
Abstract
The treatment of adult cervical deformity continues to be complex with high complication rates. However there are many new advancements and overall patients do well following surgical correction. To date there are now many types of cervical deformity that have been classified and there exists a variety of surgical options. These recent advances have been developed in the last few years and the field continues to grow at a rapid rate. Thus, the goal of this article is to provide an updated review of cervical sagittal balance including; cervical alignment parameters, deformity classification, clinical evaluation, with both conservative and surgical treatment options.
Keywords
Introduction
The cervical spine is very complex as it the largest range of motion relative to the rest of the spine and supports the weight of the head. Due to the complexity of the cervical spine, it’s thus susceptible to various pathology including deformity. The cervical spine’s neutral alignment is one in which it allows the person to assume a comfortable position while simultaneously maintaining a horizontal gaze. Deformity of the cervical spine is debilitating and causes significant dysfunction and reduced health-related quality of life (HRQOL) for the patient. 1 –6 So much so that when cervical deformity is compared to other disease states using the EuroQol-5 Dimension (EQ-5D) HRQOL metric, it is in the bottom 25th percentile which includes other disease such as heart failure, blindness, renal failure, stroke, emphysema, breast and prostate cancer. 7
However, it is very important to note that the alignment of cervical spine is not in isolation and it is very closely tied to the thoracic and lumbar alignment. It plays a crucial role in influencing subjacent global spinal alignment. Moreover, compensatory changes in pelvic tilt occur to maintain horizontal gaze. Prior studies investigating the spinal malalignment and HRQOL relationships have mostly focused on the thoracolumbar and pelvic regions until recently. Normal and pathological cervical alignment parameters have been established, a deformity classification now exists as well as a cervical osteotomy classification. 8 –16
The rate of cervical fusions in the United States has been increasing every year, 17 likely as a result of the recent focus on cervical spine pathology and outcomes. The recent major advancements in cervical deformity management continue to evolve. Therefore, the purpose of this article is to provide a review of the current concepts for cervical deformity.
Cervical alignment radiographic parameters
The role of the cervical spine is to maintain the head over the body and provide a level horizontal gaze so the person may function properly. The center of mass of the head overlies the occipital condyle 1 cm above and anterior to the external auditory canal in the sagittal plane. 18 Deviations from the normal alignment of the mass of the head can cause an increase in cantilever loads on the cervical spine, which then induces increases in muscular expenditure. Thus, an understanding of cervical alignment is crucial when evaluating and defining cervical deformity. Due to the need to compensate for the kyphotic curvature of the thoracic spine, the natural curvature of the cervical spine maintains a lordotic shape. 19 The caudal end of the lordotic cervical spine joins the rigid kyphotic thoracic inlet at the cervicothoracic junction (CTJ). When the cervical spine has reduced cervical lordosis, and in the extreme cases, such as the development of cervical kyphosis, this is associated with pain and disability, 6,19 –22
The most common method to measure cervical lordosis (CL) are Cobb angles typically measured from C1–C7 or C2–C7 (Figure 1). Of note there are two other methods to assess CL and they include Jackson’s physiologic stress lines, and the Harrison posterior tangent method, although they are less commonly used clinically. 23 The Cobb angle measurement includes drawing a line either parallel to the inferior endplate of C2 or extending from the anterior tubercle of C1 to the posterior margin of the spinous process. Then another line is drawn parallel to the inferior endplate of C7. Perpendicular lines are drawn from each of the 2 lines mentioned above and the angle subtended between the crossing of the perpendicular lines is the cervical curvature angle for measuring CL 23 (Figure 1).
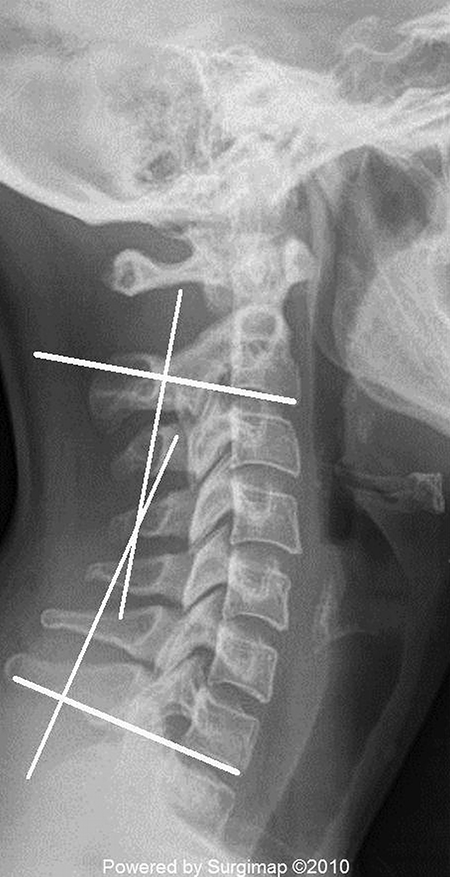
Lateral radiograph showing Cobb angle measurement using the four-line method. The method involves drawing a line parallel to the inferior endplate of C2 or extending from the anterior tubercle of C1 to the posterior margin of the spinous process with another line parallel to the inferior endplate of C7. Then perpendicular lines are drawn from each of the two lines noted above and the angle subtended between the crossings of the perpendicular lines is the cervical curvature angle.
Anterior/posterior translation of the cervical spine in the sagittal plane is primarily measured through the cervical sagittal vertical axis (cSVA). cSVA is defined by using the distance between a plumb line dropped from the centroid of C2 and the posterior superior aspect of the C7 vertebral body (Figure 2). The cSVA is especially clinically relevant as it has been shown to be directly related to HRQOL with larger cSVA resulting in worse HRQOL. 6

Lateral radiograph showing the cervical sagittal vertical axis (C2–C7 SVA) measurement. The vertical white line is a plumbline dropped from the center of C2, and the black vertical line is a plumbline dropped from the postero-superior corner of the C7 vertebral body. The horizontal line with an arrow represents the C2–C7 SVA.
Maintaining horizontal gaze is essential for proper daily function and to measure it the chin-brow vertical angle (CBVA) is used. Loss of CBVA in patients with severe rigid cervical kyphotic deformities, has a significant impact on activities of daily living and quality of life. 24 It is defined as the angle subtended between a line drawn from the patients chin to brow and a vertical line (Figure 3). 24 The angle is measured on clinical photographs of the patient standing with hips and knees extended while their neck is in a neutral or fixed position. 24 When CBVA is considered in deformity correction, studies have shown that CBVA is associated with positive postoperative outcomes, such as improved gaze, ambulation, and activities of daily living. 24 –29

A clinical photograph showing the chin-brow vertical angle (CBVA) measurement method. Reprinted with permission from Scheer JK, Ames CP, and DeViren V, Assessment and treatment of cervical deformity, Neurosurg Clin N Am 24(2), 249–274.
Another important parameter when measuring cervical alignment has become the T1 slope as it’s intimately associated with cervical lordosis. Its measurement is defined as the angle subtended by a line drawn parallel to the superior endplate of T1 and a horizontal reference line (Figure 7). The relationship between CL and the T1 slope plays a large role in classifying cervical deformity as discussed more below. It is analogous to the relationship of pelvic incidence and lumbar lordosis in the lumbar spine.
There exists a wide range of normal alignment due to the cervical spine being the most mobile part of the spinal column. 21,22,30 The majority of cervical lordosis (75–80%) is localized to C1–C2 21,31 in asymptomatic normal volunteers with relatively little CL in the lower cervical levels. The mean total cervical lordosis is approximately −40 degrees, with, on average, the occiput-C1 segment being kyphotic. 21 Only 6° (15%) of lordosis occurs at the lowest three cervical levels (C4–C7). 21 There is no difference in CL between men and women and there is a positive correlation with cervical lordosis and increasing age. 21,30 The average cSVA distance ranges from 15 to 17 +/−11.2 mm. 21 A cSVA greater than 4 cm is associated with worse HRQOL. 6 To date, normal CBVA has not been defined, however postoperative measurements of +/−10° have been well tolerated in patients. 24 –29
Clinical evaluation of cervical deformity patients
Physical exam
The primary goal during the preoperative evaluation of a patient with a cervical deformity is to determine the ideal amount of correction required and the best method to achieve the desired amount of correction. There is no predefined amount of cervical lordosis one should attempt to correct to given the wide range of normal values, however a general rule of correcting the cervical kyphosis to at least neutral has been accepted.
32
When seeing a patient with cervical deformity for the first time, the evaluation begins with the basics such as a complete medical history and physical exam. Many of these patients are frail and at high-risk for surgical complications. Therefore, a relevant medical history (e.g. major medical comorbidities, smoking, use of nonsteroidal anti-inflammatory drugs (NSAIDs, etc.) must be obtained and can aid in tailoring treatment and discussion of potential complication risks. The physical exam should include having the patient standing upright with hips and knees fully extended and in the sitting and supine positions as well as perform a detailed neurological exam. The sitting position removes the effect of lumbar and pelvic/hip deformity and the supine position can helpful to assess the rigidity of semi rigid curves under the direct effect of gravity. Chin-brow vertical angle should be measured before and after surgery (Figure 3) with the patient standing with the hips and knees extended and the neck in its neutral or fixed position.

Clinical photograph demonstrating the supine physical exam component demonstrating a patient with fixed cervical kyphosis. Reprinted with permission from Scheer JK, Ha Y, Sears WR, et al. Cervical deformity and treatment algorithms. In: Shen FH, Samartzis DS, and Fessler RG (eds) The cervical spine. Philadelphia, PA: Elsevier, 2014, pp. 146–154.
Imaging
After the physical exam, the initial radiographic evaluation should always include a 36 inch standing x-ray as well as dynamic flexion/extension cervical x-ray films (Figure 5). The 36 inch standing film allows for measurements of global spinal alignment, which is necessary when classifying the type of cervical deformity (discussed below) and identifying if the cervical deformity may be compensatory method for a thoracolumbar deformity. The dynamic films aid in determining the presence of any atlantoaxial instability as well as the relative flexibility of the cervical spine. With regard to standing x-rays, the EOS system is a new device that can provide single planar standing images of the patient from the skull to the feet as well as a three-dimensional (3D) configuration of the spine. 33 The benefits to this new system include: 1) the entire body can be imaged at once therefore obviating the need for taking and joining multiple x-rays, 2) the x-ray images can be re-formatted into 3D configuration with semi-automatic contouring of individual vertebra, 3) the delivered radiation dose is much lower than standard x-rays, thus reducing the dose by a factor of 10, and 4) all the points of alignment and related compensation throughout the spine are concurrently imaged. 34 Moreover, studies have shown that the EOS system is highly accurate, reproducible, and precise in the measurement of spinal curvature and that it even compares reliably to CT scanning. 35 –38 These systems are new and not every institution may have one, however they are recommended if one can be obtained. If not, the standard standing 3 foot x-rays mentioned above can work well. Rigid cervical deformities may need additional or more aggressive osteotomies to correct the deformity. Additional imaging studies are generally performed and include computed tomography (CT) and magnetic resonance imaging (MRI) to assess for osseous landmarks to plan for instrumentation insertion and spinal cord tethering or impingement, respectively. CT scans are very helpful in determining the extent of facet fusion and osteophytic bridging at the discs in order to evaluate the need for anteriorly and posteriorly osteotomies in fixed deformity.
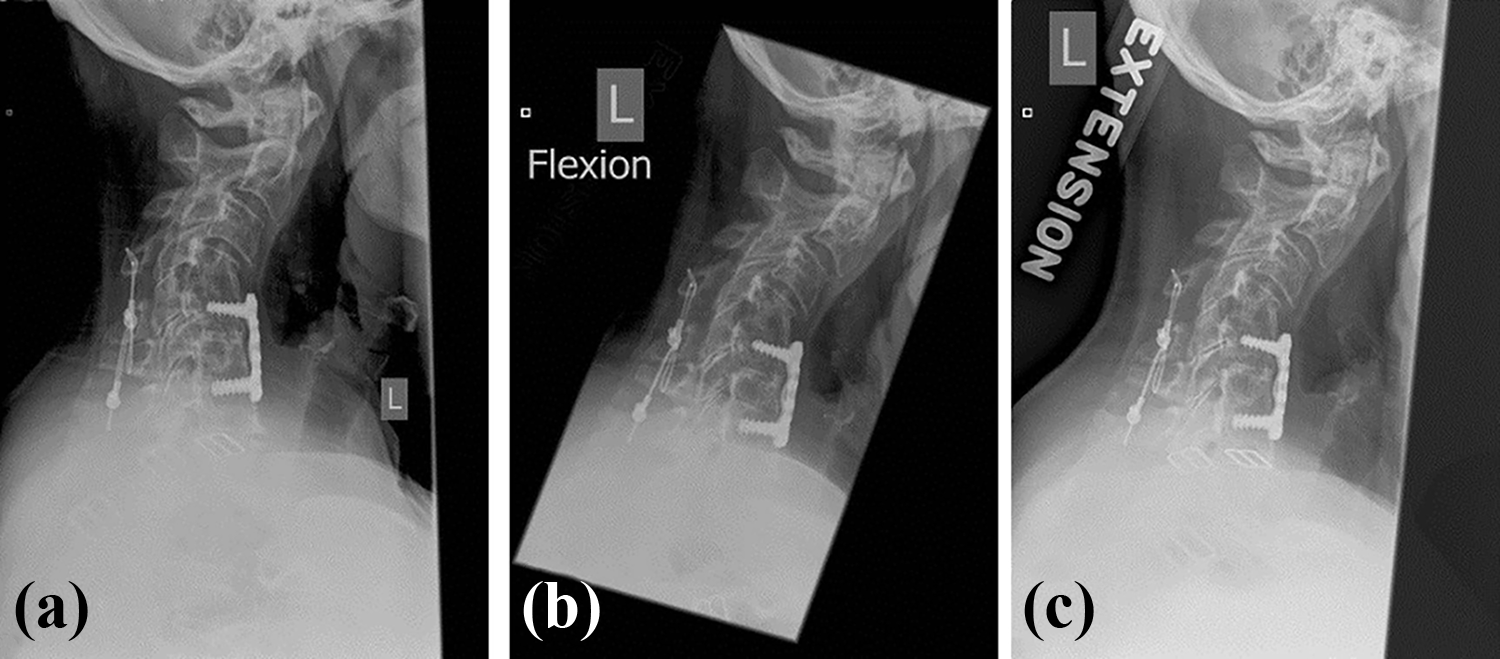
(a) Preoperative lateral radiograph of a patient with fixed cervical kyphosis. Dynamic radiographs assessing the extent of rigidity by (b) flexion and (c) extension.
Relationship of cervical deformity and myelopathy
In the context of the physical exam, one must understand the relationship between cervical deformity and myelopathy. The surgical plan may change if the patient is found to have myelopathy. Cervical deformity, especially progressive cervical kyphosis, has been associated with myelopathy even without central stenosis. This phenomenon is a result of the kyphosis leading to spinal cord being draped against the vertebral bodies. The draping causes anterior spinal cord pathology from compression against the vertebral bodies. In addition, it causes an increase in the longitudinal cord tension due to the cord being tethered by the dentate ligaments and cervical nerve roots. 39,40 (Figure 6) Tethering of the cervical cord can produce increased intramedullary pressure leading to neuronal loss and cord demyelination. 41 –43 Chronic compression of the spinal cord against the posterior aspects of the vertebral bodies results in flattening of the small feeder blood vessels on the surface of the cord become that leads to reduced blood supply and ischemia. This can lead to a large reduction in the number of vessels and network size, as well as produce an abnormal arrangement of the vessels. 44 Animal models have shown that greater cord tension increases intramedullary cord pressure 41 –43,45 and leads to neuronal apoptosis. 44 Shimizu et al. 44 analyzed the severity of demyelination and neuronal loss in spinal cord histological sections following induction of cervical kyphosis small birds. The authors discovered a significant correlation between the degree of kyphosis and the amount of cord flattening. 44 Angiography demonstrated that the vascular supply to the anterior portion of the cords was decreased. 44 Additionally, atrophy of the anterior horn, neuronal loss, as well as demyelination of the anterior fasciculus was observed. The extent of demyelination progression was directly related to a greater kyphosis angle. 44 The demyelination pattern began with the anterior fasciculus but then progressed to the lateral and posterior fasciculi. 44
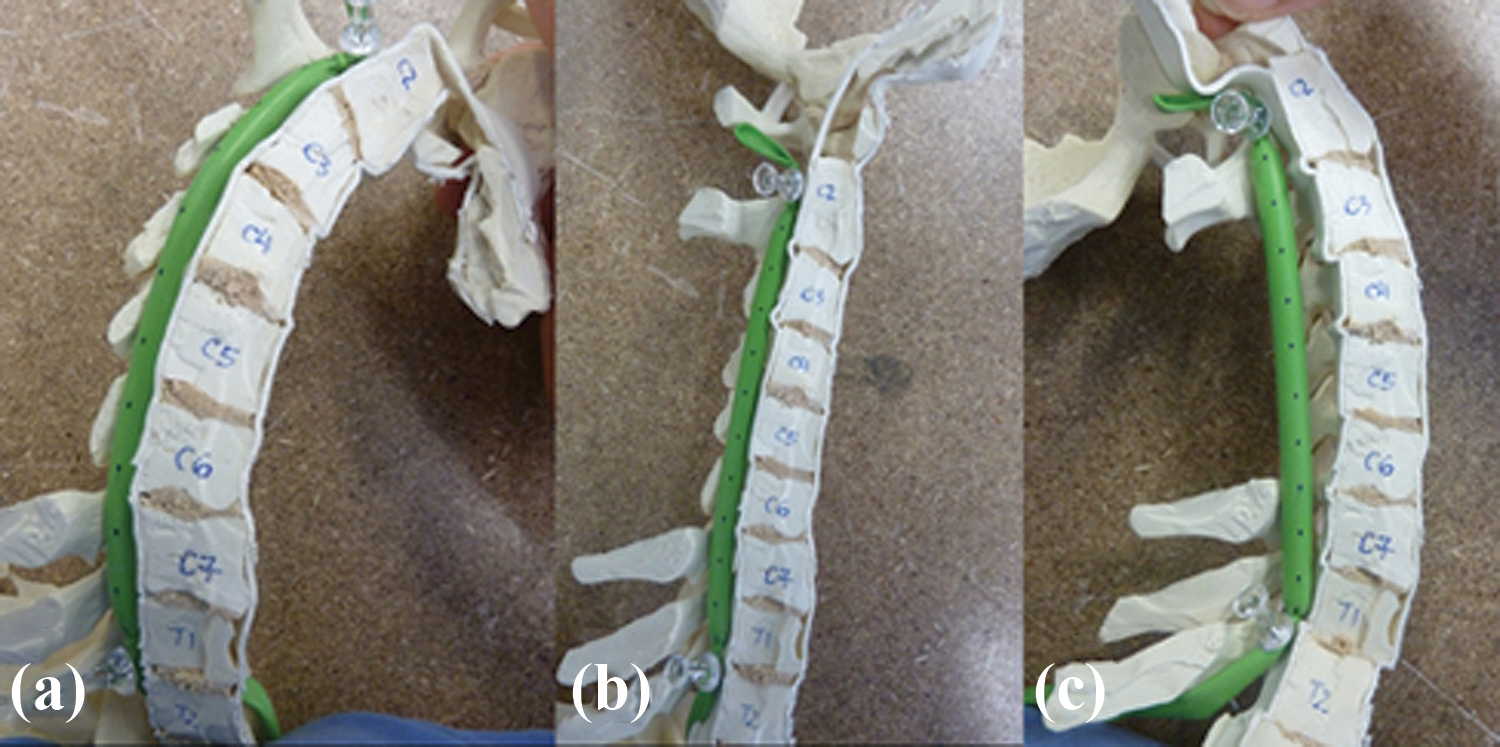
Sagittal cervical spine model showing that the spinal cord tension and length changes in response to sagittal alignment. The distance between marks (black dots) on the cord were measured and were 1.2 cm for kyphosis. Note a multilevel laminectomy has been performed to help visualize the concept. (a), 1.1 cm for the neutral position (b), and 1.0 cm for the cervical lordosis with C3–C5 laminectomy (c). Reprinted with permission from Scheer JK, Tang, JA, Smith JS, et al. Cervical spine alignment, sagittal deformity, and clinical implications: a review. J Neurosurg Spine 2013; 19(2): 141–159.
A study by Smith and collegues 46 evaluated myelopathy scores [Japanese Orthopedic Association (mJOA)] with cervical sagittal alignment and spinal cord volume in patients with myelopathy. From 56 patients, the authors found a moderate negative correlation in patients with cervical kyphosis between cord volume and cross sectional area to mJOA scores. A positive correlation was found for patients with cervical lordosis thus indicating a relationship of cord volume to myelopathy that differs on the basis of sagittal alignment. 46 Therefore, sagittal alignment can contribute substantially in the development of cervical myelopathy.
Cervical deformity classification
Not until recently did a cervical deformity classification system exist. Such as system can aid in the communication between physicians as well as assist in facilitating the appropriate clinical and radiographic evaluation of patients with cervical spine deformity. Therefore, Ames et al. 13 developed a cervical deformity classification system in order to provide a mechanism to assess cervical deformity patients within the context of global spinopelvic malalignment and clinically relevant parameters (Figure 7). The classification system consist of a primary deformity descriptor characterizing the curve apex location as well as five different modifiers. The modifiers include radiographically measured parameters and a clinical score for the degree of myelopathy. All of the five modifiers used in this classification had been previously shown to have a clinical impact. 13

Description of cervical deformity classification system, which includes a deformity descriptor and 5 modifiers. CBVA = chin-brow vertical angle, CL = cervical lordosis, mJOA = modified Japanese Orthopedic Association, T = thoracic, L = lordosis, D = double, N = none, LL= lumbar lordosis, PI = pelvic incidence.
The classification system is comprised of a deformity descriptor, three sagittal alignment parameters, a myelopathy modifier, and lastly the SRS-Schwab thoracolumbar deformity classification. The deformity descriptor was selected to provide a basic categorizing of the various deformity types. The first three types are primary sagittal deformities that are differentiated by the location of the deformity apex. Type C is for the apex in the cervical spine, Type CT for apex at the cervicothoracic junction, and Type T for apex in thoracic spine. Primary coronal deformities are those with a C2–C7 coronal Cobb angle
The three sagittal alignment parameters include cSVA, horizontal gaze (measured by CBVA), and the difference between the cervical lordosis and the T1 slope. The cSVA was selected as a modifier for the CSD classification given the significant impact of sagittal alignment on HRQOL among patients with thoracolumbar spinal deformities and the studies of Tang et al. 6 and Smith et al. 46 demonstrating correlations between cervical sagittal alignment and multiple measures of HRQOL. Tang et al found that a C2–C7 SVA threshold of 4 cm was found to correlate with moderate disability based on the Neck Disability Index (NDI). 6 Therefore, there are three scores for the C2–C7 SVA modifier focused around the 4 cm threshold (Figure 7). Because horizontal gaze has a fundamental impact on basic human function and previous reports demonstrating the importance of accounting for horizontal gaze in spine deformity surgery, 14,24 –29,47 the CBVA was selected as a modifier for the classification system. Although thresholds of normal CBVA have not yet been rigorously defined, a CBVA of 10° is accepted as an optimal value. 14 Therefore three scores were selected for the horizontal gaze modifier (Figure 7). The relationship between T1 slope and cervical lordosis is similar to the relationship between PI and LL in that a greater T1 slope requires a greater magnitude of cervical lordosis to balance the head over the thoracic inlet and trunk. 14,48 And given that cervical kyphosis is the most common type of cervical deformity with studies showing the clinical impact of this kyphosis, a parameter reflective of cervical lordosis was added as a modifier for the classification. The mismatch between T1 slope and cervical lordosis (TS-CL) was added with three scores (Figure 7).
As mentioned above, the clinical importance of cervical myelopathy is well known and its relationship to cervical alignment is critical to evaluating cervical deformity patients. Having myelopathy may affect the surgical plan in deformity patients as it should address spinal cord compromise when present, which may be through direct decompression, deformity correction, or both. Thus a measure of myelopathy was included in the CSD classification since myelopathy can be directly related to cervical deformity and since it can profoundly impact patient function. The mJOA score is a recognized and a widely accepted quantitative functional assessment of the severity of spondylotic myelopathy severity. 49 Scores range from 0 to 18, with lower scores reflecting worse impact and three groups of scores were added to the classification (Figure 7).
And finally, the SRS-Schwab modifier was added because the spinal segments are all related and are not insolation of one another. Cervical deformities may contribute to thoracolumbar deformities and thoracolumbar deformities may produce or contribute to cervical deformities. 14 Smith et al demonstrated that adults with positive sagittal spinopelvic malalignment compensate with increased cervical lordosis in an effort to maintain horizontal gaze and that surgical correction of the thoracolumbar sagittal malalignment results in improvement of the abnormal cervical hyperlordosis through reciprocal changes. 50 Ha and colleagues subsequently confirmed this observation and further identified key radiographic parameters associated with these compensatory changes. 51 The authors studied 49 patients that underwent surgical correction for thoracolumbar deformity and measured the cervical lordosis for a high and low preoperative C7 SVA groups. 51 In the lower C7 SVA group, cervical lordosis was significantly increased after thoracic/lumbar deformity correction and the high C7 SVA group showed decreased cervical lordosis postoperatively. 51 Furthermore, a high prevalence of concomitant cervical deformity has been reported among adults with thoracolumbar deformity. 52 Therefore, based on these and other studies that emphasize that assessment and classification of cervical deformity should not occur in isolation and that alignment of the thoracolumbar spine and pelvis should also be assessed. Therefore SRS-Schwab classification for adult thoracolumbar spinal deformity was added as a modifier for the cervical deformity classification. The SRS-Schwab classification includes five thoracolumbar coronal curve types and three sagittal modifiers (Figure 8). The SRS-Schwab classification has been validated, shown to correlate with HRQOL measures at baseline, and shown to be sensitive to changes in disease state. 53 –55

SRS-Schwab classification system for adult spinal deformity. The classification consists of four coronal curve types and four sagittal modifiers. PI = pelvic incidence; LL = lumbar lordosis; SVA = sagittal vertical axis; PT = pelvic tilt; T = thoracic; TL = thoracolumbar.
Treatment indications
Nonoperative management
Surgery should not be the first line of treatment and the patient may attempt a number of conservative options. Conservative treatment of cervical spinal deformity is mostly aimed at symptom reduction and the majority of cases that is addressing neck pain. Other options include chiropractic care and/or physical therapy, steroid injections, brace therapy, cervical traction, and nonsteroidal anti-inflammatory drugs (NSAIDs). Surgical treatment indications include patients with severe mechanical neck pain, any neurological deficit, and progressive deformity resulting in significant disability (i.e. loss of horizontal gaze and/or dysphagia).
Patients presenting with head ptosis or neck drop (cervical camptocormia) have a flexible sagittal deformity of the cervical spine which is corrected when the patient is laying supine. 56 The various etiologies of camptocormia include various myopathies, parkinsonism disorders, amyotrophic lateral sclerosis (ALS), and idiopathic. 56 Therefore, the initial work up of a patient with camptocormia (or other flexible deformity) should include appropriate electromyography, nerve conduction studies and referral to a Neurologist to rule out a primary myopathy or ALS. Moreover, they should be referred to physical therapy prior to considering treating with surgical correction and fusion.
Surgical management
When considering a surgical intervention, evaluation of the flexibility and rigidity of the cervical spine may determine the type of surgery needed. For a cervical spine that is flexible and is without ankyloses based on clinical exam, flexion/extension x-rays, and CT, an anterior or posterior alone correction strategy may be used. However, if the spine is rigid without ankylosed facets or have prior instrumentation, an anterior alone strategy may be sufficient. A combination of anterior and posterior approaches may be required to correct a deformity that is rigid in the anterior column and has ankylosed facets. The surgical approach, osteotomy type, and correction strategy also depends on the cervical deformity type being treated. In general, anterior release and posterior fixation is often most effective for subaxial cervical sagittal deformities (cervical kyphosis). For patients with cervical deformity as a result of CTJ pathology (high T1-slope, neutral to normal CL, and high low C2-slope), a three-column osteotomy and posterior approach would be the correct strategy to use.
Cervical traction with a halo may be used to initially attempt deformity correction prior to surgical intervention. Typically, 3–5 days of traction may be sufficient to reduce the deformity. 32 There is no current standard for the amount of weight to add, however, starting with 4 kg and adding 1 kg per day up to 9 kg has been described. 57 If the deformity is not reduced after day 5, further traction is not likely to be of any benefit. In addition to the traction, once can add various muscle relaxing agents to aid in the deformity reduction. If successful reduction of the cervical deformity does occur, posterior fixation and fusion may be used to prevent the deformity from progressing.
When able to use the anterior alone approach, this allows for deformity correction via interbody release as well as instrumentation that maintains the correction. This method uses both biomechanics and posture to obtain the targeted postoperative cervical alignment. The patient is placed in the supine position with their head extended. In almost all cases, cervical traction is utilized with Gardner well tongs with 15 to 20 lbs. of weight (depending on patient size and deformity). After adequate exposure, anterior release may be performed by a combination of the osteotomy grades listed below. They generally include releasing the disc, osteophytes and uncovertebral joints. But may include corpectomies if indicated.
When the cervical deformity is rigid with ankylosed facets, a combined anterior-posterior strategy may be employed. 58 With modern instrumentation and technology, a 360-degree approach is often sufficient to gain adequate correction. However a 540-degree approach can be utilized in uncommon circumstances. In this scenario, the side of deformity correction is first chosen for release and then the opposite side is released. Generally, the posterior approach is performed first with placement of screws and various osteotomies performed. The patient is then turned to the supine position for the anterior approach that includes disc release, anterior osteotomy and lordotic plating. The patient is then turned again to the prone position and instrumentation and posterior compression is applied. For significant fixed subaxial kyphosis it is recommended to first perform an anterior osteotomy (including release of the vertebral arteries from the foramen transversarium) then followed by posterior osteotomies with correction using head manipulation after the circumferential release. In patients requiring significant deformity correction, it is strongly recommended to use the halo ring instead of the Mayfield clamp. The halo has more fixation points and allows a stronger grip on the patient’s head during manual correction resulting in a lower chance of it slipping off the patient. Usually more lordosis is possible during an anterior release followed by posterior correction compared with the converse of posterior release followed by an anterior fixation. This is because it is typically easier to generate more lordosis from the posterior position. If the cervical deformity is very kyphotic and rigid with ankylosed facets, larger osteotomies or a combination of different osteotomies may be necessary to correct the deformity.
Cervical deformities in the coronal plane may be isolated or in combination with sagittal deformities with varying degrees of severity. Patients with fixed multiplanar deformities may require three-column osteotomies in order to allow for correction of the spine in both planes as well as to decompress the spinal cord and nerves. In addition, these patients may need multiple combined approached and/or stages. A 540 degree circumferential osteotomy or possibly a cervical vertebral column resection (VCR) may be used. 59
With the evolution of cervical deformity types and the surgical treatment becoming more complex, a cervical osteotomy classification was developed by Ames et al. 16 (Table 1 and Figure 9). This system is focused on being anatomically based, graduated in degree of resection, and comprehensive. 16 It’s not designed to describe surgical indications for correction but more to aid in determining the optimal surgical approaches and osteotomies used. Moreover, it allows for a common language to more effectively and objectively communicate cervical osteotomy resections between surgeons and in the literature when describing techniques or research. In the classification system, there are seven anatomical grades of resection that increase in amount of tissue resection and degree of spine destabilization (Table 1 and Figure 9). Furthermore, since surgical correction of complex deformities may involve combinations of resection types, modifiers are included in the system to designate the surgical approach(es) that may be used in conjunction with the osteotomy grade. These include anterior [A], posterior [P], anterior-posterior [AP], posterior-anterior [PA], anterior-posterior-anterior [APA], and posterior-anterior-posterior [PAP] are listed in Table 1.
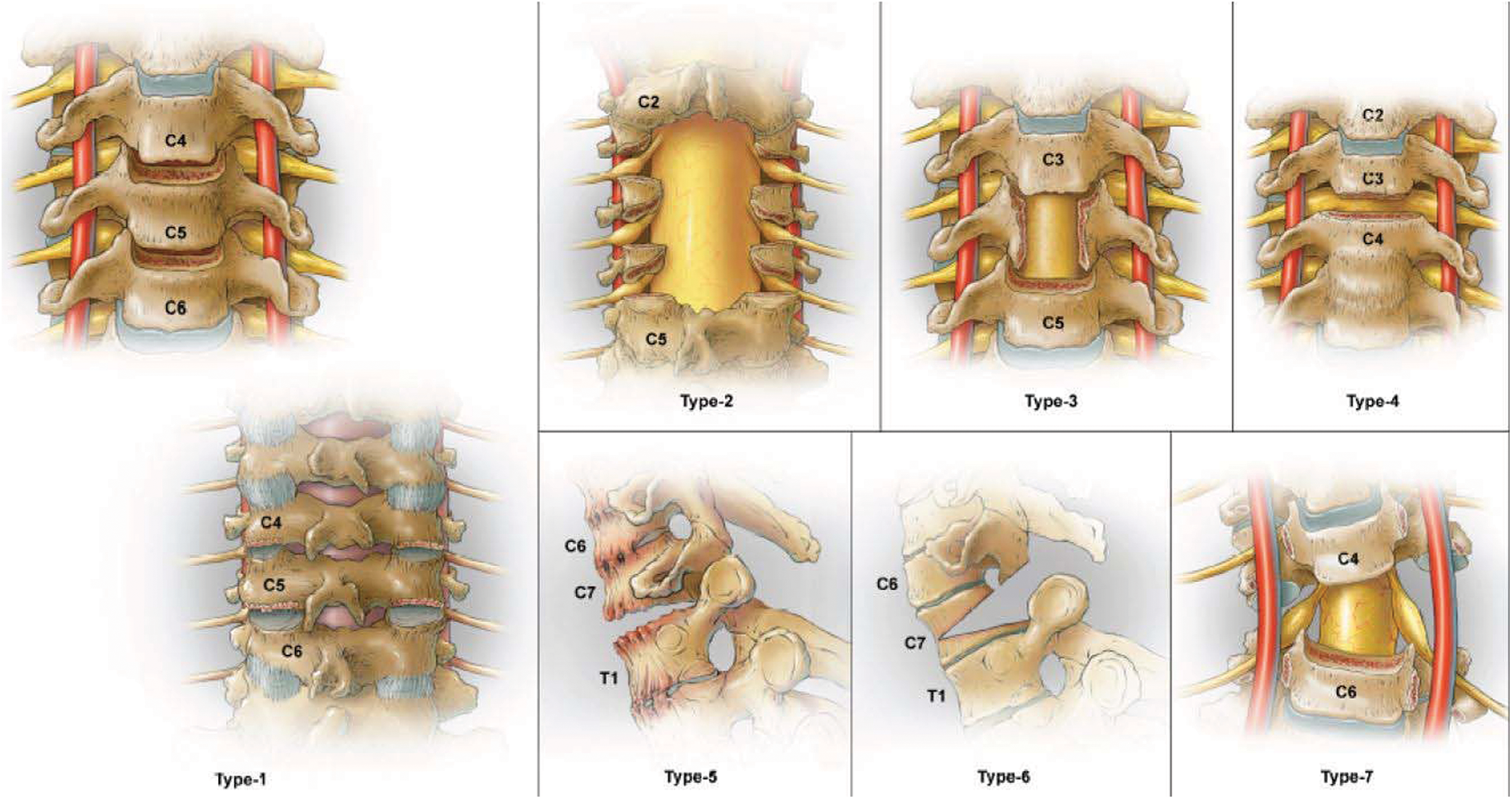
Illustrations depicting the cervical osteotomy classification system, which includes seven grades of resection, representing progressive degrees of potential destabilization. Reprinted with permission from Ames CP, Smith JS, Eastlack R, et al. Reliability assessment of a novel cervical spine deformity classification system. J Neurosurg Spine 2015; 23(6): 673-683
Description of cervical osteotomy classification system developed by Ames et al. 16

* A = anterior, P = posterior, AP = anterior-posterior, PA = posterior-anterior, APA = anterior-posterior-anterior, PAP = posterior-anterior-posterior.
Surgical complications
The surgical correction of cervical spinal deformity is very complex and associated with a high complication rate. 60,61 A study by Passias and colleagues identified a 39.9% intraoperative complication rate. 60 The authors further stratified the complications by types and reported that the neurological complication rate was 13.9%, dysphagia/respiratory was 9.8%/8.2%, infection was 8.2%, and dural tear was 4.1%. 60 Another study investigating complication rates in cervical deformity correction was conducted by Smith et al. 61 in which they found an overall complication rate of 43.6%. The most common complications were dysphagia (11.5%), deep wound infection (6.4%), new C5 motor deficit (6.4%), and respiratory failure (5.1%). And finally, another study by Smith and colleagues evaluated all-cause mortality following surgical correction of adult cervical spinal deformity and found that the 1.2 year postoperative all-cause mortality was 9.2%. 61 Given that these complication rates are high, it is very important that potential surgical risks of undergoing a cervical deformity correction are discussed with the patient and an appropriate plan is developed. For patients that require a three-column osteotomy for deformity correction, they should be especially counseled as a recent study by Smith et al. found these patients had a 56.5% overall complication rate with neurological deficit of 17.4% being the most common. The C5 palsy was most common with Smith-Petersen osteotomies (SPOs) and C8 was most common with three-column osteotomies.
Postoperative distal junctional kyphosis (DJK) in patients undergoing cervical deformity correction is of growing concern. DJK has been defined as a loss of radiographic alignment at one or two levels distal to the lower-most instrumented vertebra (LIV) and is associated with adjacent level failure, instrumentation failure, and spondylolisthesis. 62 A study by Passias and colleagues demonstrated a 1-yeay postoperative rate of 23.1% for DJK. 62 DJK occurred most commonly at 3 months postoperative and patients with DJK had significantly more severe cervical malalignment at baseline, as measured by T1S-CL, CL, cSVA, C2-T3 angle, and C2 slope. 62
Since DJK is a critical complication of cervical deformity correction, there are a few DJK prevention methods that include the use of medications to strengthen bone density such as teriparatide, appropriate selection of the LIV in relation to the curve apex, and ligament augmentation. 63 In proximal junctional kyphosis (PJK), ligament augmentation has been shown to significantly reduce the rates of postoperative PJK. 63 In a study by Safaee et al. in which the authors performed a multivariable model, ligament augmentation was significantly associated with being protective against PJK. 63 This method of ligament augmentation could be applied to DJK in the cervical spine. Furthermore, the location of the LIV relative the deformity curve apex is crucial in preventing DJK. The LIV should be below the thoracic apex (i.e.T9 or T10) if the cSVA is 4 cm or greater, the T1 slope is greater than 30 degrees, the global SVA is greater than 8 cm and for any patients undergoing a three-column osteotomy. For these instances, the risk of DJK is higher if the LIV is near or above the thoracic apex. There are many factors involved when deciding a surgical plan for cervical deformity correction and any attempt to minimize risk to the patient should be pursued. Future directions include risk stratification predictive models and artificial intelligence that may aid in surgical planning and shared decision making with the patients.
Summary
A review of cervical sagittal balance has been presented and includes key radiographic, clinical evaluation techniques and surgical decision making pearls to aid in treating this complex population of patients. A thorough understanding of the primary cervical radiographic alignment parameters and their relation in cervical deformity evaluation are critical in treating cervical deformity patients. In addition, one must consider global spinal alignment as the cervical spine is influenced by the thoracolumbar and pelvic segments. As mentioned, the T1 slope and the thoracic inlet angle, as they relate to cervical lordosis, are important parameters to consider in optimizing cervical deformity correction. 61 In addition, the importance of the CBVA has been well established and must be considered in preoperative planning strategies. 24 –29
Once can’t evaluate a patient with cervical deformity and not consider myelopathy as the cervical deformity can contribute to myelopathy and that deformity correction can treat it. Studies have shown that as the spinal cord is draped over the vertebral bodies in cervical kyphosis, there is a lack of blood flow and neuronal loss. Thus the future direction of cervical deformity correction and myelopathy treatment should involve a comprehensive approach in assessing global cervical-spinal-pelvic relationships.
There are several key concepts to understand when clinically evaluating a patient with cervical deformity. A thorough history and physical exam (including neurological exam) must be completed. The patient must be evaluated in a standing and sitting/supine positions to help evaluate whether the deformity is rigid or flexible. Appropriate imaging must also be performed and should include 3 foot standing x-rays and CT scans for surgical planning. And lastly, patients that have a flexible cervical deformity found on supine testing must be ruled out for any of the various etiologies of camptocormia including different myopathies, amyotrophic lateral sclerosis (ALS), parkinsonism disorders, and idiopathic. The initial work up a patient with camptocormia (or other flexible deformity) should include appropriate electromyography and nerve conduction studies to rule out a primary myopathy or ALS.
To help with cervical deformity diagnosis and thus treatment, both a comprehensive and validated cervical deformity classification system has been developed as well as an osteotomy classification system. The deformity classification system provides a common nomenclature to discuss different cervical deformities and can aid in surgical planning. The cervical osteotomy classification system is based on seven resection grades in increasing levels of destabilization. In addition an approach modifier is provided that allows the surgeon to have a simple, standard description of cervical osteotomies as a means of improving communication, treatment, and research efforts.
And lastly, the complication rates for surgical cervical deformity correction is very high and all means to reduce the rate and discuss these risks with the patient must be observed. Neurological complications are the most common with dysphagia/respiratory and wound infections being next. It is important to note the high 1 year postoperative all-cause mortality at of 9.2%. However this was mostly accounted for the patients’ comorbidities. Using bone modifying agents to improve bone density and ligament augmentation may help with prevention of the high DJK rate of 23%. Future work will better develop predictive models using machine learning and artificial intelligence to aid in surgical planning and informed consent.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.