
Abstract
Objectives
Osteoporotic vertebral compression fractures (OVCF) are a common increasing entity in elderly patients and represent a tremendous economic burden. Surgical treatment is related to high complication rates and little is known about patient-specific and internal risk factors associated with poor clinical results.
Methods
We carried out a comprehensive, systematic literature search according to the PRISMA checklist and algorithm. Risk factors for perioperative complications, for early inpatient readmission, for the duration of the hospital stay, the hospital mortality, the total mortality and the clinical result were analyzed.
Results
A total of 739 potentially usable studies were identified. After considering all inclusion and exclusion criteria, 15 studies with 15,515 patients were included. Non-adjustable risk factors were age >90 years (OR 3.27), male gender (OR 1.41), BMI less than 18.5 kg/m2 (OR 3.97), ASA score >3 (OR 2.7), activity of daily live (ADL) (OR 1.52), dependence (OR 5.68), inpatient admission status (OR 3.22), Parkinson disease (OR 3.63) and disseminated cancer (OR 2.98). Adjustable factors were insufficient kidney function (GFR <60 mL/min, and Creatinine Clearance below 60 mg/dl) (OR 4.4), nutrition status (hypalbuminemia (<3.5 g/dl)), liver function (OR 8.9) and further cardiac and pulmonary comorbidities.
Discussion
We identified a couple of non-adjustable risk factors, which should be considered preoperatively in terms of risk assessment. However, even more important were adjustable factors that can be influenced preoperatively. In conclusion, we recommend a perioperative interdisciplinary cooperation, especially with geriatricians, to achieve the best possible clinical results in geriatric patients undergoing surgery for OVCF.
Keywords
Objectives
Up to 400.000 vertebral fractures are diagnosed in Europe every year, with elderly patients being particularly affected. 1 Despite a high incidence, the individual as well as socioeconomic consequences are still underestimated. 1 Thus, osteoporotic vertebral compression fractures (OVCF) lead to a decrease in mobility, an increase in dependence, and lead to high mortality rates. At the end of the downward spiral described by Gold, there is a 5-year mortality rate of 72%. In comparison, the mortality rate for femoral neck fractures is “only” 59%. 2
Therefore, if conservative therapy fails, surgical intervention must be considered at an early stage in order to counteract the aforementioned downward spiral. However, there are also high complication rates associated with surgery. Little is known about which patient-specific and internal risk factors are associated with a poor clinical outcome.
The aim of the present work was to identify adjustable and non-adjustable factors on the basis of the available literature in order to recognize complicated courses in advance and to be able to positively influence the clinical result through targeted optimization of individual factors.
Material and Methods
Study Design
We conducted a comprehensive systematic review of the literature according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) checklist and algorithm. 3
Study Characteristics
Investigations between 2000 and 2020 were included. For analyses, prospective and retrospective observational investigation studies that dealt with medical comorbidities in connection of OVCF were considered. Furthermore, only articles in German or English were involved.
Information Sources
The authors performed an initial search of PubMed and Google scholar databases for investigations for possible inclusion in the review.
Search
The keywords used in the research were ("osteoporotic" OR "osteoporotics") AND ("spinal fractures" OR ("spinal" AND "fractures") OR "spinal fractures" OR ("vertebral" AND "fractures") OR "vertebral fractures" OR “Vertebral Compression Fractures”) AND ("Surgery" OR "BKP" OR "Ballonkyphoplasty" OR "Vertebroplasty" OR "Kyphoplasty" OR “Surgical Management”) AND ("Comorbidities" OR "Pre-existing illness" OR "Medicalization" OR "Medical" OR "Medication" OR "Medics" OR "medical condition") AND ("Complication" “Adverse outcome” OR “Complications” OR "Perioperative Complications" OR "General medical" OR "infection" OR "In-hospital stay" OR "Morbidity" OR "Mortality" OR "Functional outcome" OR "Quality of life" OR “Survival” OR “Treatment outcome”)
Study Selection
The authors limited the research to observational studies, while systematic reviews, meta-analyses, case series and case reports were excluded. Titles and abstracts were reviewed. Duplicates were removed and full texts were checked for suitability. In cases where a decision could not be taken based on information from the title and abstract, the full text was evaluated. The final decision was made based on the analysis of the full text. The study selection process was carried out independently by two authors (MJS, ML) (Figure 1). . PRISMA flow chart.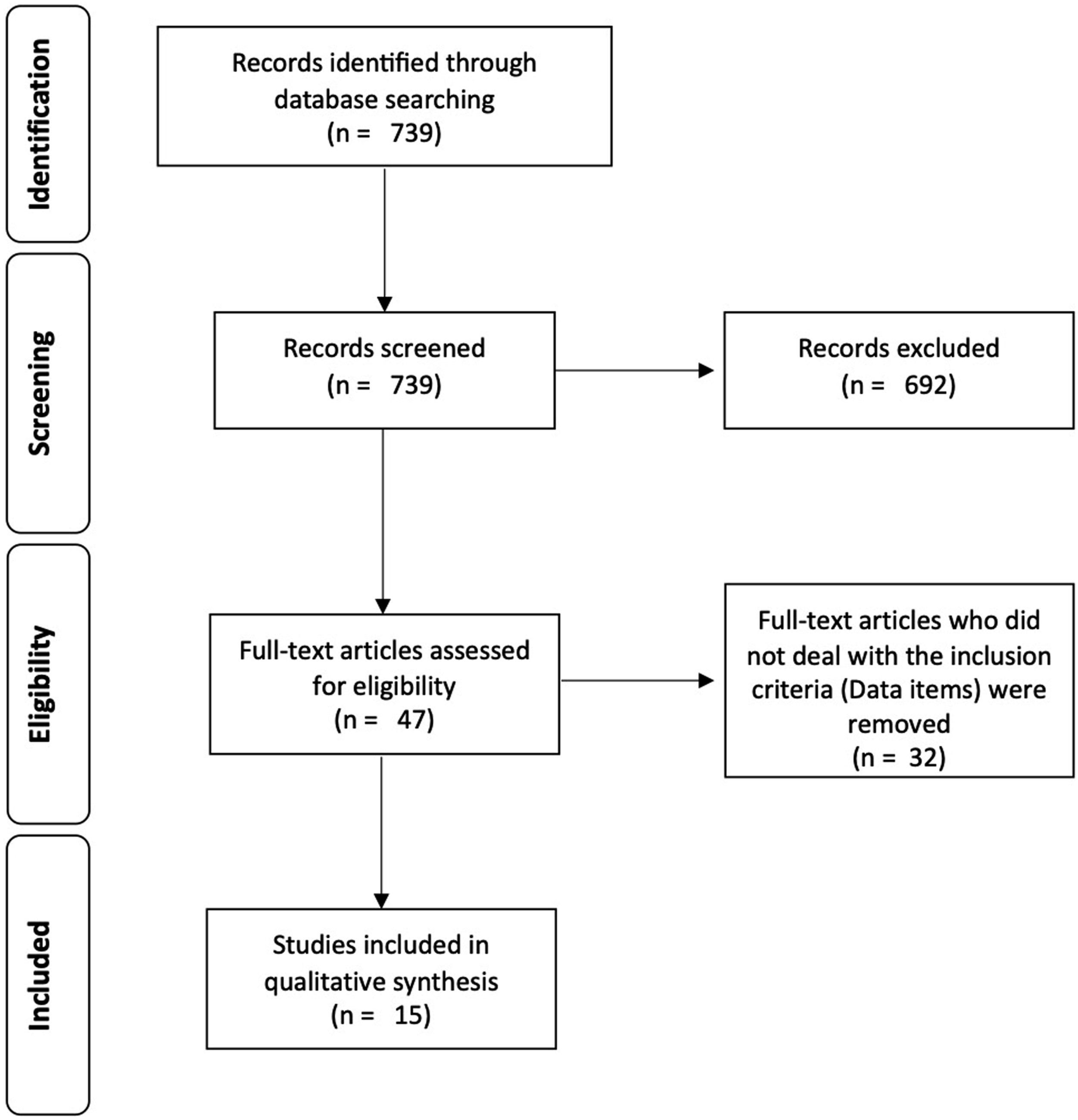
Data Items
The main prerequisite was that included studies dealt with medical comorbidities in connection with treatment of OVCF. The authors performed an initial search of both databases for investigations for possible inclusion in the review. First, title and abstracts were screened. In cases were a decision could not be taken due to the information from the title and abstract the full text was evaluated. In the end, the final decision was made based on the analysis of the full text.
Studies were selected according to the following inclusion criteria: (a) Risk factors for peri- and postoperative complications; (b) Risk factors for readmission; (c) Risk factors for in hospital stay; (d) Risk factors for In-hospital mortality; (e) Risk factors for overall mortality; (f) Risk factors with negative influence on clinical outcome.
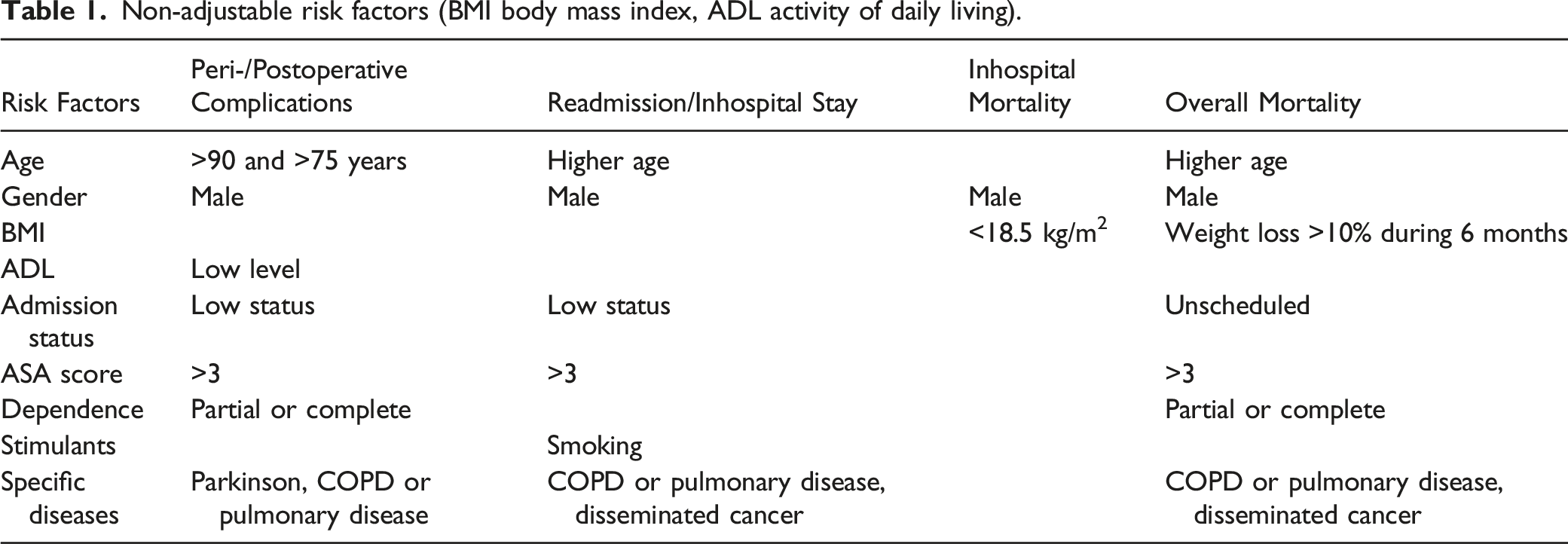
Non-adjustable risk factors (BMI body mass index, ADL activity of daily living).
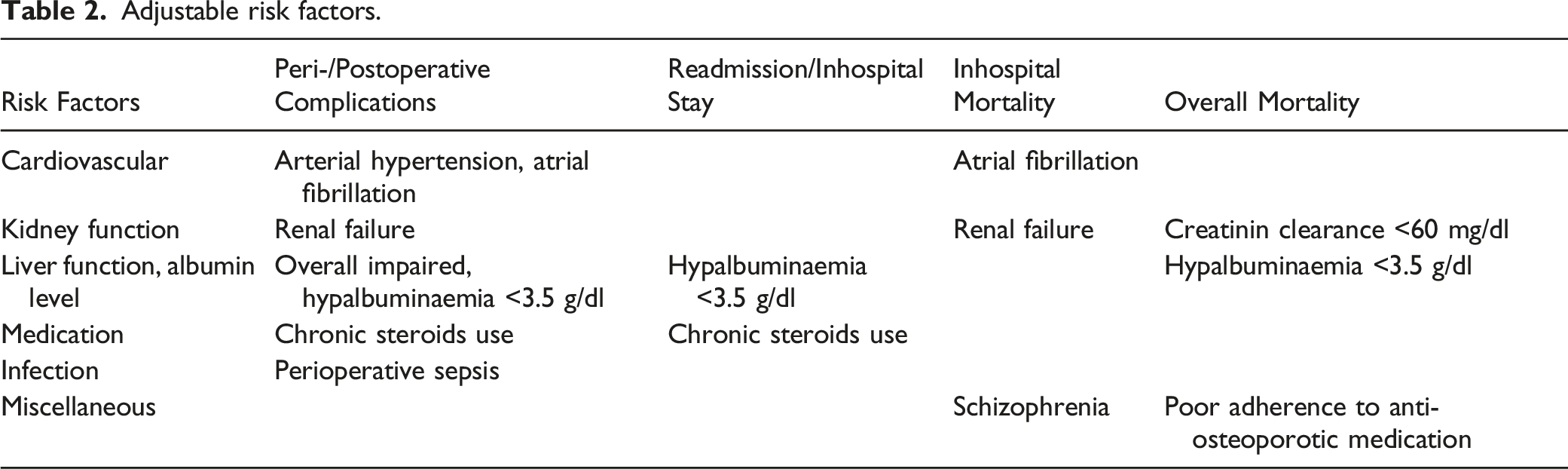
Adjustable risk factors.
Synthesis of Results
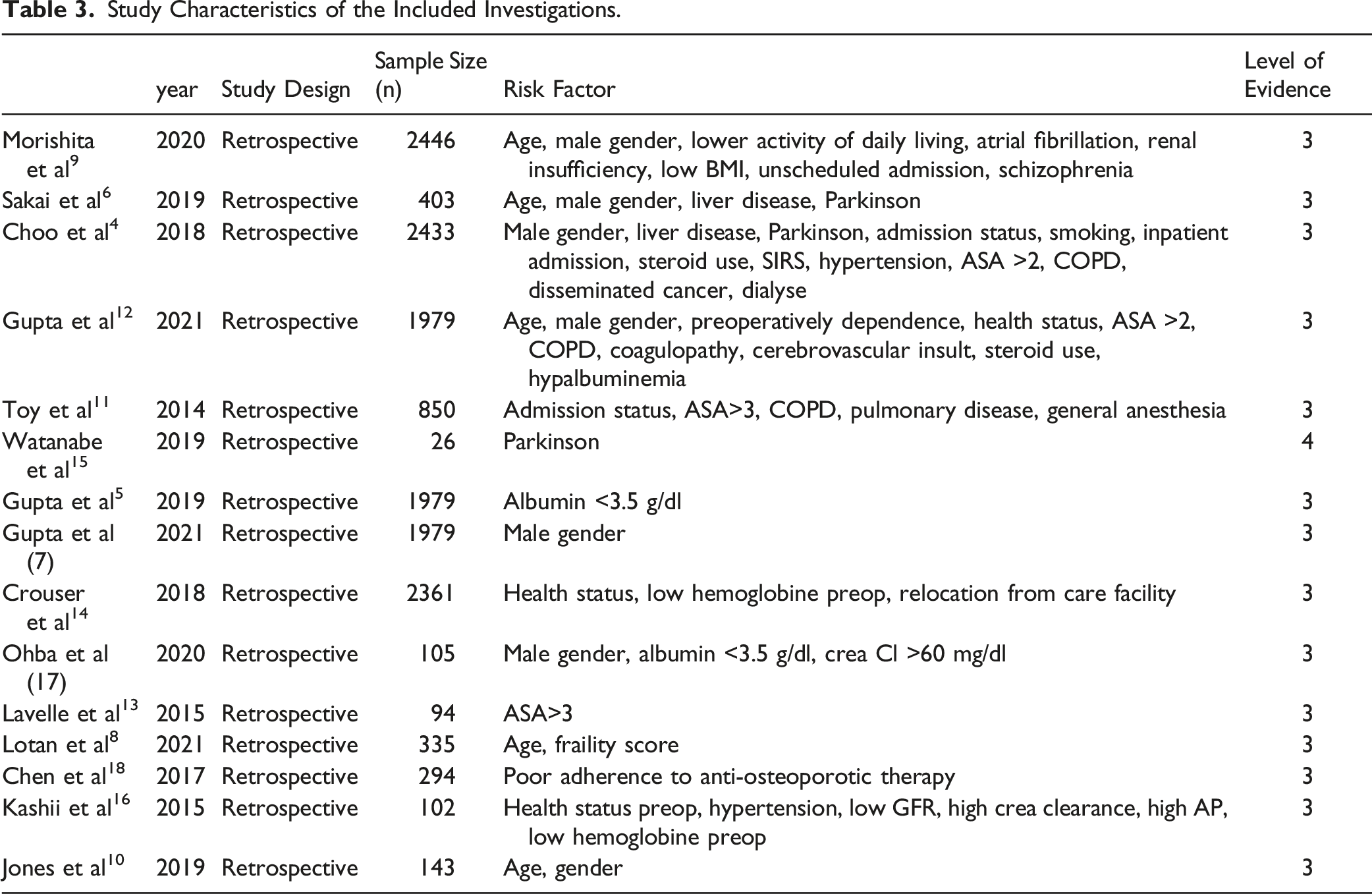
Study Characteristics of the Included Investigations.
Results
Risk Factors for Peri- and Postoperative Complications
Age was a major non-adjustable risk factor for peri- and postoperative complications: The older the patient the more likely systemic complications occur. However, with 75 years and >90 years different limit values were defined. Beside age, male sex was the second non-adjustable risk factor that seems to influence postoperative complications similar (P = .049).
Low activity of daily living (ADL) levels was significantly associated with higher complication rates (OR 1.52). Furthermore, partial or complete dependence increased the risk of minor or major postoperative complications similar. This results in the observation, that inpatient admission status was an independent predictor (OR 3.22; P < .001) of having any complication within 30-days of the surgery. Any adverse (AAE) as well as serious adverse events (SAE) were significantly associated with inpatient status before procedure (AAE: OR = 2.7, P < .001, SAE: OR = 2.4, P = .003). In a line was the association between American Society of Anesthesiologists (ASA) class and risk for complications. After multivariate analysis significantly higher AAE und SAE in ASA-class >3 patients could be seen (AAE: OR = 2.7, P = .013; SAE: OR = 2.5, P = .040).
Parkinson disease was further associated with more major complications (pulmonary embolism, cardiac events, stroke, renal failure and sepsis) (OR = 3,636, P = 0.009) as well as chronic obstructive pulmonary disease (COPD) (OR = 2.65, P = 0.004).
In contrast to abovementioned factors, cardiac, renal, hepatic, pulmonary and metabolic malfunction were adjustable risk factors, which influenced the risk for complications similar. Firstly, high blood pressure increases the patient’s ASA score up to 2, while the risk of septic complications rised (OR = 4.64, P = 0.044). Secondly, preoperative renal failure was a significant predictor of postoperative complications (OR = 21.6, P < 0.001). It was deeply associated with respiratory (pulmonary embolism, pneumonia, respiratory failure) and cardiac complications (infarction). Thirdly, an impaired liver function led to a wide spectrum of clinical pathologies: coagulopathies, impaired wound healing, respiratory and renal dysfunction as well as encephalopathy (OR = 8.993, P < 0.001). Fourthly, chronic steroid use led to more respiratory (OR = 2.38, P = 0.016) and septic complications (steroids use: OR = 6.71, P < 0.001). Fifthly, preoperative sepsis or SIRS showed a higher rate of reoperation, progression of sepsis and thromboembolic complications (OR = 2.52, P = 0.009). Lastly, hypalbuminemia (<3.5 g/dl) was linked to develop more major complication (P < 0.001), prolonged hospital stay (P < 0.001), increased septic (P = 0.001) and pulmonary complications (P = 0.0047) as well as higher mortality (P < 0.001) compared to Albumin levels >3 g/dl.
Risk Factors for Readmission and Hospital Stay
The older a patient the higher was the risk to be readmitted within 30 days after surgery (OR 1.02; P = .004). Readmission rate was 10.6% after kypho- or vertebroplasty with significantly higher rates for older than for younger patients (76-89 years: OR 1.75; P = .013, or ≥90 years: OR 2.78; P < .001). According to higher complications rates in men the readmission rate was significantly higher, too (OR = 1.41; P = .017). Also, the inpatient admission status seems to be a significant risk factor for increased readmission rates (OR 1.58; P = .001). ASA grade >3 was a significant risk factor for readmission within 30 days after surgery (OR = 3.0, P = .005).
Further non-adjustable factors were chronic obstructive pulmonary disease (COPD) as well as other pulmonary diseases, which should be considered as they increased the 30 day readmission rates significantly (OR = 1.77, P = .001). Disseminated cancer turned out to be a strong risk factor for almost threefold increased readmission rates (OR = 2.98, P < .001). In this context history of smoking seems to be a significantly single risk factor for increased readmission rates (OR = 2.1, P = 0.002).
Adjustable risk factors were chronic steroid use (OR 2.21; P < .001) and preoperative declined albumin level <3.5 g/dl.4,5
In-Hospital Mortality
Male gender (OR =3.26, P = .021), BMI lower than 18.5 kg/m2 (OR = 3.97, P = .021) and unscheduled admission (OR = 3.52, P = .026) were risk factors for death during hospitalization. Atrial fibrillation (OR = 8.31, P = .001), renal failure (OR = 7.15, P = .023) and schizophrenia (OR = 8.23, P = .010) were described as comorbidities with a significant but with less strong effect related risk for in-hospital death. In addition, complete dependence from nursing seems to influence in-hospital death, too (OR = 5.68, P = .001).
Overall Mortality
The 30 days mortality rates ranged between 1.5% and 2.0%. Looking at a longer observation period, it increases up to 34.1% 7 years after OVCF.
Decreased functional health status, defined by the ASA-score, was statistically significantly associated with higher mortality rates (OR = 2.92; P = .002 ASA > 3 versus ASA ≥ 3; OR = 2.5; P = .040 ASA > 3 vs ASA < 3) as well as discharge of the patients to an inpatient care (OR = 3.62; P = .001). Further non-adjustable factors were frailty (HR 1.98; P < .019), male gender (HR 1.93; P > .01), and higher age (HR 1.11; P < .01) regardless of the treatment modality.
Among the adjustable factors poor adherence to anti-osteoporotic therapy during the first year had a significant effect on mortality (HR 1.75; P = .012). Additionally, hypoalbuminemia was found to be a significant risk factor for long-term postoperative mortality (HR 3.37; P = .014).
Other specific parameters with variable impact on the mortality rate after surgical treatment were pre-operative dialysis (OR = 11.74; P = .003], preoperative renal failure (OR = 14.61; P = .040), disseminated cancer (OR = 3.59; P > .001), and chronic steroid use (OR 3.59; P < .001), as well as weight loss of more than 10% over the last 6 months (OR = 4.45; P = 0.030) as risk factors for 30-day mortality. Additionally, history of pulmonary disease has been found to affects the 30-day mortality negatively (OR = 2.0; P = .005).
As predictive factors regarding mortality, declined serum albumin levels < 3.5 g/dl had a significant impact with an adjusted Hazard Ratio of 3.37 (P < .014). Next to albumin level, decreased Creatinine clearance (CL) < 60 mg/dl was identified as predictive factor with an adjusted Hazard Ratio of 1.96 (P = .25).
Another factor influencing the mortality in surgical treatment of OVCF negatively, was the use of nongeneral anesthesia (OR 4.6, P = .009).
Impact on Clinical Outcome
The strongest predictors of poor ADL were renal failure grade 3 or 4 (OR = .96, P = .005) and bone metabolism disorder with an increase in serum alcalic phosphatase (ALP) level (OR = 1.01, P = .01). In a further step-down, a glomerular filtration rate (GFR) below 60 (mL/min/1.73 m2) and CL below 60 mg/dl showed an OR 4.44 (P= 0.006) and in multivariate analysis an OR 7.26 (P = .001) and with an increase in ALP >325 (IU/L) an OR 4.81 (P=.002), and an OR 8.31 (P = .001), respectively. Albumin levels < 3.5 g/dl are correlated to poor functional outcome (OR .31, P = .01), too.
Further risk factors were low BMI <18.5 kg/m2 (OR .79, P = .006), low preoperative hemoglobin below 11.2 mmol/l (OR .70, P = .02) and arterial hypertension (OR .36, P = .05).
Positive improvement of Pain Health Questionnaire (PHQ) sore could be observed in female gender (P = .010) and older age patients. Age was found to have significantly better QOL with increasing age, such that every decade of increasing age was found to improve by 9.7 points (P = .001).
Discussion
In order to avoid complications and to achieve the best possible clinical result in treatment of patient with OVCF, it is necessary to identify specific risk factors in advance of the operation and to optimize them, if possible. In this context, it seems sensible to distinguish between adjustable risk factors that can be influenced and non-adjustable factors that are given (Tables 1 and 2).
In context with last mentioned, patient age and male sex seem to affect the perioperative course significantly (6-8) Especially perioperative systemic complications occur more frequent in elderly patients, 9 especially if they are over 90 years old 4 which increases the risk to be readmitted within 30 days after surgery. The main reason for the high readmission rate is frailty, which is influenced in particular by age, among other factors like ASA score. 10 Despite these observations, Gupta et al concluded that patient’s age should not be a stand-alone as contraindication to surgical intervention. 11
A low BMI, although rather uncommon, is an important risk factor, too. A BMI less than 18.5 kg/m2 as well as weight loss of more than 10% over the last 6 months have been cited as a threshold. 10
An ASA score of 3 and higher is considered a significant risk factor.10,12 Other works have already seen a noticeable difference from an ASA score of 211 but did not differentiate further each ASA grade (1-4). 11 Higher ASA score is also associated with the increased risk in patients with lower activity of daily living (ADL) levels upon admission or partial or complete dependence.4,9,11
Also, the inpatient admission status seems to influence the clinical outcome.4,13 One reason could be that the collective of patients with an inpatient status before admission had more severe fractures. 10
Beside aforementioned, comorbidities influenced the clinical course after surgery. Especially Parkinson’s disease plays an important role as the associated regress in motoric abilities lead to frequent falls and therefore a higher rate of fragility fractures. Furthermore, the affected patients are prone to respiratory complications, as well as surgical site infection, postoperative delirium and inferior walking ability.6,14 Compared with a control group, they develop more major complications (pulmonary embolism, cardiac events, stroke, renal failure and sepsis). 14 Care must be taken to ensure an optimal preoperative drug adjustment. A disseminated tumor disease is related to perioperative complications as well as overall mortality, which certainly needs no further explanation. 4
In order to optimize clinical outcome after surgery for OVCF factors that can be influenced preoperatively should be evaluated. Hereby, comorbidities like cardiac, renal, hepatic, pulmonary and metabolic malfunction play an important role and should be optimize preoperatively as far as possible. Above all, COPD as well as other pulmonary diseases increased the risk of adverse events significantly.4,6,9-11,15 The present of atrial fibrillation lead to more thromboembolic events and postoperative bleeding was more common in patients with high blood pressure.5,9,14 Also, impaired liver function increased the complication rate up to 50%, whereby coagulopathies with consecutive postoperative bleeding, impaired wound healing, respiratory and renal dysfunction as well as encephalopathy were the main adverse events. 6
A special focus in the preoperative preparation should be placed on the kidney function, as renal insufficiency was a significant predictor of inhospital mortality, overall mortality as well as respiratory and cardiac complications.4,9,16 It increased the 90 - day - mortality by a factor of 5. 4 The authors defined a GFR smaller than 60 mL/min and a creatinine clearance < 60 mg/dl as the critical thresholds.
Beside optimization of renal insufficiency by abandon renal-toxic medication and optimizing patient’s fluid status, preoperative albumin could play a crucial role in preoperative preparation of patients as the degree of hypalbuminemia strongly correlates with the risk of postoperative heart failure, prolonged hospital stay, increased septic and pulmonary complications as well as long-term postoperative mortality.5,11,15,16 Therefore, preoperative hypoalbuminemia should be optimized consequently. A hypalbuminemia of <3.5 g/dl is usually used as the critical value.
Finally, it is not surprising, that a sufficient osteoporotic therapy seems to have positive influence on patient outcome 17 and is of general importance in patients with OVCF.
Several authors have already made attempts to consider important comorbidities when determining the indication for surgery in OVCF. In this context, the Osteoporotic Fracture (OF) Classification-based scoring system should be mentioned, which, among other factors, also takes into account the extent of mobility and the state of health (ASA scores, BMI, dementia, nursing case and anticoagulation). 18 The 5-item Modified Frailty Index, which includes cardiac diseases, diabetes mellitus, COPD/pneumonia dependent functional health status and hypertension requiring medication, also enables an assessment of the clinical outcome after kyphoplasty.19,20 Considering both assessment protocols would include most of the risk factors demonstrated in this review.
This systematic review has some limitations. Firstly, the definition of complication was not consistent in most investigations. Secondly, study designs, study population and follow-up vary between the included studies. Both circumstances make comparison of the results as well as further statistical evaluation in the form of a correlation analysis difficult. Thirdly, all investigations were retrospective analysis where the data quality cannot be evaluated.
Conclusion
In summary, there are a number of non-adjustable factors that cannot be influenced preoperatively, but must be considered in terms of risk assessment. Age > 90 years, male gender, BMI less than 18.5 kg/m2, ASA score >3, reduced ADL, dependence, impaired inpatient admission status, Parkinson’s disease, and disseminated cancer should be considered preoperatively in terms of risk assessment but cannot be influenced. In those cases, surgical intervention should be strictly questioned.
Even more important are adjustable factors that can be influenced preoperatively: nutrition status, anti-osteoporosis medication, medical adjustment of kidney, liver and cardiopulmonary function, as well as of any further disease. Therefore, interdisciplinary cooperation, especially with geriatricians, appears to be essential in order to achieve the best possible clinical result in geriatric patients undergoing surgery for OVCF.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was organized and financially supported by Deutsche Gesellschaft für Orthopädie und Unfallchirurgie e.V. (DGOU).