
Abstract
Study design:
Retrospective longitudinal cohort study.
Objective:
To investigate postoperative medical complications in patients with malnutrition after cervical posterior surgery.
Methods:
A total of 256 patients were participated and divided into PNI < 50 group (group L) or PNI ≥ 50 (group H). Patient data, preoperative laboratory data, surgical data, hospitalization data, JOA score, complication data were measured.
Results:
Group L and group H were 127 and 129 patients, each PNI was L: 44.8 ± 4.3, H: 54.6 ± 4.0, P < 0.01. There was significant difference in mean age (L: 72.2 years vs H: 64.8 years, P < 0.01), BMI (23.1 vs 24.7, P < 0.01), serum albumin (L: 3.9 ± 0.4 g/dl vs H: 4.4 ± 0.3 g/dl, P < 0.01), total lymphocyte count (L: 1.3 ± 0.5 103/µL vs H: 2.1 ± 0.7 103/μL, P < 0.01), hospital stay (L: 25.0 days vs H: 18.8 days, P < 0.05), discharge to home (87.5% vs 57.5%, P < 0.01), delirium (L: 15.9% vs H: 3.9%, P < 0.01), medical complications (L: 25.2% vs H: 7.0%, P < 0.01), pre- and post- operative JOA score (L: 11.3 ± 2.8 vs H: 12.4 ± 2.6, P < 0.01; L: 13.3 ± 3.0 vs H: 14.1 ± 2.4, P = 0.02). Multiple logistic regression analysis showed that significant risk factors for medical complications were PNI<50 (P = 0.024, odds ratio [OR] 2.746, 95% confidence interval [CI] 1.143–6.600) and age (P = 0.005, odds ratio [OR] 1.064, 95% confidence interval [CI] 1.020–1.111).
Conclusion:
Medical complications are significantly higher in patients with PNI < 50 and higher age. The results showed that PNI is a good indicator for perioperative medical complications in cervical posterior surgery. Improvement of preoperative nutritional status is important to avoid medical complications.
Level of evidence:
3
Keywords
Introduction
Several countries are facing the problem of an aging society, and Japan is known as a super-aging country. The increase in the elderly population increases the prevalence of degenerative diseases (such as osteoarthritis, spinal deformities, and spondylotic diseases). Consequently, operations performed on elderly patients have also increased. 1 However, these operations are often challenging due to the severe symptoms, comorbidities, and poor nutritional status of most elderly patients. Identifying and reducing the risks of surgery for elderly patients surgery is important for the medical economy.
Complications for cervical posterior surgery have been reported to included wound complications, 2 –4 neck axial pain 5 and delirium. 6 –9 The postoperative complication rate of cervical posterior surgery is reported to be about 15%. 10 –12 Therefore, we have to pay attention to reduce the complication rate by even a small amount.
Onodera et al. 13 reported prognostic nutritional index (PNI easily calculate nutritional status from serum albumin levels and total lymphocyte count). PNI was calculated as a prognostic predictor for terminal-stage digestive system cancer patients, but was later expanded to predict surgical indications. In recent years, the importance of preoperative nutritional status has been noted in the field of orthopedics. Oe et al. 14,15 reported a relationship between malnutrition and spinal surgical outcomes. Patients with delirium after adult spinal deformity (ASD) surgery had significantly lower PNIs compared to patients who did not have delirium. Among patients who underwent ASD surgery, 41.4% had a PNI < 50 and medical complication rates were found to be significantly higher in patients who underwent ASD surgery with a PNI < 50. 15 However, the effect of malnutrition on patients undergoing cervical posterior surgery is unknown.
The aim of this study was to investigate the perioperative medical complications of patients with malnutrition who underwent cervical posterior surgery.
Materials and methods
Patients and study design
We retrospectively enrolled 289 patients who underwent cervical posterior decompression surgery at 12 participating hospitals between August 2010 and July 2019. The inclusion criteria were cervical posterior decompression surgery including laminoplasty and laminectomy without any instrumentation. In almost all laminoplasty, double door laminoplasty was performed, and there was no big difference between facilities in terms of years of experience and skill of the surgeon. Patients for whom PNI data was not available or who were followed up for less than 1 year were excluded from the study. However, patients who had medical complications or died within 1 year postoperatively were included in this study. The patients were divided into two groups based on their PNI. Patients with a PNI < 50 were in group L and those with a PNI ≥ 50 were in group H. We recorded the patients’ age, sex, body mass index (BMI; kg/m2), smoking history (current or not), alcohol history (current or not), blood sampling data(was evaluated within 3 months prior to surgery): serum albumin (g/dL), total cholesterol (mg/dl), hemoglobin (g/dl), white blood cell count (/μL), lymphocyte count (/μL), estimated blood loss (ml), operative time (minutes), number of decompressed vertebrae, PNI (calculated as PNI = 10 × serum albumin (g/dl) + 0.005 × total lymphocyte count (/μL)), days to ambulation (days), days to discharge (days), discharge to home ratio, and medical complications (excluding surgical complications such as hematoma) within 30 days postoperatively. Surgical site infections (SSIs) and mortality were up to 1 year after the surgery. Neurologic dysfunction was assessed using the JOA score. The preoperative JOA score was assessed within 1 month prior to surgery and the postoperative JOA score was assessed at 1 year postoperatively. Recovery rate (RR, %) 16 was calculated as follows: RR = (postoperative JOA − preoperative JOA)/(17 − preoperative JOA).
The study protocol was approved by the institutional review board of Hamamatsu University School of Medicine, Shizuoka, Japan. IRB number is 19-242.
Statistical analysis
Unpaired t-tests were used to compare data between the groups and multiple logistic regression analyses were performed to identify the risk factors for medical complications. The dependent variables were set as the presence or absence of postoperative medical complications. Independent variables were set as below; age, BMI, PNI < 50. All statistical analyses were performed using SPSS version 26 statistical software package (IBM-SPSS, Inc., Chicago, IL, USA). Statistical significance was set at P < 0.05.
Results
Patient characteristics
As shown in Figure 1, 33 patients met the exclusion criteria: 33 were not to get PNI data.
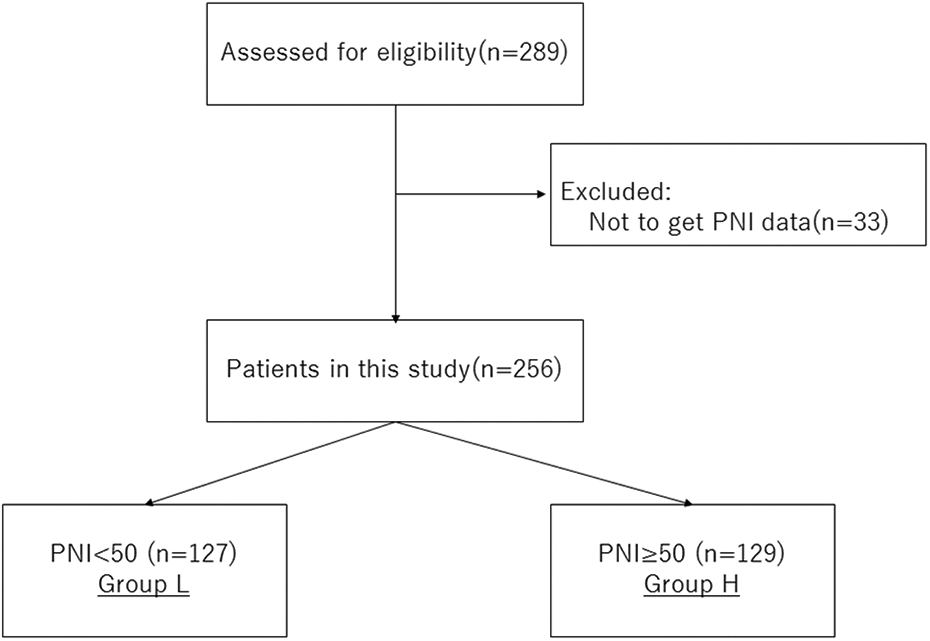
Flowchart of consecutive patients who underwent posterior cervical surgery. The excluded patients were 33 patients with no PNI data. A total of 256 patients (L group = 127 patients and H group = 129 patients) were recruited in this study.
A total of 256 patients were eligible for inclusion, 127 in group L and 129 patients in group H. There was a significant difference in age between both groups (L: 72.2 ± 10.5 years vs H: 64.8 ± 11.4 years, P < 0.01) and BMI (23.1 kg/m2 vs 24.7 kg/m2, P < 0.01), respectively, Table 1.
Baseline characteristics of patients.

Mean values are presented as mean ± SD. *Comparison among groups. BMI, body mass index.
We defined Smoking history that smoked until recently and Alcohol history that drank until recently.
There was no significant difference in male (L: 66.9% vs H: 76.7%), smoking history (L: 14.4% vs H: 20.2%), alcohol history (L: 33.0% vs H: 38.9%), respectively.
Preoperative laboratory data
There was a significant difference in serum albumin(L: 3.9 ± 0.4 g/dl vs H: 4.4 ± 0.3 g/dl, P < 0.01), total cholesterol (L: 182.9 ± 42.0 mg/dl vs H: 202.8 ± 41.4 mg/dl, P < 0.01), hemoglobin (L: 12.9 ± 1.9 g/dl vs H: 14.4 ± 1.4 g/dl, P < 0.01), white blood cell (L: 6.1 ± 2.0 103/µL vs H: 6.7 ± 1.4 103/μL, P < 0.01), total lymphocyte count (L: 1.3 ± 0.5 103/µL vs H: 2.1 ± 0.7 103/μL, P < 0.01) and PNI (L: 44.8 ± 4.3 vs H: 54.6 ± 4.0, P < 0.01), respectively, Table 2. On the other hand, no significant differences was found in the number of vertebrae decompressed (L: 4.3 ± 0.8 vs H: 4.2 ± 0.7), estimated blood loss between both groups (L: 83.7 ± 87.8 ml vs H: 89.3 ± 118.1 ml) and operative time (L: 127.6 ± 47.2 min vs H: 119.6 ± 47.5 min).
Preoperative laboratory and surgical data.

Mean values are presented as mean ± SD. *Comparison among groups. PNI, prognostic nutritional index.
Operative outcomes and hospitalization data
There was a significant difference in hospital stay (L: 25.0 ± 14.8 days vs H: 18.8 ± 12.0 days, P < 0.01) and discharge to home ratio (discharge to home, L: 73 (57.4%) vs H: 113 (87.5%), P < 0.01) between both groups, respectively, Table 3.
Operative outcome and hospitalization data.

Mean values are presented as mean ± SD. *Comparison among groups.
There was a significant difference in delirium (L: 20 (15.9%) vs H: 5 (3.9%), P < 0.01) and medical complication (L: 32 (25.2%) vs H: 9 (7.0%), P < 0.01) between both groups, respectively. On the other hand, no significant differences was found in SSI (L: 9 (7.1%) vs H: 4 (3.1%), P = 0.15), Table 3.
The medical complications for patients in each group are listed in Table 4. Medical complications in this study include: delirium 25 cases, SSI 13 cases, urinary tract infection (UTI) 5 cases, pneumonia 4 cases, renal disorder 1 case, deep venous thrombosis(DVT) 1 case, hypoglycemia 1 case, angina 1 case, cerebral infarction 1 case, sinus bradycardia 1 case and death 1case (there was duplication). L group: delirium 20 cases (15.7%), SSI 9 cases (7.1%), UTI 5 cases (3.9%), pneumonia 4 cases (3.1%), renal disorder 1 case (0.8%), DVT 1 case (0.8%), hypoglycemia 1 case (0.8%), angina 1 case (0.8%), cerebral infarction 1 case (0.8%), sinus bradycardia 1 case (0.8%) and death 1case (0.8%). H group: delirium 5 cases (3.9%) and SSI 4 cases (3.1%). Many kinds of complications were observed in group L compared with group H. In addition, in group L, there were many complications related to infection such as SSI, pneumonia, and urinary tract infection.
Medical complication.

Number (%), each articles. SSI, surgical site infection.
There was a significant difference in hospital stay (L: 25.0 ± 14.8 days vs H: 18.8 ± 12.0 days, P < 0.01) and discharge to home ratio (discharge to home, L: 73 (57.4%) vs H: 113 (87.5%), P < 0.01) between both groups, respectively, Table 3.
Neurological data
There was a significant difference between the groups in both preoperative JOA scores (L: 11.3 ± 2.8 vs H: 12.4 ± 2.6, P < 0.01) and postoperative JOA scores (L: 13.3 ± 3.0 vs H: 14.1 ± 2.4, P = 0.02). On the other hand, no significant differences was found in RR (L: 29.6% vs H: 37.5%, P = 0.73), Table 5.
Neurological data.
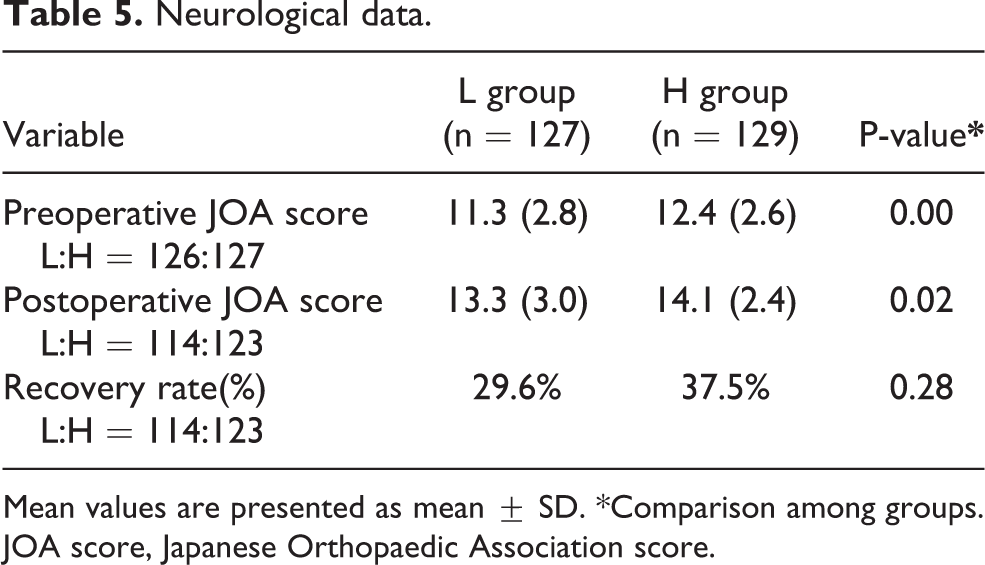
Mean values are presented as mean ± SD. *Comparison among groups. JOA score, Japanese Orthopaedic Association score.
The significant risk factors of medical complications were identified using multiple logistic regression analysis. The dependent variables were set as presence or absence of postoperative medical complications. Independent variables were set as below; age, BMI, PNI < 50. As a result, risk factors for incidence of medical complications were PNI < 50 (odds ratio [OR]: 2.745; 95% confidence interval [CI]: 1.196–6.302; P = 0.017) and age (OR: 1.068: 95% CI: 1.025–1.114; P = 0.002).
Discussion
This is the first study in the world to examine the effect of PNI on the complications of cervical posterior decompression surgery.
In this study, we intended only cervical posterior decompression surgery. A posterior approach for cervical spine surgery is often performed in Japan due to the lower incidence of fatal complications than the anterior approach and the less challenging decompressions for multiple stenoses. 17 Elderly patients are more likely to have complications during cervical spine surgery, and it is important to perform surgery safely and reduce the rate of complications.
Tables 1 and 2 show that group L had a lower BMI, serum albumin, total cholesterol, white blood cell count, and total lymphocyte count than group H. The BMI, serum albumin, total cholesterol, and total lymphocyte count are used as malnutrition markers. 18 Therefore, our results support the theory that PNI is good predictor of nutritional status.
Table 2 shows that estimated blood loss, operative time, and the number of decompressed vertebrae were almost equal for each group, indicating that the operative stress was also equal between the groups. However, Table 3 shows there were significant differences in the groups’ operative outcomes. Delirium 19 and medical complications 20 are known to be related to high operative stress, and the results of this study suggest that delirium and medical complications are also affected by the nutritional status of the patients. Previous study reported almost same results. Oe et al. 14,15 reported that a PNI < 50 was a risk factor for delirium and medical complications in patients undergoing ASD surgery. Delirium and medical complications result in longer hospital stays and fewer patients discharged to home. In this study, the cutoff value was 48.43 (sensitivity 0.694, specificity 0.700) in the ROC analysis complications as were used as the PNI as dependent variable and the independent variable. So it was appropriate that PNI < 50 was set as the standard for grouping.
In this study, there were no significant differences in SSI. Previous studies 19 –25 have reported that malnutrition status impacts SSI. Christou et al. 26 reported that host defense (delayed-type hypersensitivity), acute and chronic physiologic derangement (measured by serum albumin and age), and bacterial contamination (contamination status and duration of surgery) are all risk factors for SSI after general surgery. Therefore, PNI is one of several factors affecting the rate of SSIs. We found that patients in group L were more likely to experience an SSI, urinary tract infection (UTI), or pneumonia, which indicates that the improvement of the nutritional status may lead to a reduction in the rate of these medical complications.
Table 5 shows that both the preoperative and postoperative JOA scores were significantly lower in group L than in group H. However, group L also had a higher mean age, which may play a role in the worsened neurological findings of this group. In addition, disease duration was not considered in this study and should be considered in future studies. We also found no significant difference in the RR of the two groups. More research is required to determine the relationship between nutritional status and RR.
The total body albumin content is 4–5 g/kg, of which one third is in the intravascular space and two thirds is in the extravascular compartment. Albumin is made in the liver and has a half-life of 2–3 weeks. 27 Patients with hypoalbuminemia have depleted their extravascular albumin, and it is challenging for these patients to restock their intravascular albumin acutely. Nishida et al. 28 reported that the use of Nutritional Support Team (NST) interventions increased serum albumin levels in patients with low nutritional states after 3 months. Bin et al. 29 reported that multimodal nutritional management (MNM) protocols effectively reduced the need for albumin infusions and increased the postoperative levels of albumin. The MNM protocols included the administration of nutrition powder beginning on the day prior to surgery, and the reduction of the period for eating and drinking as much as possible. With this protocol, the serum albumin level on the third day after surgery could be maintained significantly. It is important that albumin levels are maintained before and after surgery.
There were several limitations to our study: (1) We did not include the past medical history and comorbidities of the patients, which may affect the results as there was a significant difference in age between the two groups. Furthermore, age may be a confounding factor in this study, as age and PNI are related to some extent. (2) We investigated the PNI, serum albumin, total cholesterol, hemoglobin, white blood cell count, and total lymphocyte count, but we did not include transferrin or prealbumin in our analyses, which have been reported as good indicators of poor nutrition in a previous study. 30 In the future, we will increase the number of items to be examined and conduct research. (3) Lastly, the sample size of this study was too small to evaluate postoperative medical complications, especially SSI. The number of cases of SSI was small. Larger studies that include more variables are necessary.
Conclusions
Malnutritional status (PNI < 50) results in longer hospital stays, a lower discharge to home ratio, more delirium, and more medical complications in patients undergoing cervical posterior surgery. A nutritional assessment should be done prior to surgery, and nutritional therapy should be administered for several months if the PNI is less than 50 to avoid complications. Further research is needed to determine the specific nutritional therapy needs for elderly patients and patients with impaired hepatic or renal function.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.