
Abstract
Introduction
Sarcopenia, a loss of muscle mass and strength with aging, is associated with various TKA-related complications. In 2020, the AWGS published an undated guideline (AWGS 2019) based on studies from East and Southeast Asia. The purpose of this study was to determine the prevalence of sarcopenia in Asian female patients awaiting primary total knee arthroplasty due to advanced knee osteoarthritis using the updated AWGS criteria.
Materials and Methods
The present study included 138 female patients who scheduled for primary TKA with severe osteoarthritis. The included patients were assessed with use of an AWGS 2019 diagnostic criteria based on muscle strength, physical performance, and appendicular skeletal muscle mass. Clinical parameters related to sarcopenia were collected and knee status assessed using the Knee Society scoring system. To better define the association with age, patients were stratified into following four groups: <60, 60–69, 70–79, ≥80. The prevalence of sarcopenia was identified, and the association between sarcopenia and clinical variables was analyzed.
Results
The prevalence of sarcopenia and severe sarcopenia in this cohort according to the updated AWGS criteria was 35.5% and 21.7%. Prevalence of sarcopenia and severe sarcopenia significantly increased with advancing age (p = .003, p = .040, respectively). Although not statistically significant, the proportion of severe sarcopenia among sarcopenia also increased with age. Multivariate logistic regression analysis revealed that lower BMI and lower 25-OH-vitamin D3 level were independent risk factors associated with sarcopenia in women awaiting TKA.
Conclusions
In conclusion, our study confirmed that sarcopenia is more prominent amongst female patients awaiting primary TKA than the general population. Therefore, orthopedic surgeons should consider sarcopenia prevention and intervention in this group. Further studies are needed to investigate the effect of TKA on sarcopenia, and the difference of TKA outcomes between groups with or without underlying sarcopenia.
Introduction
Total knee arthroplasty (TKA) is one of the most widely used surgical methods in the orthopedic field, and the demand is steadily increasing due to population aging.1–3 However, as the amount of surgery volume gradually increases, TKA related complications also increase, which is a major challenge for orthopedic surgeons. Several studies have reported that sarcopenia, a highly discussed phenomenon in the medical community, can independently predict postoperative complications.4–13 Since sarcopenia is known to be an independent risk factor for falls, lower extremity fracture and periprosthetic joint infection, it should be emphasized more in patients undergoing TKA.4,14–18
The diagnostic criteria of sarcopenia have been proposed by several groups. Among them, the diagnostic criteria proposed by the Asian Working Group for Sarcopenia (AWGS) in 2014 was based on Asian data that reflects differences in the anthropology, culture, and lifestyle of Asians compared to Western populations. 19 This was because special consideration was required for Asians' relatively smaller body sizes, higher adiposity, and active lifestyle due to delayed industrialization. In 2020, the AWGS published an updated guideline (AWGS 2019) based on studies from East and Southeast Asia. 20 Updated AWGS criteria evaluate low muscle mass, low muscle strength, and low physical performance to diagnose sarcopenia.
Sarcopenia, a loss of muscle mass and strength with aging, is associated with various TKA-related complications.4,14–18 Elderly women make up about 70–90% of TKA candidates,21,22 and the number is gradually increasing due to population aging.1–3 However, a few research has been conducted on the prevalence and risk factors of sarcopenia in these patients.
The purpose of this study was to determine the prevalence of sarcopenia in Asian population awaiting primary TKA due to advanced knee osteoarthritis using the updated AWGS criteria. The study also examined the relationship between sarcopenia and other clinical parameters. This study finds that sarcopenia is prevalent amongst TKA candidates; therefore, orthopedic surgeons should understand sarcopenia to be a risk factor and educate potential TKA candidates of its effect on TKA.
Materials and methods
Study sample
The study samples were retrospectively collected from consecutive patients scheduled for primary TKA due to osteoarthritis at a single secondary hospital in Korea from January 2017 and August 2018. We included independently walking female patients who were diagnosed with primary osteoarthritis. Osteoarthritis was diagnosed by physical and radiological examination, and Kellgren/Lawrence grades ≥3 were used as the inclusion criteria. The exclusion criteria were male, any diagnosis other than primary osteoarthritis, non-independent ambulation due to comorbid medical conditions, and patients with metal implants in appendicular body regions, which potentially could affect the accuracy of calculating appendicular skeletal muscle mass (ASM). 23 A total of 170 patients participated in the study. The final analysis included 138 participants after excluding 20 male patients, nine patients diagnosed with non-primary osteoarthritis and three patients with metal implants in appendicular body regions identified on DXA (dual‐energy X‐ray absorptiometry) images.
All investigations were approved by the Institutional Review Board of our institution and the procedures used in this study adhered to the tenets of the Declaration of Helsinki. Written consent was not required due to the retrospective nature of this study.
Diagnosis of sarcopenia
Muscle strength measurement
Muscle strength was evaluated by the handgrip strength test. The dominant handgrip strength was measured with a handgrip dynamometer (Jamar, Bolingbrook, IL, USA) by applying the Southampton protocol (sitting with 90° elbow flexion as the standard position). 24 The participants, with verbal encouragement, squeezed the dynamometer with the utmost effort possible. Participants were given three trials with 30 second resting intervals. The maximum handgrip strength was expressed in kilograms by selecting the highest measurement of the three trials. Low muscle strength was defined as a hand strength of less than 18 kg for women. 20
Physical performance measurement
Physical performance was evaluated by 4-m walking speed. The patient was asked to walk down a hallway through a 2-m acceleration zone, a central 4-m testing zone, and a 2-m deceleration zone. A stopwatch was used to record the gait speed. The gait speed was measured twice in order to find the average speed. Patients who took longer than 4 s to walk 4 m (<1.0 m/s) suggested low physical performance. 20 To reduce knee pain that may affect physical performance, all patients were given 200 mg of Celecoxib and an additional 500 mg of acetaminophen as needed.
Measurement of appendicular skeletal muscle mass
Appendicular skeletal muscle mass (ASM) was measured using a whole-body DXA scanner in accordance with the manufacturer’s protocol (Lunar Prodigy Advance, GE Healthcare, Madison, WI, USA). ASM was defined as the sum of the lean mass of both the upper and lower extremities and was assumed to be almost equal to the skeletal muscle mass. As height increases, the muscle mass of the limbs will increase. Therefore, we obtained the skeletal muscle index (SMI) by correcting the muscle mass with height (ASM (kg)/height (m2)). The cutoff values for the ASM index for low muscle mass were <5.4 kg/m2 in women, respectively. 20
Definition of sarcopenia
The updated AWGS criteria defined sarcopenia as low muscle mass and low muscle strength or low physical performance, and severe sarcopenia as low muscle mass, low muscle strength, and low physical performance.
Assessment of clinical parameter
The following clinical parameters were collected based on the literature: age, body weight, height, body mass index (BMI), and the Charlson comorbidity index. The commercial kit, Architect 25-OH Vitamin D3 Reagent kit (Abbott Diagnostics, Lake Forest, IL, USA) was used to measure serum concentration of 25-OH vitamin D3. Knee status was assessed using the Knee Society (KS) scoring system (including knee score and function score), which was designed to provide a simple and objective scoring system to rate the knee and patient’s functional abilities in TKA. All assessments were performed the day before surgery.
The prevalence of sarcopenia in female patients with severe osteoarthritis awaiting primary TKA was determined. The prevalence of sarcopenia in this cohort was compared to that reported by the Korean Frailty and Aging Cohort Study for community-dwelling adults aged 70 years and older. 25 That study also used the updated AWGS diagnostic criteria to conduct an evaluation. The association of sarcopenia with the clinical parameters was investigated.
Statistical analyses
All variables are presented as the mean ± standard deviation or number (percentage). To better define the association with age, patients were stratified into following four groups: <60, 60–69, 70–79, ≥80. Statistical comparisons of the continuous variables were performed using Student’s t-test, the Mann-Whitney U test or Jonckheere-Terpstra trend test, whereas the categorical variables were analyzed using the χ2 test, Fisher’s exact test, or a linear by linear association, as appropriate. Multiple logistic regression analysis was performed to evaluate the independent risk factors of sarcopenia. p-values of less than .05 were considered statistically significant in all analyses. The statistical analyses were conducted using Microsoft Excel 2013 (Microsoft, Redmond, WA, USA) and SPSS software (version 20 SPSS, Chicago, IL, USA).
Results
Characteristics of patients from the total sample and according to age group.

P-value in bold are statistically significant (p < 0.05).
Data are presented by mean ± standard deviation or number (%).
Abbreviations: BMI (Body mass, index); K-L (Kellgren Lawrence); KS (knee society); ASM (appendicular skeletal muscle mass); DEXA (dual-energy X-ray absorptiometry).
aJockheere-Terpstra test for continouous variables and linear-by-linear association for categorical variables.
Prevalence rates of sarcopenia and severe sarcopenia from the total sample and according to age group.
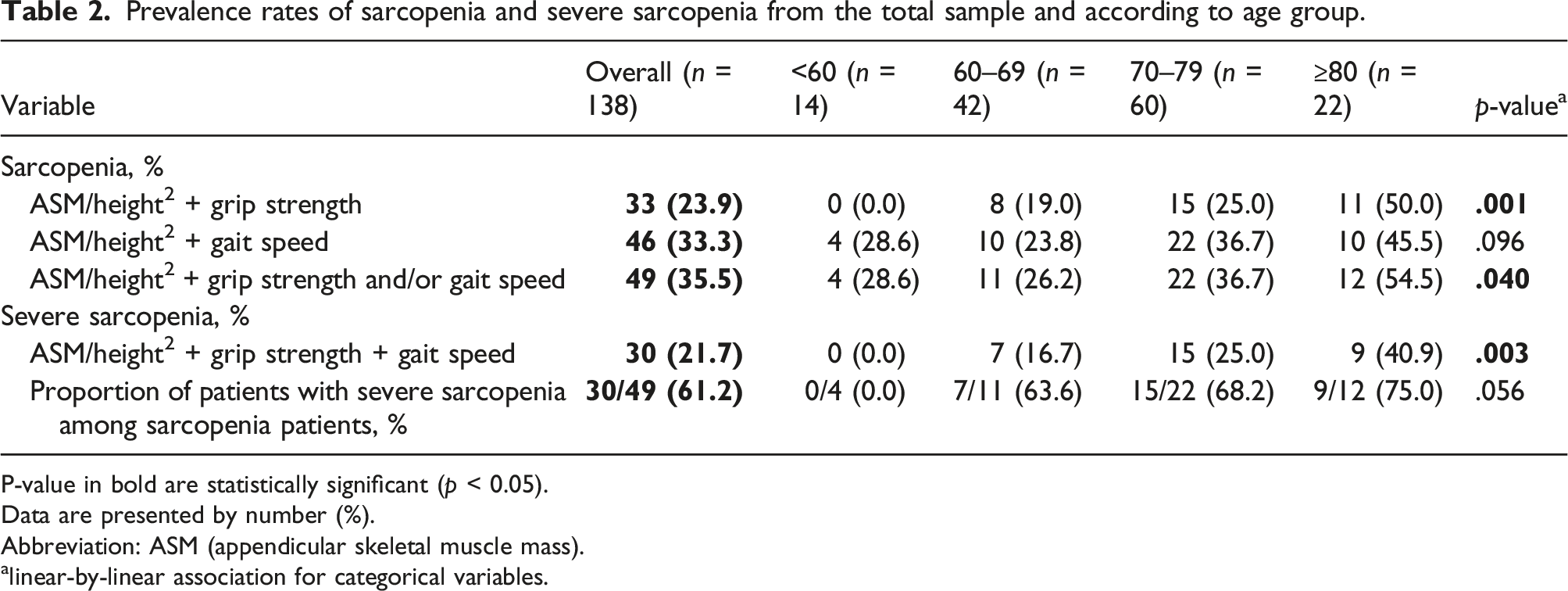
P-value in bold are statistically significant (p < 0.05).
Data are presented by number (%).
Abbreviation: ASM (appendicular skeletal muscle mass).
alinear-by-linear association for categorical variables.
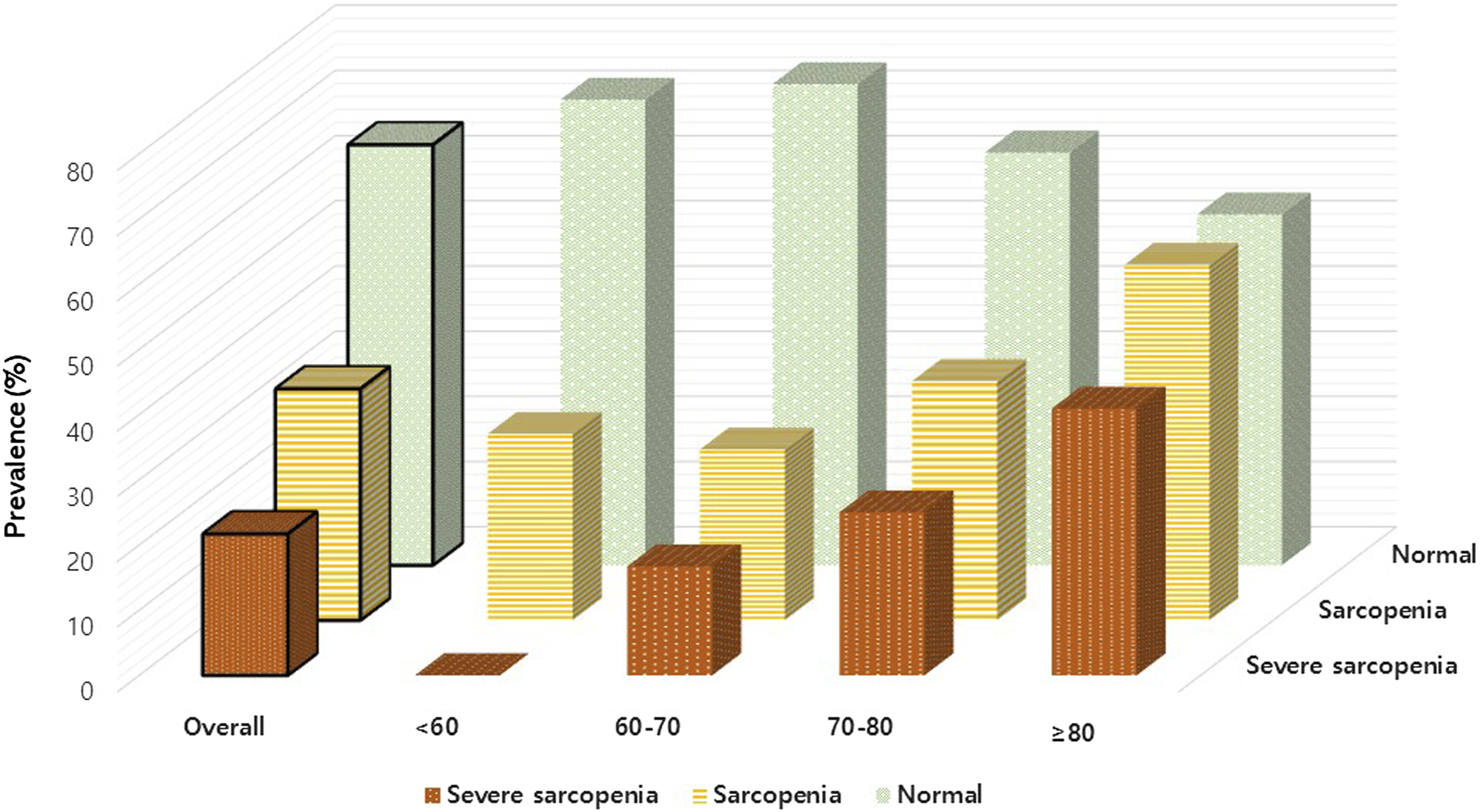
Distribution of sarcopenia and severe sarcopenia for overall sample and different age groups.
Compared to the general Korean elderly female population, 25 the prevalence of sarcopenia and severe sarcopenia in severe knee osteoarthritis female patients were significantly higher (35.5% vs. 18.8%, p < .001 and 21.7% vs. 3.2%, p < .001 respectively).
Characteristics of patients from the total sample and according to the presence or absence of sarcopenia.

P-value in bold are statistically significant (p < 0.05).
Data are presented by mean ± standard deviation or number (%).
Abbreviations: BMI (body mass, index); K-L (Kellgren Lawrence); KS (knee society); ASM (appendicular skeletal muscle mass); DEXA (dual-energy X-ray absorptiometry).
ap-values are based on the chi-square, Fisher exact, or independent t-test.
Multivariate logistic regression analysis of variables associated with sarcopenia.

P-value in bold are statistically significant (p < 0.05).
Abbreviations: OR (odds ratio calculated with logistic regression); BMI (body mass, index); K-L (Kellgren Lawrence); KS (knee society).
Discussion
Aging causes undesirable changes in body composition, such as the loss of skeletal muscle, which is sarcopenia. 26 Sarcopenia is defined as skeletal muscle disorders involving an accelerated loss of muscle mass, strength, and function associated with age. 27 In elderly people, this condition is associated with various chronic diseases and a decrease in the quality of life, as well as an increased risk of physical limitations. 28
The prevalence of sarcopenia in Asia is reported to be 0.1% to 23.6% in community‐dwelling older women, 29 and elderly female OA patients make up about 70–90% of TKA candidates. 30 Although the number of older women with TKA is increasing due to an aging population, little is known about the prevalence and risk factors of sarcopenia in this group. More information on sarcopenia in this group may help surgeons select and educate patients more appropriately. To the best of our knowledge, this is the first study to apply the recently updated AWGS criteria to female patients awaiting TKA due to primary knee osteoarthritis.
Using three diagnostic assessments including low appendicular skeletal muscle mass and low muscle strength (grip strength) or low physical performance (gait speed), this study cohort yielded a 35.5% prevalence of sarcopenia according to the updated AWGS criteria. The prevalence in this severe osteoarthritis cohort was significantly higher compared to the general Korean female population (35.5% vs. 18.8%, p < .001). The prevalence of sarcopenia and severe sarcopenia increased statistically significantly with advanced cohort age. Although not statistically significant, the proportion of severe sarcopenic patients increased among total sarcopenic patients with advanced cohort age.
Previous studies showed that age, low exercise rate, and inflammatory reactions accounted for the progression of osteoarthritis associated with sarcopenia.31,32 Severe pain and poor physical function due to advanced osteoarthritis of the knee joint might limit patient activities, which may increase the risk of developing sarcopenia. Our research results supported this by revealing that the prevalence of sarcopenia in female patients prior to TKA was significantly higher than that in the general population. In addition, more than half of the sarcopenia cases diagnosed in our cohort were severe sarcopenia. These results suggest that more attention to sarcopenia is needed in this population.
In the present study, the presence of sarcopenia was associated with some baseline characteristics, such as age, lower weight, and lower BMI and lower 25-OH-vitamin D3 levels. Among them, lower BMI and 25-OH-vitamin D3 levels remained associated in the multivariate analysis.
Low BMI was a risk factor for sarcopenia in female patients with severe knee osteoarthritis, as in previous studies in the general population.33,34 SMI is positively correlated with BMI, and low SMI is uncommon when BMI is greater than 25. 35 The strong relationship between BMI and sarcopenia deserves further consideration.
Vitamin D deficiency is common in both geriatric patients (30–90%) and community-dwelling older persons (2–60%).36,37 Correlation between low vitamin D concentration and poor muscle function has been suggested in some studies38–42 while there are still some contrary findings.43,44 Our study also found that low 25-OH-vitamin D3 is an independent risk factor for sarcopenia. Decreased Vit D3 synthesis among the elderly patient’s skin compounded with reduced UV exposure due to arthritic sedentariness may explain this relationship.
Our results suggest that female patients with advanced knee osteoarthritis may be more likely to develop sarcopenia with aging. According to the Lancet’s latest review on sarcopenia, physical activity is considered as the primary treatment for sarcopenia, because there are currently no specific drugs approved for sarcopenia. 27 Through arthritic pain relief, TKA helps sarcopenic patients engage in therapeutic physical activity. In this respect, physicians need to pay attention to sarcopenic status in patients with osteoarthritis and provide appropriate intervention. It is also recommended that the preoperative assessments of TKA include screening assessments for sarcopenia. The AWGS recommends case-finding to identify the early signs of sarcopenia, screening by measuring calf circumference, administering the SARC-F questionnaire (a simplified screening tool for assessing sarcopenia in older adults), and the SARC-F administration combined with calf circumference (SARC-CalF). 20
In previous studies amongst patients with knee osteoarthritis, physical performance was inadequately tested due to the severe pain or mobility limitations. The strength of this study was that all diagnostic assessments were well-performed. However, this study had some limitations. First, its retrospective design could lead to selection bias. Although subjects were continuously enrolled, the number of patients in each age group were not equal. Second, these results are not representative of all patients. The cohort of this study consisted of patients with severe knee osteoarthritis who were scheduled for TKA due to their intractable pain, but not all knee osteoarthritis patients are willing or eligible to receive TKA. Nevertheless, considering the assessment and management of sarcopenia before and after TKA in severe knee osteoarthritis patients, the results of this study would provide meaningful information. Third, we used the 4-m test to evaluate physical performance, whereas the AWGS standard uses the 6-m test. However, several studies have used 4-m to assess physical performance,45–47 which would not significantly affect our study results. Fourth, there was no data collection on physical activity or nutritional status that could be related to the differences in muscle mass. In addition, not all information was collected on the therapeutic interventions that could affect physical performance. Furthermore, some patients may have had hand OA, which could affect grip strength.
Conclusion
In conclusion, our study confirmed that sarcopenia is more prominent amongst female patients awaiting primary TKA than the general population. Therefore, orthopedic surgeons should consider sarcopenia prevention and intervention in this group. Further studies are needed to investigate the effect of TKA on sarcopenia, and the difference of TKA outcomes between groups with or without underlying sarcopenia.
Footnotes
Authors’ contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Dojoon Park, Chan Jin Park, Min-gee Jung, Youn Ho Choi, Kwang-Sun Park, Hae Seok Koh. The first draft of the manuscript was written by Dojoon Park and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
All investigations were approved by the Institutional Review Board of our institution and the procedures used in this study adhere to the tenets of the Declaration of Helsinki.
Data availability statement
The datasets used and/or analyzed in this study are available from the corresponding author upon reasonable request.