
Abstract
Background
Posterior stabilized (PS) total knee arthroplasty (TKA) is advocated in severe varus osteoarthritic (OA) knees as the posterior cruciate ligament posed challenges in gap balancing. However, there is scarcity in the literature to illustrate the superiority of PS TKA over cruciate retaining (CR) TKA. Our study aims to compare the outcomes between CR and PS TKAs in patients with severe varus OA knees.
Introduction
Since the advent of total condylar protheses designed by Insall et al. in 1976, 1 Cruciate Retaining (CR) and Posterior Stabilized (PS) designs are the two main types of unconstrained total knee protheses in simultaneous development in the market. The superiority of CR versus PS design in total knee arthroplasty (TKA) has been debated since 1990s 2 and is still largely inconclusive.3–5 The advocates for CR TKAs proposed that retained PCL confers theoretical benefits of native femoral rollback, increased proprioception, 6 preservation of native joint line and bone stock, 7 and lesser risk of mid-flexion laxity. 8 On the other hand, the proponents for PS TKAs have argued that PS designs achieve better range of motion (ROM) with the femoral cam—tibial post articulation5,9 and that they are less technically demanding to achieve gap balancing with the sacrifice of PCL. One of the other advantages includes the better conformity between the articulating surfaces rendering better knee stability with reduced slam-down and edge-loading of the polyethylene. 7
As the PCL serves as a secondary medial knee stabilizer, it can pose potential challenges in medial releases and creation of equal resection gaps during TKA.10,11 Hence, it was extrapolated that soft tissues balancing while retaining the PCL in CR TKAs can be technically more challenging in the face of significant coronal plane deformities such as severe varus knees in which there are tight medial and lax lateral structures. However, in the literature, there is a conflicting body of evidence in supporting the use of CR TKAs in knees with significant coronal deformities. Laskin has advocated use of PS TKAs for knees with severe varus deformities12,13 as he reported that, in a series of 65 patients, there were higher incidences of pain, bone cement radiolucencies, and reduced ROM in CR TKAs for severe varus knees at 10 years’ follow-up. 14 Lombardi and Berend has also proposed the removal of PCL in TKA for patients with significant varus or valgus malalignment. 15
On contrary, several authors proposed that CR designs delivered favorable results in severe varus osteoarthritis knees.16–18 Ritter et al. evaluated on the functional outcomes and reported good results with CR in severe varus knee of ≥20°. 16 Kubiak et al. compared 10-year results of CR TKAs in patients with pre-operative coronal plane deformity of at least 15° to the historical results of PS TKA designs in similar patients and had found very good results with 93% revision-free survivorship at 10 years and no revision for instability or loosening. 17 Faris et al. reported that a PCL retaining prosthesis could be used as long as proper soft tissue balancing was performed at the time of the surgery. 18
Aims and hypothesis
The hypothesis of our study is that CR designs for TKA can achieve favorable outcome in Asian osteoarthritic knees with severe varus deformities and are comparable with the PS designs. In this paper, we compared the outcomes of Asian patients with severe varus knees who underwent CR TKAs, with patients who received PS TKAs for similar deformities.
Materials and methods
This is a retrospective review conducted on a prospectively collected data from patients who underwent primary TKA from 2003 to 2013 for osteoarthritis knee in a hospital registry. All the data were collected at a centralized diagnostic center and managed by an institutional joint registry with the requisite data protection and integrity protocols.
The patients who had pre-operative severe varus deformity knees (≥15°) were sorted into two different groups based on the TKA implant type (Group CR and PS) and matched according to age, gender, and body mass index (BMI). The rationale for the choice of matched pair design in our observational study was to minimize selection bias and to create a homogenous population in terms of patients’ demographics.
The individual pre- and post-operative radiograph of the knees were reviewed to record the anatomical knee alignment. The anatomical alignment was recorded as the tibiofemoral angle which is the angle formed at the knee joint by the intersection of the longitudinal axes of the femoral and tibial shafts on antero-posterior view of standing X-ray film of knee. 19 Coronal angular deformity of ≥15° is widely accepted as a cut-off figure for defining severe genu deformity,12,15,17,20 whereas neutral mechanical alignment is defined as having a valgus anatomical alignment of 5°–7°. 21
The inclusion criteria were osteoarthritis knees with severe varus deformity of anatomical alignment ≥15° which received primary TKA with unconstrained and fixed bearing implants (either CR or PS). The cut-off of 15° varus deformity was decided as studies in the literature have reported significant implications on the outcomes of TKA from 15° varus deformity onward.12,15,17,20 A minimum of 2 years follow-up was required to be included in the study.
The exclusion criteria were patients with history of inflammatory arthritis, prior surgical interventions to the knee such as high tibial osteotomy, arthroscopic procedures, previous unicondylar knee arthroplasty, and previous fractures adjacent to knee. Knees with concomitant severe fixed flexion deformity of ≥15° were omitted in order to eliminate the confounding effect of sagittal deformities on the outcomes. This is because knees with severe sagittal deformities entail different surgical concerns such as the need for posterior release and gap balancing as opposed to knees with severe varus deformities which warrant other technical considerations such as the need for medial releases and management of proximal tibial bone defects. Cases complicated with superficial or deep-sited infections were also excluded to eliminate a spurious confounding effect of infection on outcomes.
The patients’ demographic data recorded were as follows: age at time of surgery, gender, and BMI. The intra-operative details collected from the electronic records were implant design, use of polyethylene insert size, whether the patella was resurfaced and whether a navigation system was used. The electronic records of the patients were evaluated for post-operative events of aseptic loosening requiring revision arthroplasty.
Surgical procedures
All the patients underwent fixed bearing unconstrained TKA (CR or PS) after induction of anesthesia. All surgeries were performed by senior surgeons in the institution and the choice of surgical techniques and implants were dependent on individual surgeon’s personal preference and experience. The TKA implant systems used in this study comprised of P.F.C® Sigma® Total Knee System (DePuy Orthopaedics Inc, Warsaw, IN) (n = 63) and NexGen® Complete Knee Solution (Biomet Inc, Warsaw, IN, USA) (n = 49). The use of computed assisted navigated TKA was performed for five knees. Patellar arthroplasty and use of all-polyethylene tibial components were performed for a total of 3 and 11 knees, respectively. Most of the knees were operated via the medial parapatellar approach except for one knee which was performed via a mid-vastus approach. The variants in surgical techniques were dependent on individual surgeons’ preferences. Literature has shown there is no significant differences in terms of functional outcome despite the differences in surgical techniques as listed above.22–25
The correction of the coronal deformities was accomplished via medial exposure, osteophyte removal, and soft tissue releases at the discretion of the surgeon. The soft tissue releases were executed sequentially from deep medial collateral ligament (MCL), superficial MCL, and to posteromedial capsule, as necessary, to achieve adequate medial release and a stable knee. For CR knees, the posterior cruciate ligament was preserved and might be recessed, as necessary, to achieve proper gap balancing. With proximal tibial bone loss being a potential problem in knees with severe varus deformity, the decision on whether to use implant augmentations such as cement, screw, or tibial stems was dependent on surgeons’ assessment and preference. All surgeries achieved correction of the varus deformity, proper gap balancing, and stable knee with the trial components before the actual implants were used.
The post-operative management consisted of the use of continued prophylactic antibiotics for 24 h and an analgesic regime including parenteral opioids. All patients received mechanical prophylaxis against deep venous thrombosis with the use of intermittent pneumatic calf pumps. The decision for post-operative use of continuous passive motion for the knees would be dependent on individual surgeons’ clinical assessment and preferences. Regardless of CR or PS implants, all the patients underwent a standardized rehabilitative program involving full weightbearing and ambulation from first post-operative day and, aiming for stairs climbing from third or fourth post-operative day onward.
Outcome measures
All the functional evaluations were carried out by trained physiotherapists following a standardized protocol. The assessors were blinded to the implant type. Each patient was evaluated 2 weeks prior the elective TKA, 6 months and 2 years after the surgery. ROM of the knees were assessed using a goniometer placed on the lateral side of the knee with the limbs of the goniometer in line with the greater trochanter proximally and the lateral malleolus distally.
The assessment of health-related quality-of-life was performed with Short Form-36 Health Survey (SF-36). There are eight scales in the SF-36 health survey score: physical functioning, role-physical, bodily pain, general health, vitality, social functioning, role-emotional, and mental health. 26 With the use of the eight domains, summary scale scores for Singapore were calculated via a validated formula 27 to compute the Physical Health summary scale score (physical component score [PCS]) and Mental Health summary scale score (mental component score [MCS]). The PCS and MCS are scored from 0 to 100 with 100 being the best outcome. Disease-specific outcomes were quantified with Knee Society Score (KSS) and Oxford Knee Score (OKS). KSS evaluated on patients’ symptoms of pain, knee alignment, stability, and joint motion. Similar to SF-36 scores, it is also scored from 0 to 100 with 100 being the best outcome. It consisted of two components; Knee score and Functional score. Knee score is an objective evaluation while functional score is a subjective evaluation of patient’s symptoms and function. 20 The OKS is a 12-item Patient Reported Outcome specifically designed and developed to assess function and pain after TKA. 28 It evaluated on patients’ symptoms of knee pain and coping with activities of daily living. It scored from 12 to 60 with 12 being the best outcome and 60 being the worst.
Statistical analysis
Statistical analysis was performed with IBM® SPSS Statistics Software Version 23.0. Power analysis was performed to reveal that 37 knees in each group were sufficiently powered to detect a mean difference in functional score of 20 with a SD of 30, taking power at 80% and significance at 0.05. The difference in functional score of 20 was based on the minimally clinically important difference (MCID) of at least 10 points in SF-36 for TKA. 29 For comparison of categorical variables between the groups, univariate analysis was performed with use of Chi-square. The data for continuous variables was presented with median as the measure of central tendency with the range between first and third interquartile. Mann–Whitney U test was used to compare the continuous variables with non-parametric distribution for univariate analysis. For multivariate analysis, ANOVA with repeated measures was used to compare each outcome measure between PS and CR groups over the 24-month period. A p value of <.05 was considered significant.
Ethical approval was granted by the institution’s Centralised Institutional Review Board (CIRB reference: 2018/3131 prior to commencement of the study.
Results
There was a total of 112 knees (104 patients) included in the study. All patients were reviewed for pre-operative scores as baseline. At 6 months post-operation, six CR and four PS knees defaulted for follow-up. All patients returned for review at 2-year post-operation for clinical and functional scorings. There were 56 knees (50 patients) in Group CR which were matched with 56 knees (54 patients) in Group PS according to age, gender, and BMI.
Patients’ characteristics (median; IQR).

Abbreviations: interquartile range (IQR).
Intra-operative details.

Abbreviations: cruciate retaining (CR); interquartile range (IQR).
Clinical and functional outcomes
Coronal tibiofemoral alignment (median; IQR).

Abbreviations: cruciate retaining (CR); interquartile range (IQR).
Pre-operative outcomes (median; IQR).

Abbreviations: cruciate retaining (CR); Knee Society Score (KSS); interquartile range (IQR); mental component score (MCS); Oxford Knee Score (OKS); physical component score (PCS).
Post-operative clinical and functional outcomes (median; range).

Abbreviations: cruciate retaining (CR); Knee Society Score (KSS); mental component score (MCS); Oxford Knee Score (OKS); physical component score (PCS); Posterior Stabilized (PS). P-value1: statistical significance of outcomes at 6 months compared with baseline. p-value2: statistical significance of outcomes at 2 years compared with baseline.
In terms of functional outcomes, both Group CR and PS were able to achieve significant improvement for KSS, OKS, and SF-36 scores (Table 5, Figures 1–3). For KSS Function score, Group CR has achieved statistically significant improvement from pre-operative baseline score of 45 to post-operative 6 months score of 65 (p—value1 ≤ .001). It has also achieved significant improvement from the baseline score to post-operative 2 years score of 75 (p—value2 ≤ .001). On the other hand, Group PS has achieved significant improvement from baseline score of 45 to post-operative 6 months scores of 60 (p—value1 ≤ .001). Significant improvement was also achieved from the baseline score to post-operative 2 years score of 70 (p—value2 ≤ .001). The repeated measures ANOVA test has showed that there were no statistically significant differences in the KSS function score over the 2 years duration between Group CR and PS (p = .485). These findings were similar for the rest of the functional scores for both Group CR and PS as illustrated in Table 5. This has shown that Group CR and PS were comparable in achieving significant improvements in the functional outcomes. X-ray radiograph of 79-year-old female with pre-operative varus alignment of 21.7° (A and B). CR TKA was performed and achieved correction with post-operative valgus alignment of 9.2°. X-ray radiograph of 61-year-old female with pre-operative varus alignment of 20.9° (A and B). PS TKA was performed and achieved correction with post-operative valgus alignment of 8.9°. Post-operative outcomes.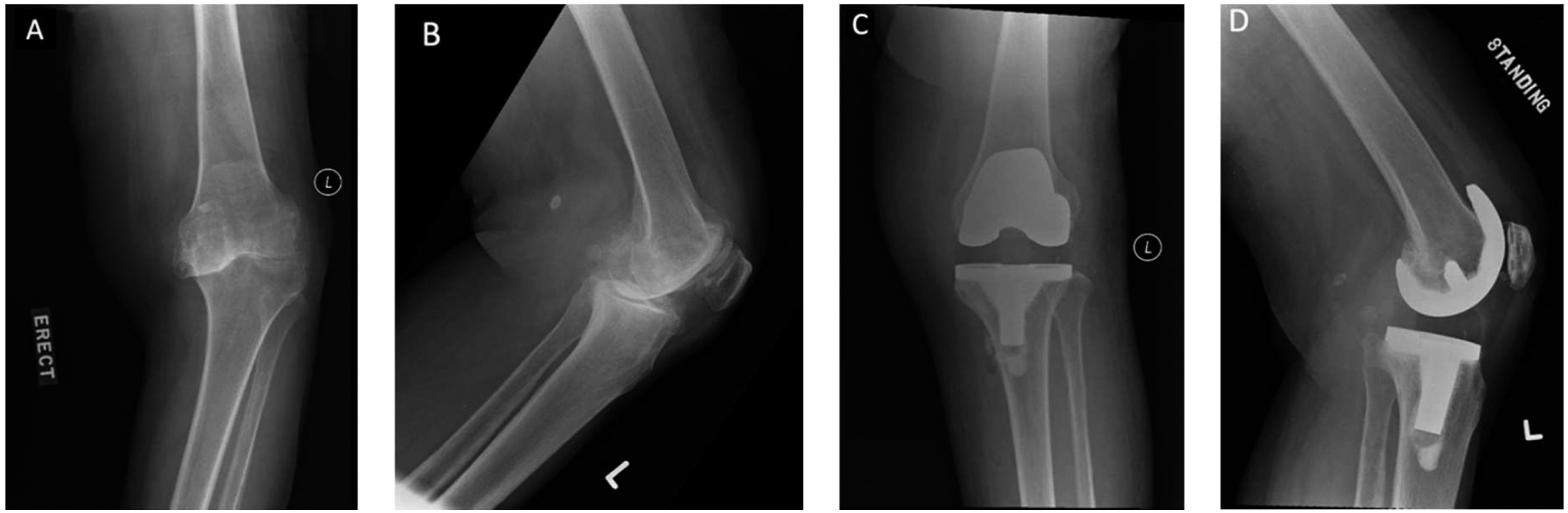


Discussion
The main findings of our study were that CR and PS TKAs were comparable in achieving significant improvement in outcomes in severe varus knees. Our study has demonstrated a comprehensive evaluation on the functional outcomes with the use of patient-reported outcome measures (KSS and OKS scores) and Quality of Life scores (SF-36 scores) during the 2 years follow-up. Our study population has a predominance of female (98 out of total of 112) and overweight patients (median BMI ≥25). 30 These patient demographics were in line with the epidemiological studies which reported higher prevalence of female and obese patients with diagnosis of osteoarthritis knee.31,32
A similar study by Ünkar et al. was performed for severe varus knees and reported no significant difference between CR and PS TKAs in terms of KSS scores, flexion arc, and knee alignments. 33 These findings were in keeping with our study that both CR and PS TKAs were non-superior to each other in terms of clinical and functional outcome in severe varus knees. As compared to the former study, our study has focused specifically on coronal deformities by excluding knees with severe sagittal deformities (fixed flexion deformities ≥15°) and our choice for a match-paired study design has conferred a homogenous study population for comparison. Our study has also reported additionally on the intra-operative usage of surgical augments. To the authors’ knowledge, there were no other two-arm studies comparing between CR and PS implant designs that focused on knees exclusively with severe varus deformities and in an Asian population.
Profound deformities in knees can pose many challenges to surgeons as they entail attention to bony alignment and soft tissues balancing. It is paramount for surgeons to achieve a balance between the constraint of the implants and the stability of knee. Inability to do so could lead to early catastrophic failure with accelerated polyethylene wear or peri-implant loosening. In knees with severe coronal deformities, some studies have proposed the use of highly constrained or hinged protheses to achieve proper correction of the deformities without the need to restore soft tissues balance.34,35 In our study, both group CR and PS had a median follow-up of 65 and 74 months, respectively (Table 1), and there were no reported cases of revision surgery for aseptic loosening during the follow-ups.
Ritter has studied on CR TKAs on knees with angular varus or valgus deformity of ≥20° and reported a slight tendency to under-correct the deformities. 16 Teeny compared the results in CR TKAs between knees with pre-operative varus deformity of ≥20° and those with <5°, and reported slightly lower (but not statistically significant) correction of mechanical axis in the varus deformity group. 36 In our study, our CR group was able to attain similar post-operative neutral knee alignment as the PS group (Table 3). Both designs achieved neutral mechanical alignment with post-operative median valgus anatomical angle of 4.9° for CR and 4.0° for PS. There was no significant difference between the two groups (p = .408).
One of the potential advantages of PS over CR TKAs, as suggested by the literature, was the increased ROM. The Cochrane studies performed by Jacobs et al. 4 and Verra et al. 5 have reported significantly higher ROM in the PS TKAs. In our study, our results were consistent with the literature in showing higher post-operative ROMs in PS TKAs (Table 5). However, this was not shown to be statistically significant. This is likely attributed to favorable pre-operative ROM of the knees in our study in which we excluded knees with pre-operative severe fixed flexion contractures.
In our study, we have also evaluated and found no differences on the usage of polyethylene insert sizes and surgical augmentations between CR and PS TKAs (Table 2). One of the possible challenges in CR TKAs for severe varus knees is the narrow flexion gaps due to the retention of the contracted PCL. Several studies have found the influence of flexion and extension gap with resection of PCL during TKA.37,38 Kadoya et al. has found significant increase in flexion gaps when the PCL was resected in PS TKA. The PCL resection could result in average increase in flexion gap by 4.7 mm and make space for approximately 3 mm thicker polyethylene inserts. 38 Hence, when PCL is retained in CR TKAs, the narrow flexion gaps may limit the thickness of polyethylene and lead to higher risk of polyethylene fracture, and catastrophic failure. In our study, the median thickness of polyethylene inserts used in Group CR was found to be thinner as compared to Group PS (Table 2). However, the difference was not found to be statistically significant.
The use of surgical augmentations can be indicated in primary TKAs when there is significant bone loss, primarily in the medial-sided proximal tibia in severe varus knees. The usage of surgical augmentation in our study can reflect on the degree of bone loss and deformities of the knees evaluated intra-operatively. With that, our study has found no differences between group CR and PS in terms of the degree of bone loss and deformities warranting the use of augments (Table 2).
There were several limitations identified in our study. Firstly, it was the small sample size of our study population which could lead to bias and increased type II errors. 39 However, our study has evaluated to have sufficiently powered to detect the MCID for functional score in SF-36 for TKA. 29 Secondly, the retrospective nature of our study and relatively short duration of follow-up results may not effectively depict the long-term outcome of the patients. Although our study has a median follow-up duration of up to 74 months, we have reported on 24 months of outcome scores. This was due to the logistical limitation of the centralized diagnostic center which collected up to 24 months of outcome scores. The patients who have been operated for more than 5 years ago will be recalled for assessment to evaluate on the long-term outcomes for subsequent studies. It is noteworthy that most of the TKAs that would require revision TKA did so during the early perioperative period. The American Joint Replacement Registry has highlighted that 68% of patients who underwent revision TKA between 2012 and 2013 did so within 3 months of the initial procedure. 40
Next, our study population was heterogenous in terms of the use of different surgical techniques. There was a lack of multiple regression analysis to control for these confounding factors. Nonetheless, we have match-paired the Group CR and PS in attempt to create a uniform study population in terms of patients’ demographics. Lastly, the pre-operative and post-operative anatomical angles were measured using short standing AP knee radiographs. There can be potential inaccuracy in the measurement of anatomical angle using short standing films as compared to the measurement of mechanical angles with full-length lower limb films. 41 The measurement of the anatomical tibiofemoral angle was performed by a senior resident under training. There was no available statistical evaluation for inter-observer or intra-observe reliability. Regardless, the limitations of our study do not undermine the important finding that CR TKA can achieve equivalent functional outcomes as PS TKA for patients with severe varus knees.
Conclusion
Both PS and CR TKA designs are able to achieve equally good clinical and functional results over 2 years for severe varus deformities. Further studies are warranted to assess the long-term outcomes and survivorship between the two implant designs.
Footnotes
Acknowledgments
I would like to express my special gratitude to Prof Yeo Seng Jin for his patience and guidance through my work for this project. I would also like to extend my gratitude to Dr Youheng Ouyang for his valuable suggestions and guidance in the making of the manuscript for this project. We would like to thank Orthopaedic Diagnostic Centre in Singapore General Hospital for providing the informative data relevant for the study.
Author contributions
This study was designed and carried out by above authors. A/Prof SJY, as the principal investigator, has provided the conceptual and administrative guidance for the project. The acquisition of data, interpretation and analysis of data, and drafting of the manuscript was performed by Dr JS. Dr YOY has contributed in the data interpretation and revising of the manuscript. The manuscript was commented on by all authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Singhealth CIRB D CIRB Ref: 2018/3131.
Informed consent
Informed consent was not required as there were no anticipated risks to the subjects in the retrospective study.