
Abstract
Purpose
This study aimed to evaluate the clinical and financial outcomes of the My PreHab Program (MPP), a digitally delivered, patient-led prehabilitation initiative for patients undergoing elective hip or knee arthroplasty across two metropolitan hospitals.
Methods
An observational cohort study of MPP participants compared to a standard care group (SCG). MPP participants were invited via text message to complete a Health Assessment Questionnaire (HAQ) and received tailored health information on modifiable risk factors. For analysis, demographic data, length of stay (h = hours), hospital-acquired complications, readmission rates and hospital costings were collected from hospital records and the digital platform’s website.
Results
A 24-h reduction in length of stay was observed in MPP participants compared to the SCG (MPP: 107 h vs SCG: 131 h, p = <0.001). The average cost of an admission for MPP participants was $2,251.85 less than SCG. MPP participants rated the program as acceptable (3.6/5), appropriate (3.6/5), and feasible (3.8/5).
Conclusion
MPP demonstrated promising results, specifically by reducing length of stay and hospital costs. These findings support broader implementation of digitally delivered, self-administered prehabilitation programs as an effective, affordable strategy in elective surgery pathways.
Introduction
Globally, there is a demonstrated high demand for elective surgery, and healthcare organisations continue to seek more efficient ways to meet this demand. 1 For example, in Australia alone, more than 770,000 patients on public hospital waitlists underwent elective surgery in 2023–24, a 4.9% increase compared with the previous year. 2 This growing demand contributes to broader system pressure and occurs in the context of significant national healthcare expenditure, with Australia spending an estimated $252.5 billion on Health goods and services in 2022–23 and a projected budget of $112.7 billion in 2024-25.3,4
Often, patients undergoing elective surgery at public hospitals experience long waiting periods between referral, first assessment, and then the subsequent surgical procedure. 5 This time tends to be passive, with minimal intervention from general practitioners or hospital clinicians.
However, this waiting period presents a critical opportunity and can be used to support patients to optimise their health before surgery by addressing modifiable risk factors, enhancing shared decision-making and empowering patients to take a proactive role in their care. 6 In perioperative medicine, the focus on health optimisation through patient-centred, multidisciplinary and integrated medical care from the initial consideration of surgery until well after recovery is widely accepted. 7 Despite this recognition, there remains a gap in the consistent implementation of prehabilitation programs within public health systems.
One such initiative is the Central Adelaide Local Health Network's (CALHN) My PreHab Program (MPP), a hospital-initiated, community-based, digital program that supports patients while waiting for surgery. By promoting health optimisation, programs like MPP may reduce surgical risk, improve surgical outcomes, or in some cases, reduce the need for surgery altogether.
This report provides an overview of the outcomes observed after the implementation of MPP. Specifically, hospital costings, length of stay (LoS), hospital acquired complications (HACs) and readmission rates, were compared between MPP participants and those who received standard care (Standard Care Group: SCG). By evaluating these between-group differences, the report seeks to contribute to the growing body of evidence on the effectiveness of digital prehabilitation initiatives in improving patient outcomes, enhancing hospital efficiency, and reducing healthcare costs in public healthcare settings.
Methods
Study design and setting
This observational cohort study was conducted between July 1, 2022, to June 30, 2024, in CALHN across two metropolitan acute surgical sites involving patients waitlisted for primary hip or knee arthroplasty. A total number of 558 patients were included in the analysis (MPP participants: n = 116, SCG: n = 442). Full details of the initial co-design and user testing of MPP as well as program implementation, cohort description, and feasibility are outlined elsewhere. 8
Briefly, patients newly referred for surgery were invited to participate in the study at two entry points: initially by clinical staff upon receiving a referral for consideration of hip and knee joint replacement surgery or later when added to the surgical waitlist following a surgeon’s review. MPP participants were then sent a cold-text message inviting them to register on the online platform, where they received a welcome message outlining a typical surgical journey and the role of prehab, along with a Health Assessment Questionnaire (HAQ; Supplement A). The HAQ was a study-specific health screening tool, designed to assess modifiable risk factors.
Upon completion, MPP participants received tailored health information regarding identified modifiable risk factors and targeted, practical self-management resources and/or access to primary care support. Participants also received a personalised summary letter based on their responses. MPP followed patients throughout their surgical journey with follow-up at 2-weeks post registration and then at either 2 or 6-monthly intervals until surgery, and again 6 weeks post-operatively. Participation in MPP was voluntary, with all participants providing digital informed consent.
Patients in the SCG received usual care, which did not include systematised proactive pre-surgical health optimisation beyond what was provided by individual healthcare providers during primary care visits or at surgical consultations.
Comparator
Comparators included two groups, those who participated in MPP and SCG patients within the same timeframe (July 1, 2022–June 30, 2024) who either: (a) did not participate as they had been wait listed for surgery before the program had been implemented; or (b) were not invited to join MPP as they did not have an active mobile phone number therefore were unable to receive a digital invitation to the platform; or (c) those who received an invitation to join the program but did not engage with the initial invitation or activities within the platform.
Data collection and measures
This study used standard hospital-recorded metrics to evaluate the impact of the MPP on participants’ outcomes. Key measures included data collected from the electronic medical record (EMR) focusing on LoS measured in hours (from admission to discharge), American Society of Anaesthesiologists (ASA) status classification, and hospital-acquired complications (HACs), recorded under predefined categories including delirium, cardiac complications, healthcare-associated infections, respiratory complications, and venous thromboembolism. Hospital costings, including direct costs, were provided by the hospital’s finance department as total admission-level costs per patient, based on internal casemix data. Patient demographic data for MPP participants were collected from the HAQ and engagement with the digital platform and educational materials was downloaded from the pathway provider’s (Personify Care) website. Participants’ views on MPP, including user experience and perceived usefulness, were collected via the digital platform at 2 weeks post-registration and again post-operatively.
Cost comparisons were made between MPP participants and SCG within the implementation period (FY 2022/23-2023/24).
Analysis/statistics
Due to sample size differences, all analyses were conducted using unpaired tests. Descriptive statistics, two-tailed independent t-tests, cross-tabulation, and chi-square tests were conducted using IBM SPSS Statistics (Version 29). Descriptive statistics were used to summarise demographic characteristics and costing data. Associations between demographic variables and cost outcomes for MPP participants and SCG were analysed with the threshold for statistical significance set at p < 0.05.
Ethics
The initial design, development and user-testing were approved by the organisation's Human Research Ethics Committee (HREC) (approval #15507). From July 1, 2022, the project was regarded by hospital HREC as an evaluation of a quality improvement initiative and provided publication approval (21509).
Results
MPP participant engagement
During the study period (July 2022 and June 2024), participation in MPP was high. Of the 1618 invited to the platform, 1253 (77%) registered and 1190 (95.0% of those who registered) completed the HAQ. Following completion of the HAQ, participants were provided with tailored health information based on their responses as well as a summary report. Engagement with this information was high, with 1086 (87%) accessing the summary report. As seen in Figure 1, when information about modifiable risk factors was generated for participants to review, they were consistently accessed by participants. Health information areas provided versus accessed by participants.
Cohort demographics
Between July 2022 and June 2024, 1614 people had total knee or total hip arthroplasty surgery. Of this 1,614, 898 were excluded from this project as they underwent emergency or non-elective admissions. An additional 158 were excluded due to having procedures other than primary hip or knee replacements (e.g., revision arthroplasties). The remaining 558 patients were included in the analysis, of whom, 116 were MPP participants. Details of the analysis group, eligibility, invitation, uptake, and exclusion are summarised in Figure 2. Patient flow of study cohort.
Demographic information.

Abbreviations: IQR, interquartile range; THR, Total Hip Replacement; TKR, Total Knee Replacement; IRSD, index of relative socioeconomic disadvantage; ASA, American Society of Anaesthesiologists. NB: Numbers represent n (%) unless specified by * to represent years.
In both cohorts more than a third of participants resided in areas of significant socioeconomic disadvantage, as defined by the lower three deciles of the Index of Relative Socio-Economic Disadvantage (IRSD) (43.7%, n = 193 vs 39.7%, n = 46, p = 0.437). Overall, 137 participants (24.6%) resided in rural or regional areas, with a greater proportion of them in the SCG (117, 26.5% SCG vs 20, 17.2%; MPP participants, p = 0.040). Of the 558 individuals in this study, 507 had ASA physical status scores recorded in EMR (SCG = 401, MPP participants = 103). The median ASA status score was 2 for the MPP group and 3 for the SCG group (p = 0.005). While this difference is statistically significant, both groups were predominantly in the lower-risk ASA categories, suggesting broadly comparable preoperative health status.
Clinical and cost outcomes
During the study period (July 2022 to June 2024), the average LoS for MPP participants (x̄ = 107 h, IQR 72.2–129.3) was 24 h shorter than the average LoS for SCG (x̄ = 131 h, IQR 77.9–154.2, p = <0.001, 95% CI 10.94–37.81). This difference is further illustrated in Figures 3 and 4. Associated with the reduction in length of stay for MPP participants, the average cost of an admission was 6.9% lower compared to the SCG, equating to a cost saving of $2,251.85 per admission (p = 0.199). This cost reduction for MPP participants was consistent across both comparison periods (2023/24 and 2022/23). A breakdown of the costings can be found in Table 2. Distribution of length of stay (hours) for MPP participants. Distribution of lenth of stay (hours) for standard care group. Breakdown of average costs between program participants and SCG during implementation period.


Breakdown of hospital acquired complications between MPP participants and SCG.
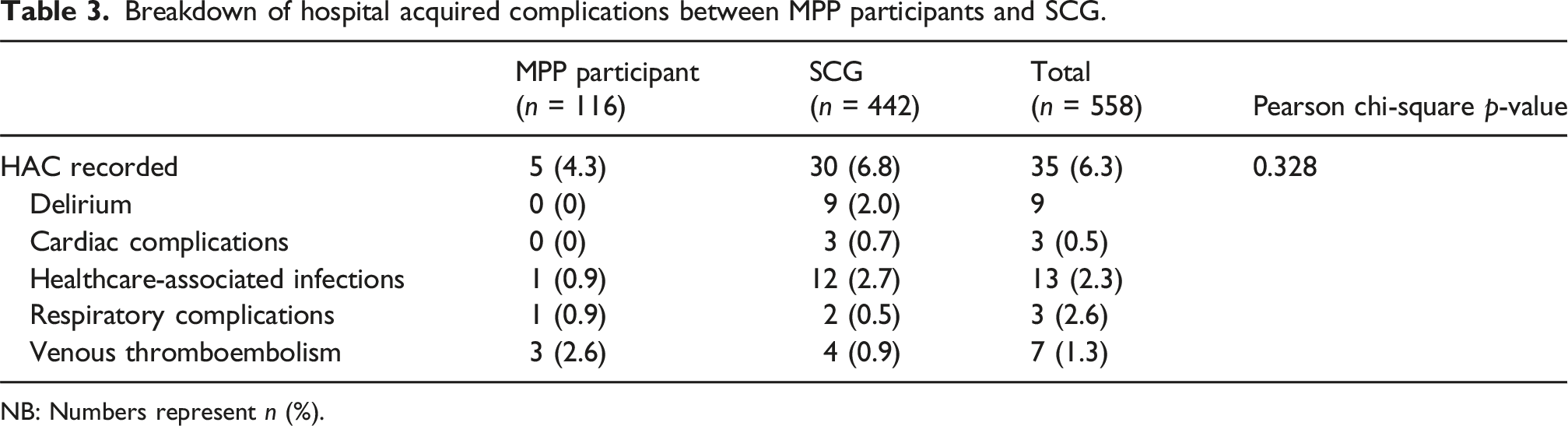
NB: Numbers represent n (%).
Participant feedback
Of the 116 MPP participants, 66% (n = 74) provided feedback 6 weeks post-operatively via the digital platform. When asked whether the My PreHab Program helped them prepare for surgery, the majority of either ‘somewhat agreed’ (n = 33, 45%) or ‘strongly agreed’ (n = 25, 34%). Additionally, 81% (n = 60) stated that they worked on improving health areas identified through the initial health questionnaire completed at registration.
On a five-point scale, MPP scored an average of 3.6 for acceptability, 3.6 for appropriateness and 3.8 for feasibility, with rare negative ratings, see Figure 5. Acceptability, appropriateness and feasibility of MPP post-operatively.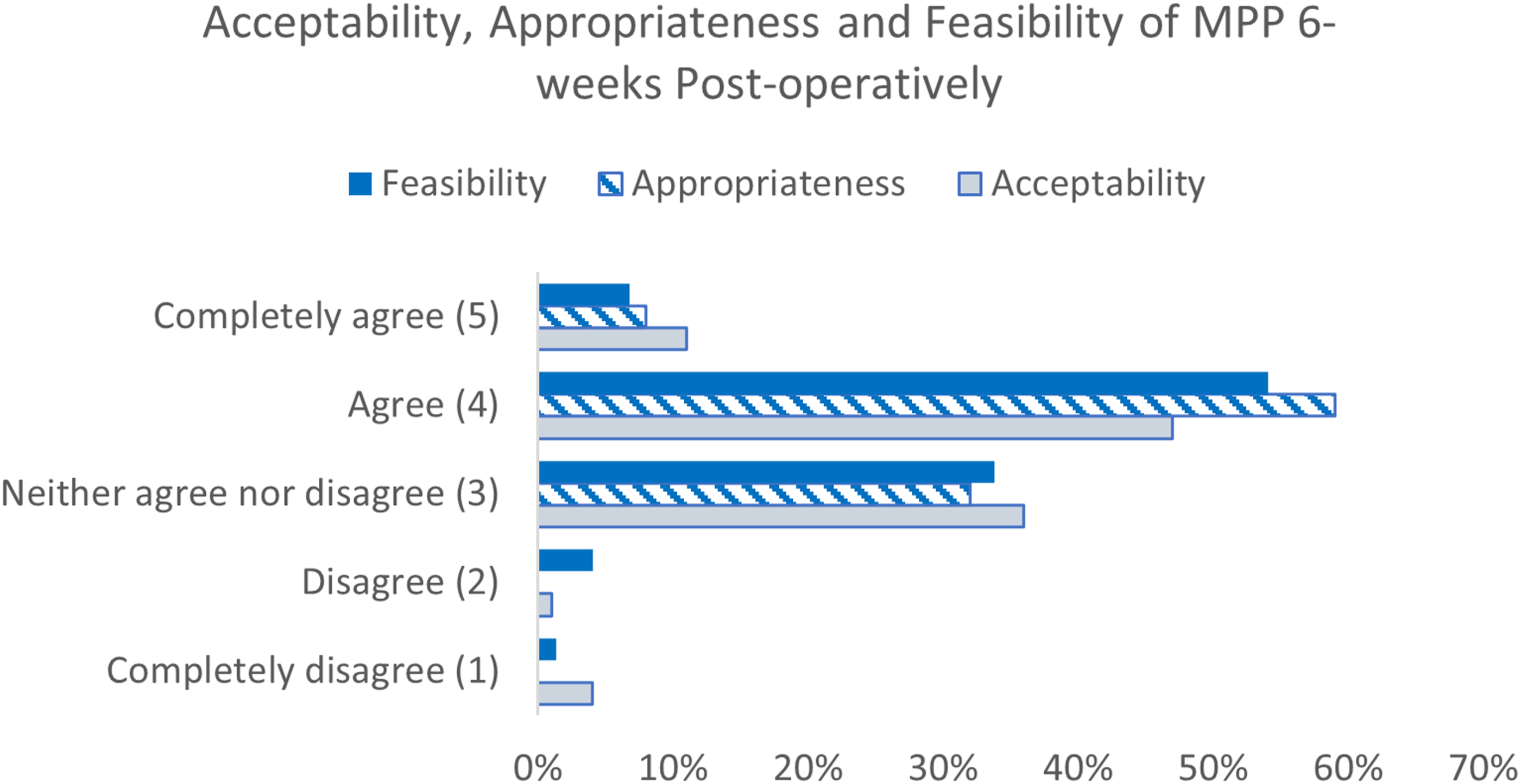
Discussion
Our findings indicate a strong correlation between patient-led health optimisation during the pre-surgical waiting period and reduced length of stay. A 24-h reduction in LoS represents a meaningful improvement in recovery time, with the additional benefit of improving patient flow through the system and thus reducing wait times for other patients. Additionally, despite not reaching statistical significance (p = 0.199), the current results show a trend toward a reduction in HACs for MPP patients, which may partially explain the reduced LoS and additionally deliver gains in patient safety and hospital performance. These clinical benefits are further amplified by a $2,251.85 reduction in the average cost of admissions in MPP participants, highlighting the cost-effectiveness of the intervention and its potential benefits for healthcare budgets and resource allocation. Previous studies have highlighted that cost-effectiveness for prehabilitation remain scarce, but reductions in hospital stay and associated costs have been reported in similar contexts. 9
With a global rise in ‘hidden’ waiting lists, leveraging what is often considered passive wait time to enable early pre-surgical health optimisation offers a unique opportunity for patient engagement and system efficiency. Early intervention may have the potential to delay or reduce the need for surgery by strengthening muscles, addressing pain and losing weight, potentially reducing demand. Identifying and addressing modifiable risk factors via targeted health advice well before surgery can support more comprehensive optimisation, further reducing post-operative complications and supporting faster surgical recovery. While MPP may have influenced expectations and perceived surgical preparedness, it is difficult to determine which specific components contributed to the observed reduction in length of stay. Improved consumer understanding of their condition and available options can enhance the quality of care and satisfaction with the surgical journey.
Improvements are also likely to be seen in readmission rates and patient safety metrics by proactively managing risks such as obesity, chronic pain, and frailty before surgery. Early intervention allows consumers, primary care staff and hospital healthcare teams to tailor perioperative plans more effectively, potentially preventing complications that often lead to extended hospital stays or readmissions.
By providing patients with health advice well before a hospital appointment, the program empowers patients to take an active role in their care. This early engagement promotes autonomy, self-management, shared decision-making, and better engagement in pre- and post-operative care plans. Early pre-operative interventions, such as multimodal prehabilitation including exercise, nutritional optimisation and psychological support take advantage of the window between contemplation of surgery and the procedure, improving surgical outcomes, facilitating rapid recovery, and limiting post-operative functional dependence. 10 Enhanced patient understanding may contribute to more efficient perioperative pathways by reducing uncertainty and improving preparedness for surgery.
Given its scalability and adaptability, this light-touch, digital prehabilitation program could be integrated across other surgical pathways and hospital settings. It underscores the value of multidisciplinary collaboration and may serve as an affordable, scalable foundation for broader ‘surgical school’ or surgical coaching programs which have demonstrated benefit across a range of settings.11,12
Potential limitations of the approach and observed results include the observational design, potential participation bias and the relatively small number of participants who have had surgery thus far. This study was also limited by the data available from EMR; more use of digital health questionnaires would greatly improve sample size, data collection and quality allowing for greater comparison between cohorts. Further research with a larger operated cohort and longer-term evaluation are needed to better assess the effect size and help understand potential mechanisms whereby the apparent gains are delivered. The inclusion of validated patient reported outcome measures (PROMs), such as the EQ-5D-5L, would also strengthen the analysis by capturing broader health impacts and patient perspectives. MPP pathways developed more recently have been labelled as ‘My PreHab Program +’ which include more tailored elements such as referral and waitlist management, generalised PROMs (EQ-5D-5L) as well as specialty specific PROMs (e.g., Breast/Body-Q, the Australian Pelvic Floor Questionnaire).
However, it is unlikely that randomised, controlled trials can now be ethically justified as the gains demonstrated from prehab to date are real and the approach delivers no harm to participants, meaning that genuine equipoise in group assignment cannot be said to exist.
Conclusion
In summary, this study supports digitally delivered, self-directed prehabilitation as a cost-effective, patient-centred strategy that improves surgical outcomes, reduces hospital costs, and enhances hospital efficiency. By embedding a simple digital intervention into the elective surgery pathway, patients can be empowered to optimise their health, leading to measurable clinical and operational benefits. This approach to prehabilitation is a real world, pragmatic example of how targeted, patient-centred interventions can be effectively integrated with existing healthcare systems to improve surgical outcomes and optimise resource use. These findings highlight the potential for prehabilitation programs to transform elective surgery in healthcare systems and warrant further research to assess long-term outcomes and broader implementation.
Supplemental material
Supplemental material - A ‘light touch’ digitally delivered, self-administered, prehabilitation pathway was acceptable to consumers and improved surgical outcomes for elective hip and knee replacements
Supplemental material for A ‘light touch’ digitally delivered, self-administered, prehabilitation pathway was acceptable to consumers and improved surgical outcomes for elective hip and knee replacementss by Anastasia D. Westin, Eleanor Bills, Anne L. J. Burke, Kathryn L. Collins, Jane M. Andrews in Journal of Orthopaedic Surgery.
Footnotes
Acknowledgements
The authors would like to thank the CALHN My PreHab Program Steering Committee members for their valuable knowledge and ongoing support of the program; Vicki Hume, A/Prof Ecushla Linedale, Sharyn Coles, Dr Jackie Yeoh and Mandy Nolan.
Funding
The authors disclosed receipt of the following financial support for research, authorship, and/or publication of this article: this work was supported by the Hospital Research Foundation Group (2021/57-QA25315).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.