to evaluate and compare the effects of these KAFOs, which have been produced in the Prosthetics and Orthotics Laboratory of our University for 10 years and are specifically designed for children with ITV. Measurements on the correction of the deformity were taken in order to evaluate the daily application periods; identify difficulties encountered during the production and application of the orthosis, evaluate participant satisfaction; and identify, if any, recurrences in varus deformities.
Single medial metal upright KAFOs with drop lock knee joints were used on all participants. Three types of KAFO were used: Type 1, without a medial discus; Type 2, with a medial discus; and Type 3, a plastic KAFO. Six patients were treated with Type 1, seven participants were treated with Type 2, and seven patients were treated with Type 3 orthoses. Two cases, treated with Type 1 (Case No. 15) and Type 3 (Case No. 22) orthoses were excluded from the statistical evaluation because their treatment was ongoing.
Participants received follow-up clinical examinations and radiological evaluations every 1–3 months. Data on the age, sex, height, weight, and affected extremities were recorded before using the orthoses.
Technical specifications of the KAFO
Correction fields were identified on the positive models produced according to the measurements obtained with plaster cast application. Three corrective forces were planned on the femur for each orthotic type. The forces to be applied on the tibia were again identified on the positive models; however, they were designed in different ways for each of the three types of orthoses (Figure 1). According to this, tibia distal forces were applied from the medial part of the boot in Type 1, from a discus as pressure pad placed on the medial bar in Type 2, and from a boot Type 1, from a discus Type 2, from a plastic ankle-foot-orthosis (AFO) Type 3. Therefore, the application fields of five corrective forces on the femur and proximal tibia were constant, while the fields were planned as on the medial malleolus for Type 1 (Figure 2(a)) and on the upper to medial malleolus on the distal tibia for Type 2 (Figure 2(b)) and Type 3 (Figure 2(c)). The corrective bands applied from the lateral tibia were produced as rigid or elastic columns.
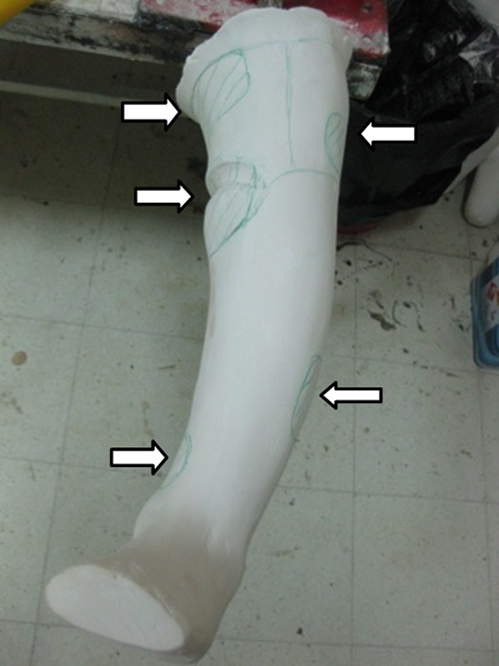
Anterior view of KAFO-positive model showing mediolateral force application.
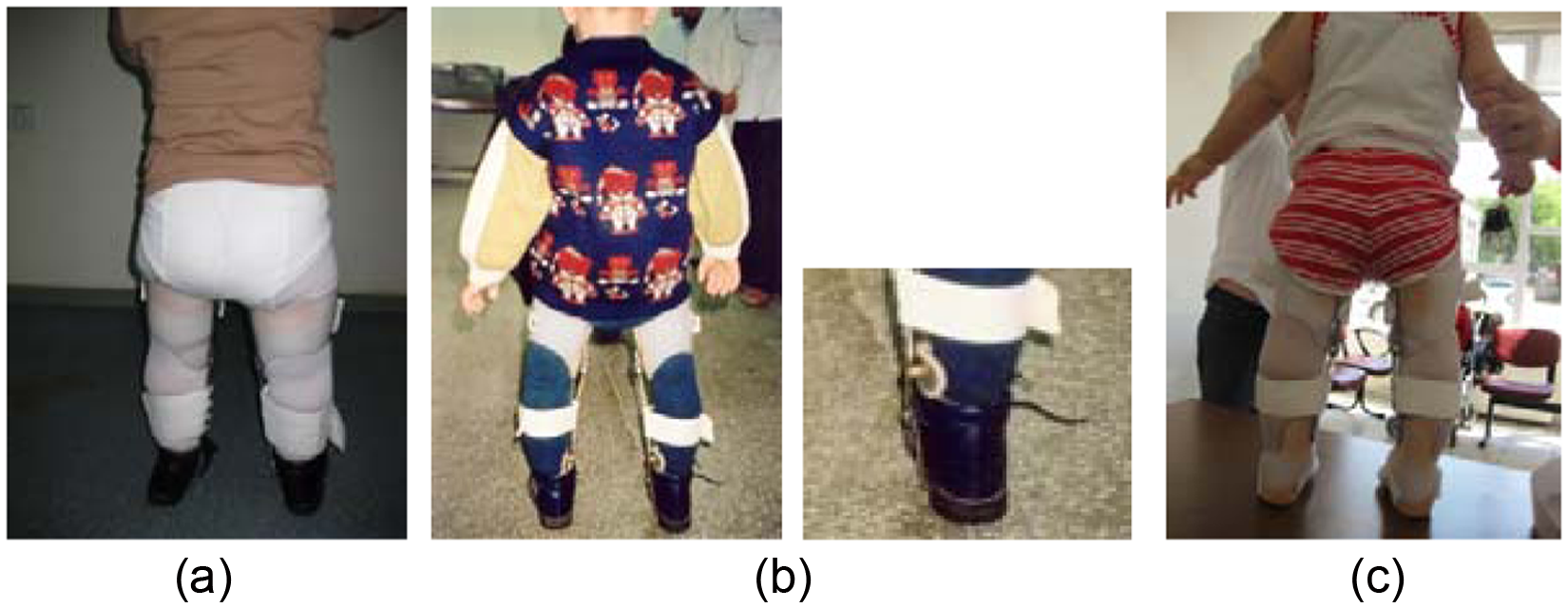
Posterior views of KAFOs with rigid columns: (a) Type 1 KAFO, (b) Type 2 KAFOs and discus-magnified posterior view (Case No. 2), and (c) Type 3 KAFO.
The corrective forces for all three types of orthoses in the plastic thigh sections of the KAFOs were placed according to the patients’ radiographic appearances. The corrective forces on the tibia, however, were located in the femoral plastic thigh section in the region of the medial tibial condyle through the proximal femoral cover, and corrective forces on the tibia were formed with the column and on the medial malleolus in the boot in distal tibia, upper to the medial malleolus at the discus, and plastic AFO region of KAFO (Figure 2).
The discus being is an aluminum plate (3-5 cm in lenght, 2-3 cm in width, and 2 mm in thickness) and the plastazote (3-5 mm in thickness) is covered with the inner surface of discus that is attached to the medial bar of KAFO through a specially designed brass pin (7 mm in diameter and 5–10 mm in length) (Figure 2(b)).
Orthosis use and follow-up
Participants used their orthoses full-time until the first follow-up visit which took place, 1 month after the orthoses application of the orthosis. The orthoses were removed for 3 h every day during the period of use. Stretching exercises directed at the tensor fascia lata, and strengthening exercises for the knee flexor and extensors, and abdominal and back muscles were as well as a classical massage for the lower extremities taught to the families during this process. In cases that showed radiographic improvement (Case Nos. 4, 5, 6, 8, 13, and 21), part-time application (children used the orthoses during the day and at night while sleeping, totally for 12 h) was initiated and subsequently the orthosis was removed.
In cases in which no improvement was observed after the first month, full-time application was continued for a further 3 months (Case Nos. 1, 2, 3, 7, 9, 11, 12, 14, 16, 17, 18, 19, and 20). In cases of no change or a decrease in the angle at the second follow-up visit performed in the fourth month, treatment was replaced with part-time orthotic application (Case Nos. 2, 3, 9, 10, 11, and 19), while full-time application was continued in cases that had increased angles (Case Nos. 1, 7, 14, 16, 17, and 20). The duration of the orthotic application was adjusted according to the patients and the differences in the angles at the monthly and tri-monthly follow-up visits. They were decreased through the transition from full-time to part-time application and then completed. The follow-up visits occuring two years after treatment did not show any tibia vara.
Statistical analyses were performed with the SPSS 16 program. The Pearson’s correlation was used to assess the duration of treatment, age at the start of treatment, percentile height, and percentile weight. The Mann–Whitney U-test was used to compare the different types of orthoses. The p-values of <0.05 were considered to be significant.
Problems encountered
One patient’s steel medial bar was broken during the application of corrective forces. A stirrup was released and broken.
When single-elastic columns were used, deformities and imprints on the soft tissue occurred in the upper and lower edges of the columns. Double-elastic columns were used in three cases with the aim of distributing the forces. These resulted in roll of the soft tissue between the double elastic columns. Redness was not observed under discus and columns, but there were pressure prints.
Twister cables were added to the KAFOs in two cases due to the tension in the internal rotators of the hip (Figure 3). In-toeing was observed in all participants. However, the normal range of in-toeing is very broad due to age, and most of the times, ITV happens with medial tibial torsion.21,22 A twister elastic-fabric cable with the KAFO was used only for internal hip rotation contracture in patients with genu varum.

Anterior view of twister cables added to Type 2 KAFO with rigid columns (left) and posterior view of Type 2 KAFO with an elastic column (right).
In order to prevent the orthosis from directly contacting the skin and forming rashes they wore cotton tights.
Patient satisfaction
Patient satisfaction was evaluated based on the approval of the orthosis by the family, the difficulty of wearing and removing the orthosis, independent walking, duration of application, difficulty in cleaning, and discomfort at the extremities caused by the orthosis. Independent walking in cases where a unilateral KAFO was used was achieved in an average of 1 day. In bilateral cases, independent walking was achieved in an average of 3 days. Walking was accomplished with minimal hand-to-hold support of the family members. No other walking aids were utilized by any of the participants. However, during adaptation of participants to bilateral KAFOs, difference was not observed among types.
Complaints from the child and family were addressed. Soft booties were placed over the boots during sleep in cases with Type 1 and Type 2 orthoses. In some cases, pillows were placed between the patient’s legs to prevent discomfort from the metal bars of the orthosis during sleep. Families reported that the children slept more comfortably when the orthosis locks were unlocked.
Results
A total of 20 patients with ITV completed the treatment. These included 8 males and 12 females. Orthotic treatment was applied to a total of 31 extremities with 9 unilateral and 11 bilateral extremities. All participants included in the treatment were Turkish and of white race. A total of 17 of them had defects in the left extremities, and 14 participants had defects in the right extremities. The mean starting age of the participants receiving treatment was 31.8 ± 4.8 weeks, the mean percentile height was 63.5 ± 29.2 cm, and the mean percentile weight was 81.3 ± 16.05 kg (Table 1). Patients completed the treatment after a mean of 25.3 ± 9.7 weeks with a minimum of 9 weeks and a maximum of 41 weeks. There was no statistically significant correlation between the duration of completion of treatment and percentile height and weight (Table 2).
Characteristics of participants with ITV and orthosis.
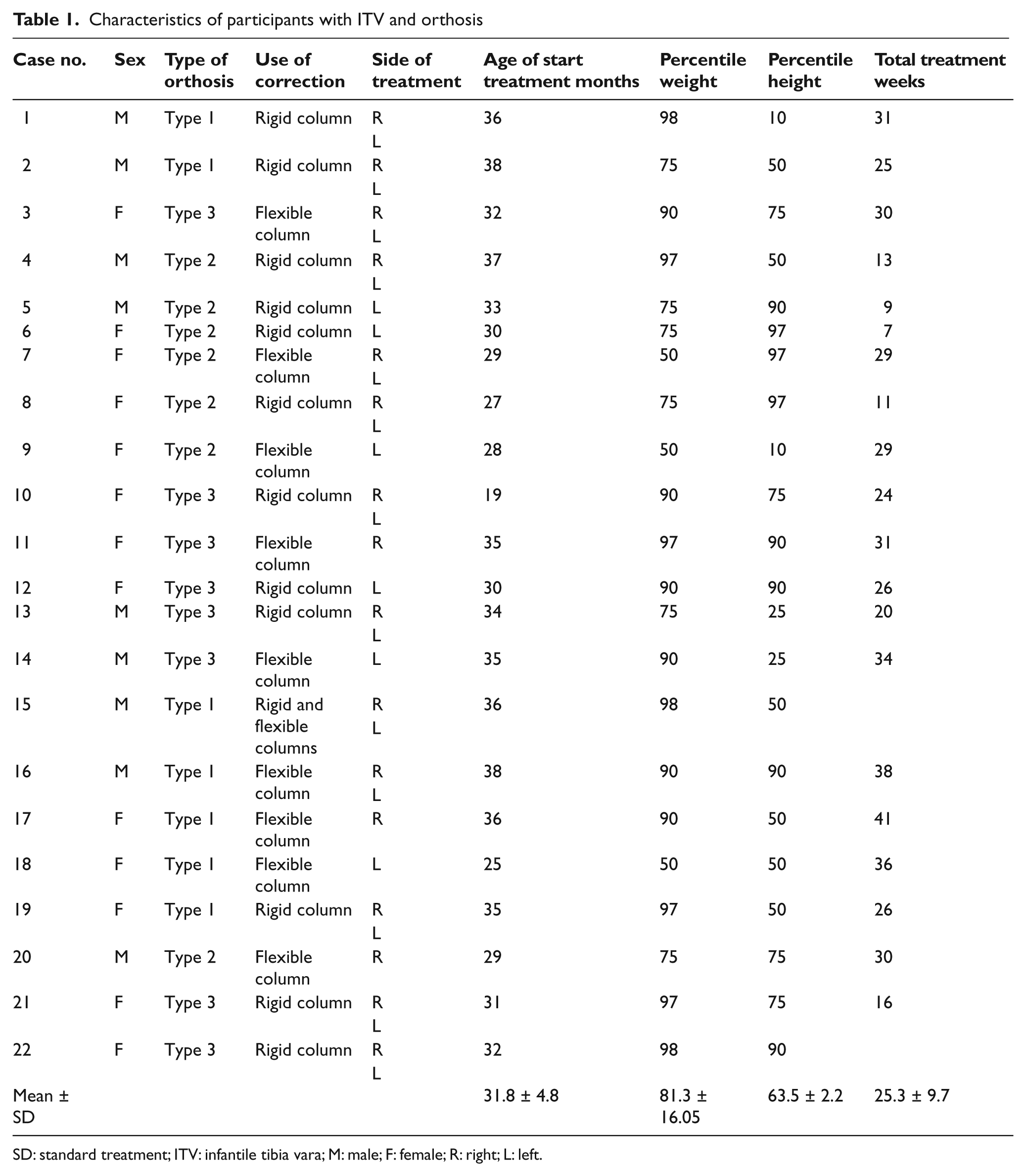
SD: standard treatment; ITV: infantile tibia vara; M: male; F: female; R: right; L: left.
Correlation analysis of the total treatment weeks with the age of start treatment weeks, percentile weight, and percentile height.
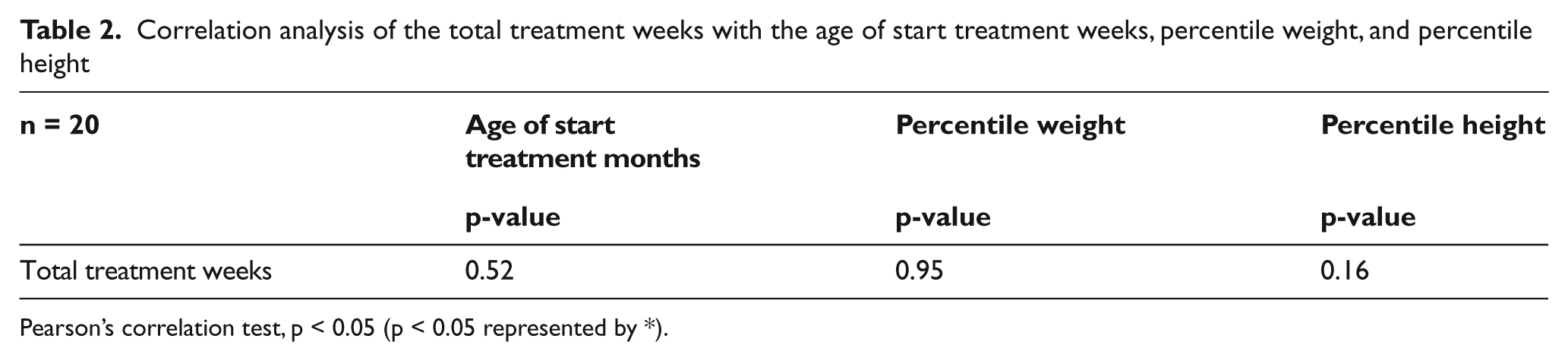
Pearson’s correlation test, p < 0.05 (p < 0.05 represented by *).
When the types of orthoses and the duration of treatment until completion of therapy were analyzed, significant differences were encountered between Type 1 and Type 2, and Type 1 and Type 3 (p < 0.05), while no significant difference was found between Type 2 and Type 3 in duration of treatment (p > 0.05, Table 3). We observed that the metal upright KAFO had the least effect on correction. However, the metal upright KAFO with a medial discus elicited the quickest corrective response.
Comparison according to the types of KAFO.
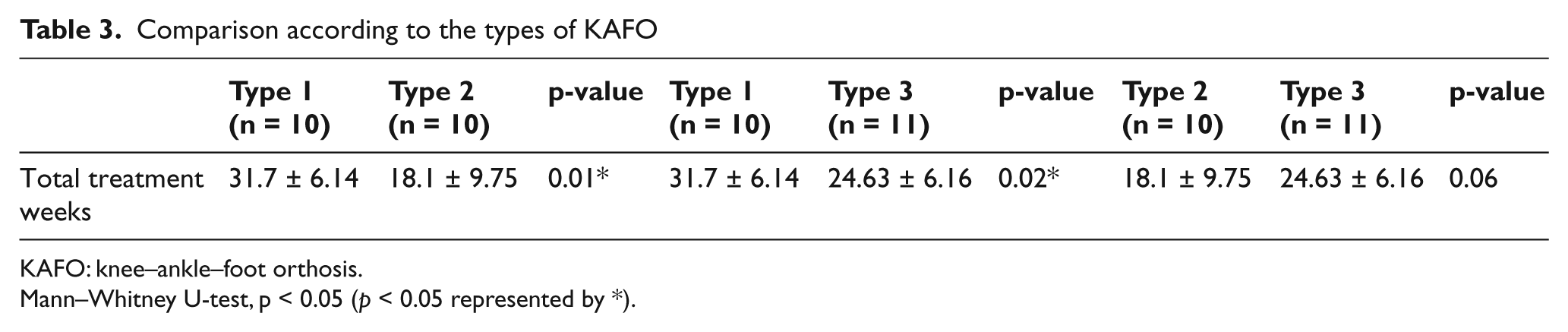
KAFO: knee–ankle–foot orthosis.
Mann–Whitney U-test, p < 0.05 (p < 0.05 represented by *).
When the effects of distal correction methods on the treatment process were evaluated, the medial discus present in Type 2 orthosis, applied from the superior malleolus, was shown to have an important effect on the duration of treatment. A statistically significant difference was observed, with a mean of 18.1 ± 9.75 weeks of treatment in case of the Type 3 orthosis, the obtained result was a mean of 24.63 ± 6.16 weeks of treatment. With this result, the distal tibial corrective effects of the medial discus and the medial part of the compression plastic AFO were found to be more effective in shortening the treatment process compared to the effects produced from the malleolus, which is only from medial to the boot. This shows the importance of correct placement of the corrective effects and the most appropriate localization in the distal tibia. Type 1 orthosis, in which there was medial wall support on the medial malleolus in the boot, showed the longest duration of treatment with a mean of 31.7 ± 6.14 weeks (Table 3).
When rigid and elastic columns in the KAFOs were compared for the duration of treatment, the results were in favor of the rigid column (p < 0.05) (Table 4). Use of a rigid column as a midtibial correction decreased the duration of treatment. When the effects of the different column types used in the different orthoses were evaluated, the differences were significant. The duration of treatment using a Type 1 orthosis with a rigid column was, on average, 3 months less than the same orthosis with an elastic column. The duration of treatment using Type 2 and Type 3 orthoses with a rigid column was 4.5 and 2.5 months less than using the same orthosis with an elastic column, respectively (Table 5). From these findings, we can conclude that use of a rigid or elastic midtibial correction in each orthosis type makes a difference to the duration of treatment and that the rigid column decreases the duration of treatment. In particular, the rigid column used in the Type 2 orthosis was significantly better due to the selection of the medial discus for this type of orthosis and its localization on the tibia.
Comparison according to the types of column.

Mann–Whitney U-test, p < 0.05 (p < 0.05 represented by *).
The effects of different types of column within types of orthoses.
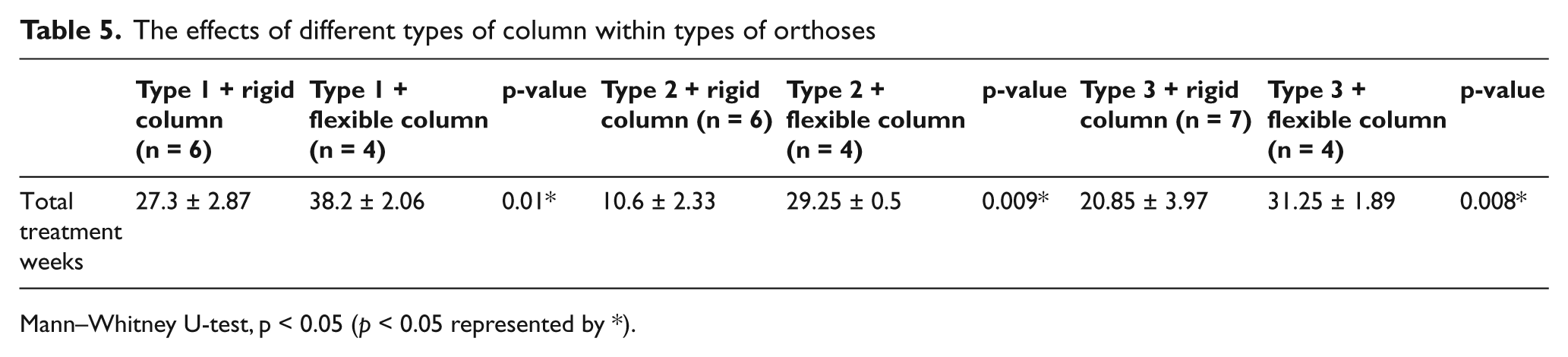
Mann–Whitney U-test, p < 0.05 (p < 0.05 represented by *).
When we looked into the effects of rigid and elastic columns on the duration of treatment, we observed statistically significant differences between Type 1, Type 2, and Type 3 orthoses with a rigid column and Type 2 orthosis with rigid column, and Type 3 orthosis with rigid column (p < 0.05; Table 6). According to this, upright metal KAFOs required the longest time to achieve a corrective effect among the groups using a rigid column; and these KAFOs with a medial discus were effective in the shortest time. These results shows that the rigid column as a midtibial correction type and the medial discus as a distal correction type have important effects on the duration of treatment (Figures 4 to 6).
The effects of identical column with different types of orthoses.
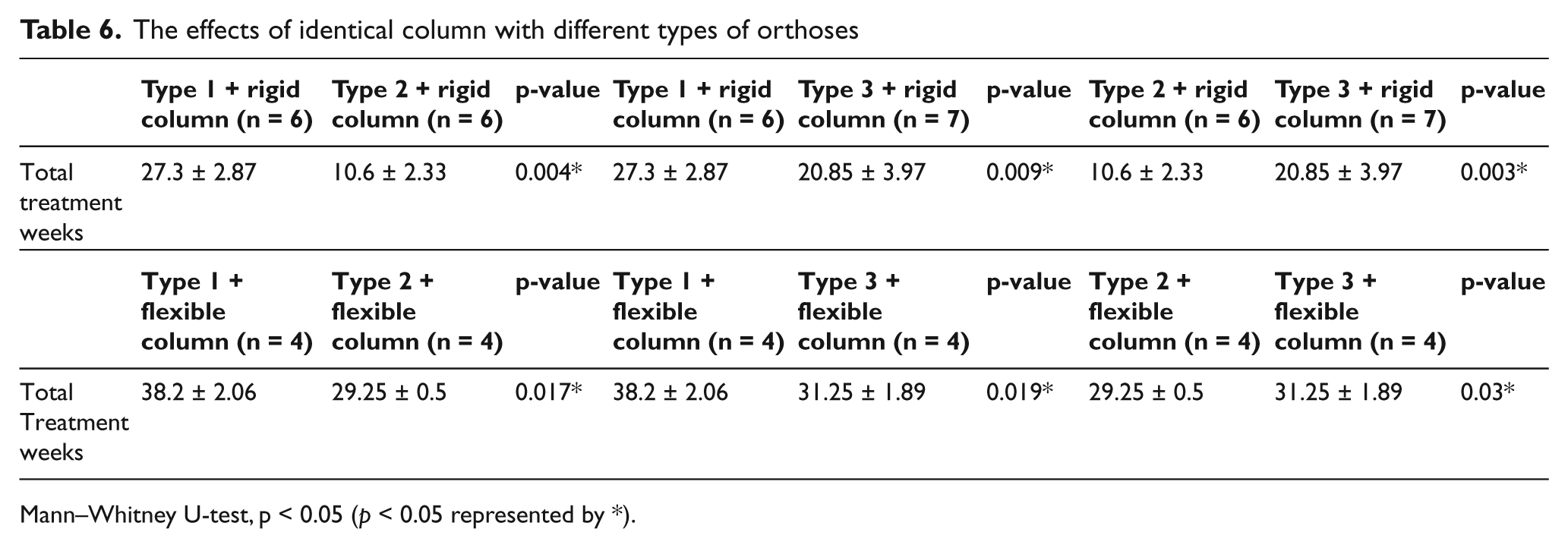
Mann–Whitney U-test, p < 0.05 (p < 0.05 represented by *).

Anteroposterior radiographs of lower extremities before (left) and after (right) treatment with Type 2 KAFO (Case No. 7).
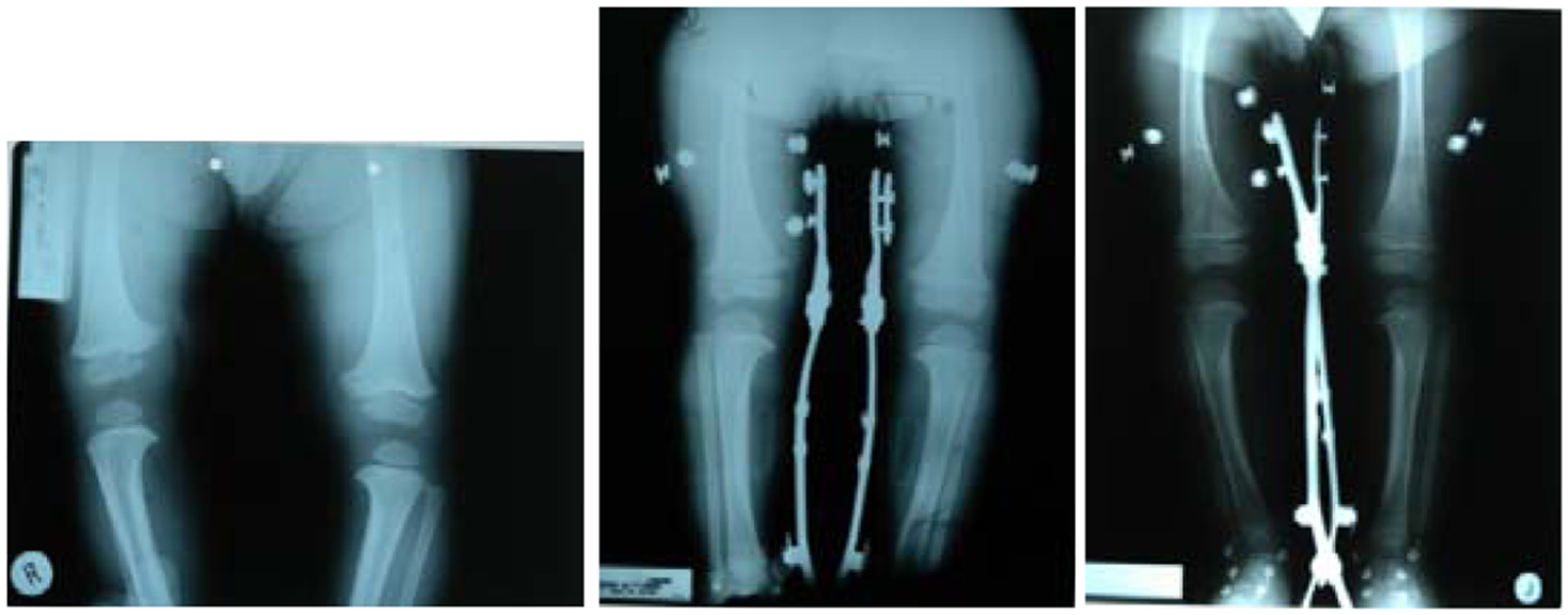
Anteroposterior radiographs of lower extremity at initial stage of bracing (left), at the duration of treatment (middle), and at latest fallow-up (right) with Type 2 KAFO applications (Case No. 2).

Posterior view of Type 2 KAFO application with rigid columns (left) before treatment (middle) and after treatment (right) (Case No. 8).
Significant differences in the duration of treatment were found between groups using the elastic column in Type 1, Type 2, and Type 3 orthoses. The elastic column, particularly in a Type 2 orthosis, was found to have a shorter response time (Table 6). Although that the duration of treatment was lengthened by 3 months when using an elastic column, the longest treatment was still observed in participants using a Type 1 KAFO, and the shortest treatment was observed in participants using a Type 2 KAFO. In terms of ease of wear and removal, usage, comfort, and cleanliness, Type 3 KAFOs showed the highest patient satisfaction.
Discussion
The natural history of ITV deformity in children is uncertain. Most children with so-called physiological bowing will have spontaneous resolution and will not necessarily require treatment. A small number, however, remain in varus and have slow progression of the deformity, which is determined as pathologic genu varum. Unfortunately, there are few reports of ITV since surgery or orthotic treatment is generally advised. The aim of this study was to determine different orthotic treatments and their effects on this condition.
Many authors believe that treatment by orthosis is effective in the early stages of ITA.17,23–27 This study showed successful orthotic treatment in ITV. Richards et al. 24 reported improvement after orthotic treatment in 65% of patients with Langenskiöld Stage II ITV, and the duration of orthosis use averaged 9.7 months. The prescribed orthosis was a KAFO “elastic Blount brace” producing a valgus force by a 3-point pressure system with T-band connection boats. This brace was first introduced in 1985 by Supan and Mazur 23 as an alternative to the conventional KAFO. The designed consisted of three forces not on the full length of the limb. We modified the design to exert five forces on the full length of the limb. In this study, the duration of orthosis averaged 6.2 months.
Raney et al. 26 and Zionts and Shean 25 advised orthotic treatment for cases of ITV with an MD angle of >16°. The success rates of these two groups were 86% and 92%, respectively. Zionts and Shean 25 applied three forces on the orthosis they used, and the corrective force was located laterally on the knee. Zionts concluded that daytime, ambulatory orthotic treatment may favorably alter the natural history of tibia vara in patients younger than 3 years of age and with a Langenskiöld Stage I or II deformity. Raney et al. applied three forces on the orthosis they used in their study, which were applied by means of a wide strap located on the lateral tibia instead of the lateral knee. In this study, forces were applied from five points on the orthosis we designed, and orthotic correction was observed in all patients. Complete improvement was observed in 20 of 22 participants. The treatment on the remaining two patients has not yet been completed, although a reduction in their MD angles was observed. None of the patients needed surgical intervention. Based on our experience, Stage II and Stage III tibia vara can be effectively corrected with orthotic management. Orthotic treatment gave the best result in participants with Langenskiöld Stage II.
Blount advised his bowleg brace to be used at night in patients younger than 2 years. 28 Schoenecker et al. 17 reported successful outcome in five of six extremities in patients with Stages I–II ITV. Loder and Johnston 16 reported successful outcomes in 12 of 23 extremities in patients with Stages I–II disease, and orthotic treatment was only 50% successful. They believe that orthoses were indicated only for children between ages 1.5 and 2.5 years; however, this study showed successful treatment from 1.5 to over 3 years of age. Full-time use of the orthosis at the beginning of treatment was important in this study. The type of corrective strap was also important. A rigid lateral midtibial strap was more effective than an elastic strap. We found that our second orthotic design and its corrective results were admirable. Kumar et al. 27 showed 18 patients with Stage I and Stage II ITV. They were treated with night-time bracing.
We conclude that all three types of KAFOs and their effects on 31 extremities in 20 participants with ITV have been successful. The fastest correction was observed implementing the second design. We also found that bracing is an effective form of treatment for ITV up to 38 months of age if the KAFO exerts five forces on the full length of the limb with full-time use.
This research is being continued and when results of two participants currently under treatment are obtained, tables and graphs showing the changes in MD will be presented as a separate research that would be able to assist clinical practice.
Footnotes
Conflict of interest
The authors report no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.