
Abstract
Introduction and Aim:
Modern knee replacements aim to improve patient function in arthritis affecting different compartments of the knee. This study evaluates the Patient Reported Outcome Measure (PROM) and functional outcome of a modern total knee replacement (Attune, DePuy) in patients with isolated patellofemoral arthritis.
Methods:
A total of 50 consecutive patients with isolated unilateral patellofemoral arthritis having had Attune total knee replacements at a single institution between 2010 and 2016 were prospectively studied. Five patients who developed symptoms on the opposite side during the study and two patients lost to follow-up were excluded. One patient needed early revision for loosening, leaving a total of 42 patients to be followed up over a period of 4 years. The Oxford Knee score (OKS) and Knee Injury and Osteoarthritis Outcome Score (KOOS) recorded pre-operatively and at follow-up was compared. A Functional assessment at around 8 months after operation was undertaken.
Results:
At average follow-up of 24 months the mean OKS score improved by 15 points and the KOOS score improved by 20 points. Final KOOS sub-score for Pain was 80, Symptom 80, and ADL 82, Sports & Recreation 32 and QOL 60. Functional assessment at mean 8 months showed that a significant number of patients were able to Kneel (50%); Sit cross legged (23%); sit on their heel (23%) and were able do a single leg dip test (86%).
Conclusion:
This unique study of a modern design total knee replacement (Attune) in patients with isolated unilateral patellofemoral arthritis shows good PROM scores at 2 years and good functional assessment results at 8 months. The PROM scores are marginally better than the published results with Attune’s predecessor, in a similar cohort of patients, but falls short of the published results of patellofemoral replacement implants. Large randomised comparative studies between traditional and the modern implant design is recommended to answer the question if design modification has influenced clinical outcome in patients with patellofemoral arthritis.
Introduction
Isolated patellofemoral arthritis is seen in about 13–15% of patients over the age of 60 years. 1 The aetiology is unclear but the altered biomechanics at the patellofemoral joint is believed to be the main cause of progressive patellofemoral degeneration and eventually established patellofemoral osteoarthritis. 2 Severe isolated patellofemoral arthritis can be treated with total knee replacement. 3 –8
Total knee replacement in general gives a good result but some patients continue to suffer from pain, patellofemoral crepitus and reduced range of movements, which limit their function. The origin of the pain or its contribution to functional limitation is difficult to understand but prosthesis design 9 and surgical errors including patellofemoral mal-tracking, patella tilt and over stuffing of the patellofemoral joint have been reported. 10 To overcome these problems and to improve overall function, Implant manufacturers continue to modify the design of their prosthesis. One such modification in design is the Attune total knee replacement over its predecessor the Press Fit Condylar (PFC). Theoretically, this improved design is meant to provide an improved patellofemoral articulation. It remains to be seen if the modified design has influenced the outcome of patients undergoing replacement for isolated patellofemoral arthritis.
Some studies have used Patient Reported Outcome Measure (PROM) data to compare the modified design of a total knee replacement with its predecessor. 11 –14 All these studies however, included heterogeneous groups of patients with degeneration affecting one or more compartments of the knee.
The aim of this study is to evaluate the PROM and functional outcome of a select group of patients with isolated unilateral patellofemoral arthritis undergoing total knee replacement with a modern knee prosthesis design (Attune Depuy).
Patients and methods
After obtaining approval from the hospital committee all patients undergoing Attune total knee replacement (DePuy Synthes, Warsaw, Indiana, USA) between Feb 2010 to Feb 2016 for predominantly patellofemoral arthritis were selected for the study. Patient selection was based on the appearance of severe degeneration isolated to the patellofemoral joint on pre-operative weight bearing Anterior-Posterior (Merchant View), lateral and skyline radiographs. All patients had significant disabling symptoms and had failed conservative non operative treatment. The prospectively recorded PROM data and prospectively recorded functional assessment were studied.
All these operations were carried out by a single surgeon in an identical fashion through a medial para-patellar approach. The posterior cruciate ligament (PCL) was sacrificed in favour of a PCL stabilised femoral prosthesis. The Patella was resected and replaced in a uniform fashion. A fixed bearing modular tibial bearing was used in all cases. The patella was always resurfaced unless it was too thin to do so. There was no change in wound closure, post-operative care, and thromboprophylaxis was in accordance with hospital policy. Thromboprophylaxis involved foot and calf compression pumps in the immediate post-operative period, compression stockings for 6 weeks, and Low molecular Heparin for 2 weeks. All the patients underwent the same post-operative physiotherapy and were reviewed at 6 weeks, 8 months and up to 4 years. Before the operation and around 24 months after the operation each patient had to complete patient outcome questionnaires. If the range of movement of the knee at 6 weeks was less than 90 degrees, they underwent a closed manipulation.
Exclusion criteria
Patients with pre-operative radiograph showing Kallgren Laurance 15 Grade 2 or more degeneration in any part of the knee other than the patellofemoral joint were excluded from the study. Patients where the clinical notes had suggested symptoms of pain, stiffness, swelling or having had a knee replacement on the opposite knee were also excluded from the study. Patients who developed symptoms in the opposite knee during the study period were also excluded. Thus, the best effort was made to study a cohort of patients with isolated unilateral patellofemoral arthritis.
Outcome measures
The demographic data, comorbidities, post-operative complications, and physiotherapy records of the selected patients were studied. Prospectively recorded Patient reported outcome measures (PROM) consisting of Knee Injury and Osteoarthritis Outcome Scores (KOOS) and Oxford Knee Scores (OKS) were analysed.
The Oxford Knee Score is a patient reported response to 12 questions. These relate to pain and function. Each question is scored from 0–4. The KOOS consists of 42 items divided into five subgroups namely Pain, Symptoms, Activities of daily living (ADL), Sports & recreation and Quality of life (QOL). All subgroup scores are standardised on to a 0 to 100 scale.
Our primary outcome was PROMs data at around 24 months after the operation as a comparison to the pre-operative data.
Secondary outcome measures were the range of movements measured by the physiotherapist and a functional assessment in the clinic at 8 months’ follow-up.
Functional assessment undertaken in the clinic involved an assessment of the patient’s ability to perform a ‘Single-leg dip’ on the operated leg, ability to get up from a chair by just using the operated leg without arm support, the ability to kneel, sit on the heel and sit cross legged. ‘Single leg dip’ was defined as the ability of the patient to stand and slowly bend the operated knee as shown in Figure 1. Kneeling in our assessment was defined as the patients’ ability to take pressure on the operated knee against a soft surface with knee flexion more than 90 degrees (Figure 2). ‘Sitting on the heel’ was defined as increased knee flexion after kneeling as demonstrated in Figure 3. ‘Sitting cross legged’ was defined as sitting in a posture as demonstrated in Figure 4. The Range of movement of the knee was measured by the physiotherapist using a long arm goniometer with the patient lying supine and asked to flex the knee as demonstrated in Figure 5.

Single leg dip test demonstrated.

Kneeling demonstrated.

Sitting on heels considered possible as demonstrated.

Cross legged sitting demonstrated.

Position for measuring knee range of movement by the physiotherapist using long arm goniometer.
Analysis
Using the mean 24 months follow-up KOOS score we also counted the number of patients showing less than Minimal Detectable Change (MDC) to distinguish a true change in their score as opposed to that caused by measurement error. Numerical value of the KOOS score from a previously published study 16 was used to set the threshold for MCD. If the difference of pre-operative and 24 months post-operative score was less than 15 points for Pain, less than 16 for symptom, less than 15 for ADL, and less than 14 for QoL, it was assumed that it is very likely that the patient’s true score is outside the reported score.
Substantial Clinical Benefit (SCB) is the lower boundary for a change in score to define the optimal clinical patient benefit. We counted the number of patients who showed Substantial Clinical Benefit using the KOOS threshold numeric data from a large published study. 16 Thus, patients who showed a change greater than 22 for pain, more than 21 for symptoms, 15 for ADL and 23 for QoL subgroup were considered to have had Substantial Clinical Benefit.
Results
Between Feb 2010 and Feb 2016, 76 patients had total knee replacement for predominantly patellofemoral arthritis. 20 of these were excluded as they had a prosthetic joint in the opposite knee. Six patients were excluded as their radiographs showed degeneration of greater than Grade 2 Kallgren Laurance 15 in the tibiofemoral compartment. Thus, 50 patients with unilateral isolated patellofemoral arthritis were prospectively studied. During the study period five patients reported significant symptoms on their opposite knee and had to be excluded. Two patients were lost to follow-up. One patient who had initially been lost to follow-up presented with symptoms and radiological signs of loosening at 16 months and had a revision for aseptic early loosening at 26 months. The patient was excluded from the study as the 8-month functional record had not been undertaken. PROM score (OKS and KOOS) and functional assessment of 42 patients are reported (Table 1).
Patient flow chart showing inclusions and exclusion.


Basic demographics
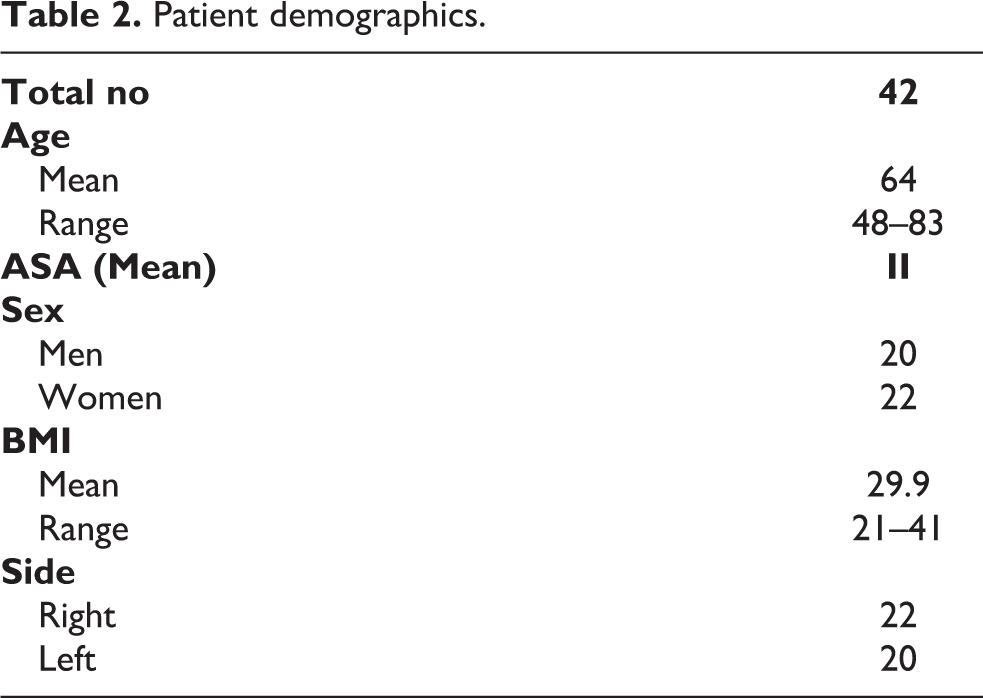
Table 2 illustrates basic demographics data including age, BMI (Body Mass Index) and ASA grade (The American Society of Anaesthesiologists) of the patients included in the study.
Patient demographics.
Patient reported outcomes measures
A marked improvement in the mean 24-month (range 18 to 38 months) post-operative Oxford knee Scores and KOOS scores was seen (Table 3 and Figure 6).
Prospectively recorded PROM data (OKS and KOOS) pre-operative and at follow-up.


Demonstrate the change in KOOS score at mean 24 months follow-up.
OKS
The OKS recorded at mean 24 months (range 18 to 38 months) improved by 15 points when compared to pre-operative score.
KOOS Score
Improvement in the mean KOOS sub-score for Pain was by 30 points, Symptom 20 points, ADL 32 points, Sports & Recreation 22 points and QoL 30 points.
Minimal detectable change (MDC) and substantial clinical benefit (SCB)
The number of patients showing an improvement less than MDC and more than SCB in their KOOS subgroup score have been highlighted in Table 4. The threshold values of the standardised KOOS subgroup score used has been noted in the first column. The number of patients showing MCD is very small. A large number of patients showed Substantial Clinical Benefit in terms of the ADL (Activity of daily living) score and QOL (Quality of life) score.
Minimal change detectable and substantial clinical benefit.
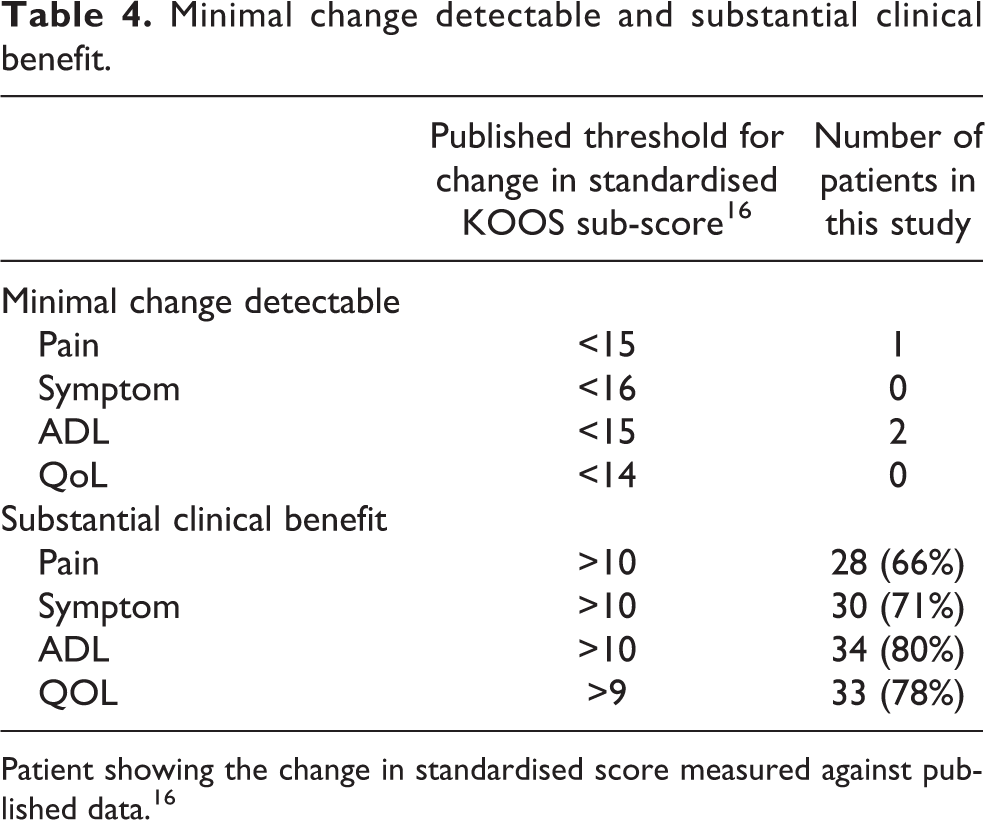
Patient showing the change in standardised score measured against published data. 16
Functional assessment
The functional assessment undertaken in the clinic at 8 months (Table 5) showed that 40 (96%) patients were able to rise from a chair by just using the operated leg; 36 (86%) patients were able to do a ‘Single leg dip’; 21 (50%) could kneel; 10 (23%) could sit on the heel and 10 (23%) could sit with cross legs.
Functional assessment in the clinic.
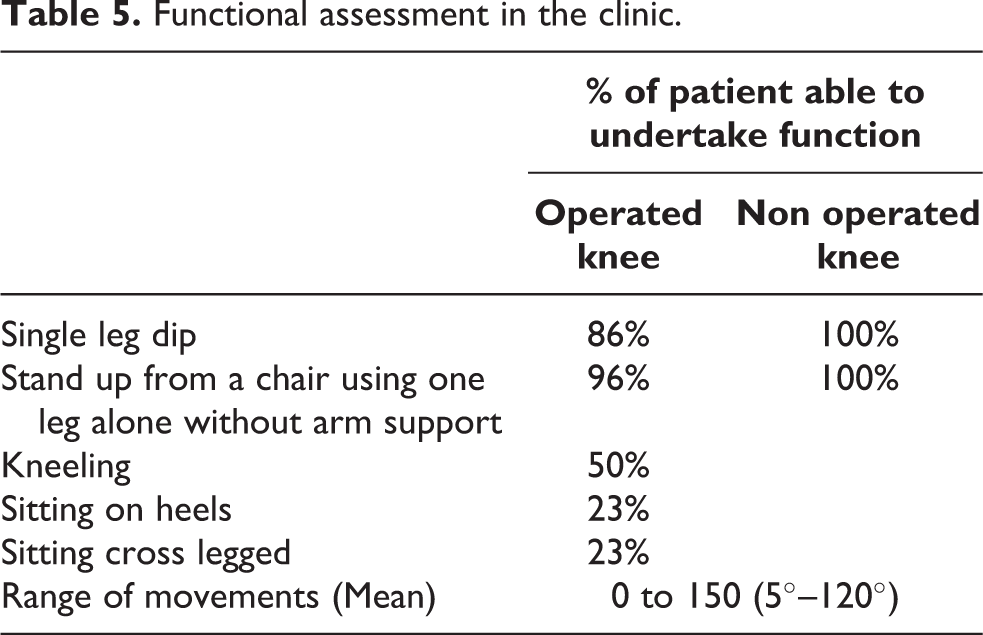
The mean range of movement recorded by the physiotherapist was 5–120 degree at mean 20 months (range 12 to 24 months).
Complications
Table 6 presents complications observed in patients included in this study. There were a number of manipulations undertaken for stiffness. One patient presented with persistent pain and swelling with radiological signs of loosening at 16 months between the cement implant interface. Infection was ruled out by blood tests, aspiration and biopsy. Revision for aseptic loosening was undertaken. Figure 7 shows the tibial surface at the time of revision surgery.
Complications.

MUA: manipulation under anaesthesia.

Operative photograph at the time of revision demonstrating intact cement mantle confirming loosening of the tibial component at the cement implant interface.
Discussion
Patient reported outcome measure (PROM) is a subjective tool to assess different designs of knee replacement prosthesis. 11,17,18 In this study the Oxford Knee Score (OKS) and the Knee Injury and Osteoarthritis Score (KOOS) used as a patient reported outcomes measure and clinic based assessment of various knee function has been used to evaluate the modern design Attune® Knee replacement.
The most important finding of the study is that patients with isolated unilateral patellofemoral arthritis do reasonably well with the modern Attune Knee replacement. The 2-year PROM score (OKS and KOOS) in this select group of patients are marginally better than the published series with its predecessor (PFC sigma) 19 but falls short of the published results for patellofemoral joint replacement in the same cohort of patients. 19
The main strength of the study is that it relates to a homogenous group of patients suffering from isolated patellofemoral arthritis. Patients with involvement of other compartments of the same knee have been excluded from the study. This criteria for selecting patients provides a focus on a specific type of arthritis. We believe that patients with isolated patellofemoral arthritis have different patellofemoral biomechanics 2 thus should be assessed separately.
Patient reported outcome measure like the KOOS is increasingly being used to assess outcome of a prosthesis. 11,17 These scores can be influenced if the opposite knee is either symptomatic or has been replaced. Therefore, in this study we have excluded patients with either a replacement or symptoms on the opposite knee.
The design modification in the Attune prosthesis involves a gradually reducing radius of curvature for the femoral component which is intended to improve knee flexion concurrently providing increased congruency and stability between the femoral component and the polyethylene insert. The femoral component profile at the level of the trochlea has also been reduced and the trochlear groove has been modified to closely mirror the native knee with the aim of improved patella tracking and reduce anterior knee pain. 14 We believe that this is the only study where such design modifications have been assessed in patients with isolated patellofemoral arthritis.
The main limitation of the study is that there is no control group. Comparative studies with this prothesis and its predecessor, in patients with arthritis affecting different parts of the knee, have been published. 11 –13
Our study has other limitations. The mean follow-up period in this study is 2 years. We appreciate that the PROM can continue to improve beyond 2 years after surgery. 20 The number of patients is small which reflects the incidence of isolated patellofemoral arthritis and our selection criteria which excluded symptoms on the opposite side. Our functional assessment involves deep flexion activity like kneeling and squatting which is a reflection of patellofemoral kinematics of the knee prosthesis 21 –23 and are indicators of patient satisfaction. 24,25 However, we have not taken into account other factors like muscle control and limb stability which contribute to such activity.
One obvious limitation is that although we are evaluating component design, we have ignored the modification in the instrumentation and the availability of greater spectrum of component sizes. The Attune unlike its predecessor the PFC has a ‘narrow’ femoral component option which was used in a number of our cases.
We have studied the Minimal Detectable Change (MDC) and Substantial clinical Benefit (SCB) using surrogate data, which is statistically debateable. However, the parameters have been used for descriptive purpose. A large percentage of patients seem to have had Substantial Clinical Benefit which is reflected in a large number of patients who were able to kneel and sit cross legged.
We had one case of early loosening of the cement implant interface although we have not undertaken a detailed radiological assessment for our patients. Such early radiological loosening with Attune prosthesis has been reported by other studies and close observation with long follow-up of radiolucent lines around the prosthesis has been recommended. 26
Severe isolated patellofemoral osteoarthritis can be treated with a total knee replacement or patellofemoral joint replacement. While patellofemoral joint replacement is a more conservative option, a high failure rate with this prosthesis causes some concerns. 3,4 These concerns have led to some centres, including ours, undertaking total knee replacements for patients suffering with isolated patella femoral arthritis. 5 –8 A prospective blinded randomised trial comparing the PFC (predecessor of Attune) and patellofemoral replacement in patients with patellofemoral arthritis found an improvement in the OKS of 10 with PFC and 15 with patellofemoral replacement. The improvement in KOOS score of 17 (Pain 26, Symptom 12, ADL 26, Sorts & Recreation 13 and QOL 29) with PFC as compared to 27 (Pain 33, Symptom 23, ADL 28, Sports Recreation 23, QOL 35) with the patellofemoral replacement. Our results with Attune are marginally better than PFC but short of patellofemoral replacement. 19
We note that in our study we have used a posterior stabilised Attune implant as compared to a posterior cruciate retaining implant in above comparative study. 19 In another study a great improvement of PROMs in Attune posterior stabilised prothesis was seen when compared to posterior stabilised PFC on the opposite knee. 12
A comparative study of different prosthesis design by Chua et al. 11 reported no difference in the overall patient reported score in patients having modern knee implant (Attune) as compared to traditional implants (PFC). In addition, the authors did not find any significant difference when they compared the patellofemoral joint related sub-score.
We note that in our study we have used a posterior stabilised Attune implant as compared to a posterior cruciate retaining implant in this comparative study. 19 In another study a great improvement of PROMs in Attune posterior stabilised prothesis was seen when compared to posterior stabilised PFC on the opposite knee. 12
Ranawat et al. 13 have compared 100 Attune® TKA patients with a matched group of 100 PFC Sigma® TKA patients and found no significant difference in Knee Society Scores but less anterior knee pain and crepitus in patients with Attune prosthesis. In our study, we have not looked specifically for anterior knee pain or crepitus but a large number of patients being able to kneel and sit cross legged would suggest a similar finding.
Another study 18 found a greater improvement in the physical PROMIS-10 (Patient-Reported Outcomes Measurement Information System) between those who were treated with Attune as compared to others who had the PFC implant. The authors point out PROMIS provides a global health score that is not joint specific. We have used a similar score but in patients with unilateral disease.
The introduction of new design of implants, which are often more expensive, often generates a debate on its usage and the justification of additional cost. Some surgeons rely on the ‘old is gold’ concept and are reluctant to adapt new designs while others hasten to change. A number of the studies comparing Attune to its predecessor 11 –13,27 have highlighted that there has been no significant improvement in the patient reported outcome. Some studies have shown some statistically non-significant improvement in knee function or patient satisfaction or the range of movement. 18
Conclusion
In conclusion, this is the first study of total knee arthroplasty in isolated patellofemoral arthritis patients using the modern design of the Attune total knee replacement. Good results on 2-year PROM and 8-month Functional assessment was found. The improvement in PROM, with Attune, is only marginally better than that published with its predecessor but falls short of the published results with patellofemoral replacement in this select group of patients.
Randomised comparative study with longer follow-up is required in this select group of patients to answer the question if the modern design in a prosthesis has influenced clinical outcome.
Footnotes
Authors’ note
All research was conducted at The Royal Orthopaedic Hospital, Birmingham, UK.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.