
Abstract
Study design
Narrative review.
Objective
It is known that adult spinal deformity surgery (ASD) is associated with a high medical complication rate. However, it remains unclear which comorbidities impact these adverse events. The purpose of this study was to review the current knowledge regarding the association between postoperative medical complications and comorbidities.
Methods
The literatures in English were searched using PubMed. The search method involved a combination of keywords including “adult spinal deformity,” “complication,” and each specific risk factor. The search was limited to items listed in PubMed by February 15, 2022. The odds ratio (OR) of medical complications and mortality were evaluated.
Results
A total of 94 publications were reviewed. The risk factors with the higher OR for medical complications were frailty (OR: 4.4, 95% CI: 2.0-9.9), ASA class 4 (OR: 3.58, 95% CI: 2.00-6.39), male sex (OR: 3.52, 95% CI: 1.78-6.96), malnutrition (OR: 2.89, 95% CI: 1.69-4.93), and pathologic weight loss (OR: 2.38, 95% CI: 2.01-2.81). Similarly, the risk factors with the higher OR for mortality were liver disease (OR: 36.09, 95% CI: 16.16-80.59), pathologic weight loss (OR: 7.28, 95% CI: 4.36-12.14), renal failure (OR: 5.51, 95% CI: 2.57-11.82), chronic heart failure (OR: 5.67, 95% CI: 3.3-9.73), and age over 65 (OR: 3.49, 95% CI: 2.31-5.29).
Conclusion
This review demonstrates the impact of a patient’s comorbidities on postoperative medical complications. Understanding the level of risk involved can help to provide surgeons and patients with the information required to determine the suitability for surgery.
Keywords
Introduction
Adult Spinal Deformity (ASD) is characterized by a complex pathophysiology, encompassing not only coronal spinal malalignment as previously studied but also incorporating elements of sagittal spinal malalignment. Emerging evidence suggests that sagittal malalignments caused by particularly lumbar lordosis and pelvic retroversion, bear stronger clinical relevance than coronal spinal malalignment in impacting patient outcomes.1,2 In 2012, Schwab et al introduced the Scoliosis Research Society-Schwab Adult Spinal Deformity Classification based on abnormalities observed in the lumbar spine, pelvis, and global alignment on whole spine standing radiographs. 3 This classification has since become the prevailing standard for defining and categorizing ASD.
The complication rates in ASD surgery are reported to be as high as 40%,4-6 and the reoperation rate is 21%. 7 In the context of cost-effectiveness in ASD surgery, Carreon et al investigated the cumulative costs and cost-effectiveness over a 5-year period between surgical and non-surgical (conservative) treatment groups. The cumulative costs in the surgical group were $96,000, with an increase of 2.44 Quality-Adjusted Life Years (QALY) reported. 8 In contrast, the conservative group incurred $49,546 in cumulative costs, with an increase of .75 QALY. The study concluded that the surgical group demonstrated superior cost-effectiveness. However, it should be noted that postoperative readmissions were observed in 24% of ASD cases, with reports indicating costs of $92,755 for pseudoarthrosis, $75,172 for infection, and $66,713 for proximal junctional kyphosis. 9 While research on mechanical complications and cost-effectiveness in ASD surgery is available, there remains a scarcity of studies reporting on the association with medical complications.
Bhargava et al studied more than 60,000 patients over the age of 80 years who underwent general spine surgery from three national databases. They found that the medical complication rate during hospitalization was 5% and the mortality rate was .2%. 10 However, the incidence of these medical complications increases further in highly invasive ASD surgery. Oe et al, 11 in a study of 285 ASD patients undergoing deformity surgery, reported a 33.7% medical complications rate that increased to 49.2% in patients with pre-operative poor nutritional status. Similarly, Soroceanu et al 12 reported a medical complication rate of 26.8% in 448 ASD patients. Hypertension (Incidence rate ratio; IRR 2.43) and smoking (IRR 2.49) were identified as significant risk factors. The incidence of medical complications in ASD surgery is notably elevated in comparison to general spine surgery. Various comorbidities (such as hypertension, diabetes, respiratory disorders, and heart disease) and patient characteristics (including age, sex, obesity, and malnutrition) have been identified as significant risk factors contributing to these complications. With reports suggesting an ASD rate of 32% to 68% in patients over the age of 65 the number of ASD surgeries is expected to increase in the future,13-15 making the need to minimize adverse events all the more important. In order to prevent postoperative adverse events, it is important to identify risk factors for postoperative complications and, if possible, whether they can be addressed before surgery. However, few review papers have investigated the impact of comorbidities and patient background on postoperative medical complications. The purpose of this study was to review the current knowledge of postoperative adverse events focused on medical complications and comorbidities in patients undergoing surgery for ASD.
Material and Methods
Ethical Considerations
This study, being a literature review and not involving human subjects or samples, does not require informed consent or approval from Institutional Review Board.
Literature Review
We conducted a literature search limited to English using PubMed. The search method used was a combination of “adult spinal deformity”, “complication”, and each risk factor (comorbidities and patient’s characteristics) for medical complications. The selection of risk factor was based primarily on the Charlson Comorbidity Index (CCI) and American Society of Anesthesiologists (ASA) Physiological Status classification. The literature search was conducted by two experienced spine surgeons with over 10 years of experience. Only literature written in English was included in the evaluation. The search was limited to items that were listed in PubMed by February 15, 2022. Whenever possible, studies involving patients with ASD were reviewed, but When appropriate, literature involving patients other than those with ASD or general spinal disorder was also considered for evaluation. We excluded literature where the deformity was due to infection, tumor or symdromic conditions. In addition, osteoporosis and blood management including anemia and blood transfusion as risk factors for adverse event were not included in this review as they have a separate dedicated section in this focus issue.
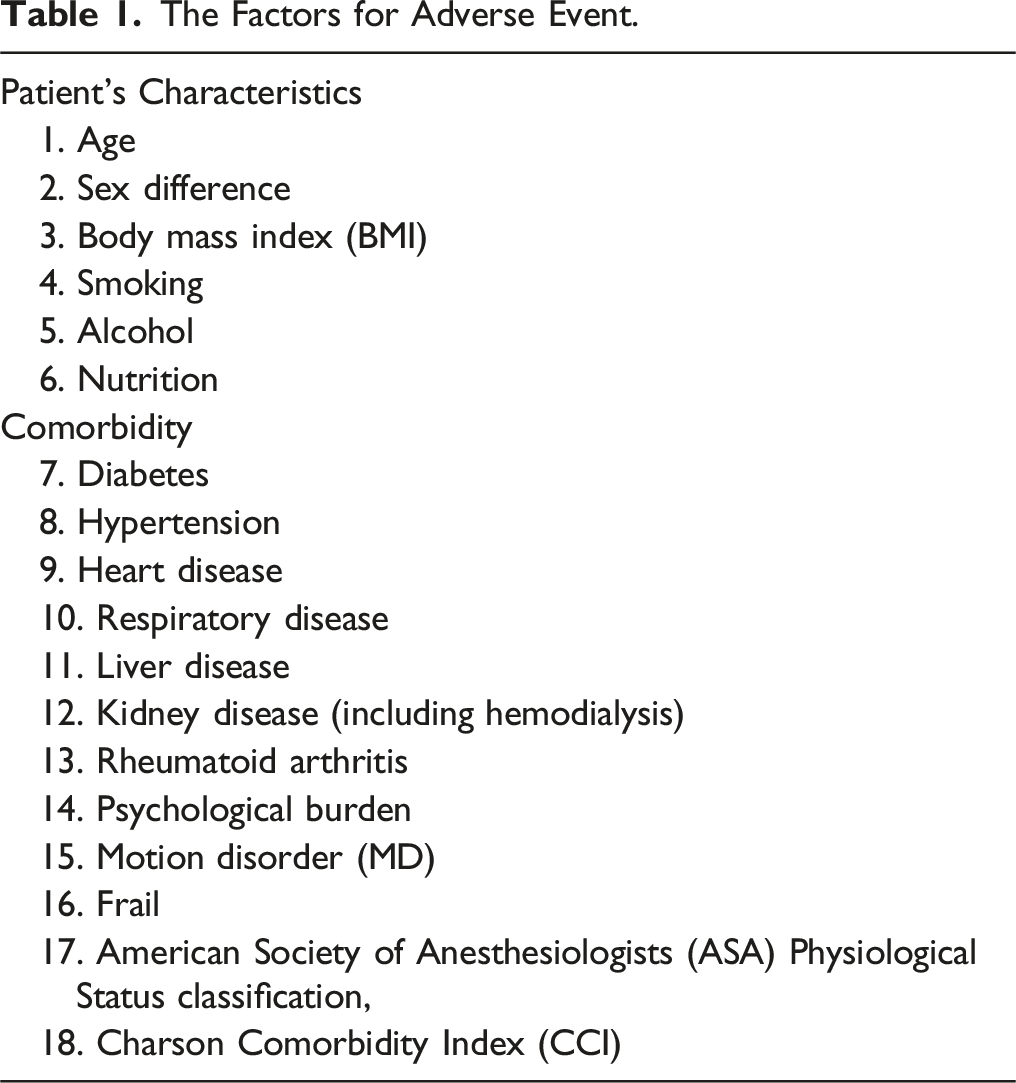
The risk factors of patient’s characteristics were age, sex, body mass index (BMI), smoking, alcohol, nutritional status. Factors for major comorbidities included diabetes, hypertension, heart disease, respiratory disease, liver disease, kidney disease, rheumatoid arthritis, psychological problem, motion disorders (MD), frailty, malignancy, ASA Physiological Status classification, and CCI.
Results
The Patient’s Factors
Age
There are many reports suggesting that higher age is associated with postoperative complications. Lau et al reported a significant association between age and overall complications (P = .002) as well as medical-specific complications (P < .001). The rates of overall and medical complications were 9.7% and 6.5%, respectively, for patients younger than 50 years, 16.7% and 10.2% for those aged 50-64 years, 31.4% and 22.6% for those aged 65-79 years, and 41.7% and 41.7% for those aged 80 years or older. 16 Furthermore, higher age was identified as an independent factor associated with longer ICU stay (P = .028) and total hospital stay (P = .003). Similarly, a nationwide study involving 11,982 discharges in ASD surgery found that age >65 was linked to increased morbidity and mortality compared to the age 25-64 group, with odds ratios of 1.09 (95% CI 1.05-1.14) and 3.49 (95% CI 2.31-5.29), respectively. 17 Another study by Oe et al 18 reported that delirium was the most common complication in ASD surgery, occurring in 26 out of 141 (18.4%) patients aged 68.5 years or older. These results suggest that patients over 65 years of age are at an increased risk of medical complications and mortality after ASD surgery. However, it is important to acknowledge that there is significant heterogeneity among individuals aged 65 years and older, particularly in terms of their health status. Considering patient stratification based on frailty rather than solely on age may offer more meaningful insights. However, further research is warranted to explore this relationship in greater depth.
It should also be noted that aging is strongly associated with osteoporosis, and that osteoporosis associated with aging is likely to cause instrumentation failure. 19
Sex
In adolescent idiopathic scoliosis (AIS), it is known that males tend to experience higher intraoperative blood loss, longer operative times, and higher complication rates compared to females.20,21 This has been attributed to the greater and rigid curves in males during surgery, but the exact reason is not clear. Despite this, there is no consensus regarding the difference in adverse events between males and females undergoing ASD surgery. Bumpass et al 22 conducted a study comparing the postoperative outcomes of 90 men and 319 women and found no significant differences in complication rates or health-related quality of life (HRQOL). On the contrary, Oe et al 11 performed a multiple logistic regression analysis and reported an OR for the risk of medical complications of 3.5, with a 95% confidence interval (CI) of 1.78-6.96 in males compared to females. Further adding to the complexity of the role of sex in adverse events, Worley identified female sex as a significant risk factor for medical complications in ASD surgery, showing an increased morbidity [OR 1.18 (95% CI 1.13-1.23)] and decreased mortality [OR .30 (95% CI .21-.44)]. 17 Thus, the difference in complications between men and women remains controversial, and future large-scale studies with a high level of evidence are needed.
BMI
High and low BMI have been associated with various comorbidities (cardiovascular, respiratory, endocrine, digestive, musculoskeletal) and, therefore, considered to be prone to perioperative complications. Both obese and underweight patients are at risk of increased adverse events and perioperative mortality.23,24 In ASD surgery, Sorocesnu et al showed that obese patients (BMI ≥30 kg/m2) had a higher overall incidence of major complications (IRR 1.54, P = .02) and wound infections (odds ratio 4.88, P = .02). 25 In a series of general spine surgery, Ushirozako et al 26 reported that BMI ≥30 kg/m2 was a significant risk of SSI (OR 2.89, 95%CI 1.20-6.97). On the other hand, Kobayashi reported that lower BMI (≤20.39 kg/m2) was a significant risk factor of SSI. 27 In addition, pathologic weight loss is associated with postoperative medical complications (OR 2.38, 95%CI 2.01-2.81). 17 In terms of patient reported outcomes, Soroceanu et al 25 reported that the SF-36, ODI, and SRS-22 improve significantly following ASD surgery in both groups with and without obesity, however, the rate of improvement was lower in the obese group.
Moreover, the cost per QALY of ASD surgery was $8,588.70 (BMI <18.5), $12,805.72 (BMI 18.5-24.9), $16,221.32 (BMI 25-25.9), $27,574.77 (BMI 30-34.9), $18,317.11 (BMI 35.0-39.9), and $9,591.06 (BMI ≥ 40). 28 The study revealed that patients with lower body weight and those with a BMI ≥ 40 exhibited relatively lower cost perQALY. This phenomenon can be attributed to a significant difference in baseline EQ-5D scores, which were notably poorer in these groups compared to others. Consequently, these patients experienced substantial postoperative improvements in EQ-5D scores, resulting in the observed lower cost per QALY. When assessing 1 year cost per QALY, obese patients had costs 32% higher than nonobese patients ($224,440.61 vs $331,048.23).
Smoking
Smoking is commonly known to cause respiratory complications in surgeries requiring general anesthesia. Soroceanu et al 12 showed smoking to be a significant risk factor for medical complications in ASD surgery and the IRR for medical complications was 2.49 (P = .0001). On the other hand, de la Garza et al showed that smoking was not associated with 30-day complications or mortality after ASD surgery. 29 Of the 1368 patients, 15.9% were smokers and 84.1% nonsmokers. The proportion of smokers who developed at least one complication was 9.7% vs 13.6% for nonsmokers (P = .119). Wilson et al reported that surgery-related excessive bleeding (>4 L) was significantly higher in the smoking group in ASD surgery (smoking group = 5/26 vs non-smoking group = 9/244; 19.2% vs 3.7%; OR 6.22 [95%CI 1.48 - 22.75]; P = .006). 30 Smoking is also associated with post-operative pneumonia, and it is recommended that patients quit smoking at least 8 weeks prior to surgery. 31 Moreover, there are some reports that smoking impact to SSI. Nota et al studied the incidence of surgical site infection in 5761 patients undergoing spinal surgery. 32 They reported that smoking was a risk factor for SSI in 443 (8.0%) of 5545 non-infected cases and in 30 (13.9%) of 216 infected cases (P = .002). On the other hand, a meta-analysis evaluating 20 articles investigating the association between spinal surgery and SSIs concluded that there was no relationship between smoking and SSIs, with the incidence of SSIs in the smoking group being 226 of 7690 patients (2.9%) and in the non-smoking group 908 of 30514 patients (3.0%) (OR 1.15, 95% CI: .99 -1.35). 33
Alcohol
Alcohol consumption is associated with increased blood loss, length of stay (LOS), transfer to the intensive care unit (ICU), postoperative infections, wound complications and cardiopulmonary dysfunction.34-39 In a retrospective study which compared 317 ASD surgery patients who drink alcohol with 693 who do not, Elsamadicy et al 40 reported that there was no significant difference in the incidence of medical complications during the first 30 days after surgery; rather, intraoperative bleeding and ICU admission rates were significantly higher in the non-drinking group.The association between alcohol consumption and adverse events after ASD surgery has rarely been reported and remains controversial.
Nutrition
There are numerous reports that malnutrition is a cause of postoperative complications. The complications reported are SSI,26,41-44 wound complications,45,46 delirium,11,18,47-50 heart failure,43,44,46 respiratory failure,45,46 renal failure,42,44 pneumonia,42-44 urinary tract infection,42,44 pulmonary embolism (PE), 44 unexpected reintubation,42-44 prolonged hospital stay,45,46 and death.42,45,46,51-53 However, there is little literature on the relationship between ASD surgery and malnutrition. Oe et al 18 evaluated the nutritional status in ASD patients using prognostic nutritional index (PNI). They concluded that the most common complication was delirium, with a cutoff value of 50 for PNI. Moreover, they also reported that the patients with PNI < 50 had medical complications in 58 of 118 cases (49.2%) after ASD surgery 11 compared with a rate of 38 of 167 (22.8%, P < .0001) in patients with PNI > 50. 11 The OR for the incidence of medical complications in patients with PNI < 50 was 2.888 (95% CI 1.691-4.933), demonstrating that malnutrition is a significant predictor of medical complications.
Although there are only a few reports on nutritional status and ASD surgery, more large-scale studies are needed to determine the impact of malnutritional on outcomes in ASD surgery, and to determine whether improving nutritional status before surgery can reduce the occurrence of adverse events.
Comorbidity
Diabetes
In a database study of ASD surgery, Caupa et al reported that diabetes status was significantly associated with length of stay ≥5 days (non-insulin-dependent diabetes mellitus [NIDDM]: OR: 1.27, 95%CI: 1.02-1.58, P = .034; insulin-dependent diabetes mellitus [IDDM]: OR = 1.55, 95% CI = 1.15-2.09, P = .004), any complication (NIDDM: OR = 1.26, 95% CI = 1.01-1.58, P = .037), urinary tract infection (NIDDM: OR = 1.87, 95% CI = 1.14-3.05, P = .012), and cardiac complications (IDDM: OR = 4.05, 95% CI = 1.72-9.51, P = .001). 54 In addition, Olsen et al 55 reported that a preoperative glucose >125 mg/dL or a postoperative glucose >200 mg/dL was associated with higher odds (OR:3.3) of SSI even in the absence of diabetes in patients undergoing general spinal surgery. Diabetes status also impacts on postoperative outcome. Takahashi et al showed that patients with glycosylated hemoglobin of 6.5% or more showed a 2-fold increase of poor improvement of low back pain (OR = 2.37; 95% CI, .99-5.70) in lumbar spine surgery, and patients with diabetes for 20 years or more were more likely to experience poor improvement of low back pain and leg numbness (OR = 4.95; 95% CI, 1.69-14.5 and OR = 2.80; 95% CI, .98-7.94, respectively). Insulin use was also associated with poor improvement of leg numbness (OR = 4.49; 95% CI, 1.24-16.3). 56 Diabetes mellitus affects postoperative complications and is associated with poor postoperative outcomes.
Hypertension
Hypertension causes arteriosclerosis, which is associated with diseases of the blood vessels throughout the body. 57 However, there are few reports describing the relationship between hypertension and spinal deformity. It has been reported that atherosclerosis causes disc degeneration by blocking blood flow to the discs. 58 Arima et al 59 reported that hypertension was a significant risk factor for increasing of the sagittal vertical axis in a cohort study of health screening.
Regarding adverse events, Soroceanu et al conducted a survey of medical complications within 6 weeks after ASD surgery and reported that the most common complication was cardiopulmonary disease (deep vein thrombosis, arrhythmia, heart failure). Furthermore, among the various characteristics, hypertension was shown to be a significant risk factor, with an IRR of 2.43 (P < .001). 12 In addition, hypertension has been cited as a risk factor for complications in studies of patients older than 75 years (OR 10, 95% CI 1.3-78; P = .02). 60 However, the specific level of blood pressure elevation associated with adverse events in adult spinal deformities is not clear and remains to be determined.
Heart Disease
Cardiac diseases include arrhythmia, ischemic heart disease, and heart failure, which are sometimes life-threatening complications. In a database study of 1250 patients, Ramos et al investigated complications within 30 days of surgery. The OR for complications of congestive heart failure was 1.0. 61 On the contrary, there is also the report that the IRR for heart disease after ASD surgery was 2.07 (P < .01). 12 Moreover, Worley et al 17 reported that the OR of chronic heart failure for medical complications and mortality was 1.62 (95%CI 1.42-1.84) and 5.67 (95%CI 3.3-9.73), respectively. While most patients with severe cardiac disease are declined for major elective spine surgery, identifying patients with cardiac disease remains important in the pre-operative work-up of ASD patients.
Respiratory Disease
Respiratory dysfunction, such as asthma and chronic obstructive pulmonary disease (COPD), has a significant impact on postoperative complications. Rizzi et al 62 reviewed 35 patients with respiratory dysfunction who underwent spinal deformity surgery and reported that seven patients died within one year of surgery. In addition, there is a 4.7-fold increase in respiratory complications in patients with COPD in any surgery. 63 Moreover, Worley et al reported that chronic pulmonary disease was significantly associated with medical complications (OR 1.08, 95%CI 1.02-1.14). 12 On the other hand, the OR for the incidence of medical complications in COPD was reported to be 1.1 (95% CI .53-2.27) and IRR 1.59 (P = .11).12,61 This might be due to the fact that there is a difference in the severity of respiratory dysfunction. In the future, it is necessary to investigate the incidence of complications according to the severity of respiratory impairment. However, it has been reported that preoperative respiratory function training can improve postoperative pneumonia and atelectasis by up to 50%, and it is recommended that patients with lung disease undergo respiratory function training before surgery.64-66
Liver Disease (Including Liver Cirrhosis)
There is no report about liver cirrhosis and few reports on the impact of liver dysfunction on adverse events after ASD surgery. Worley et al 17 reported in a database study that the OR for mortality of liver disease was 36.09 (95% CI 16.16-80.59), which was the highest among their comorbidities. Moreover, Lu et al 67 reported that the impact of liver disease was longer hospital stay (OR 2.16, 95% CI 1.664-2.84), respiratory complications (OR 1.78, 95% CI 1.16-2.74), blood transfusion (OR 1.67, 95% CI 1.36-2.05), and any complications (OR 1.43; 95% CI 1.15-1.77; P = .001) within 30 days after the surgery. Because most patients with severe liver disease are declined surgery for ASD, there is limited reports on peri-operative adverse events related to liver dysfunction.
Kidney Disease (Including Hemodialysis)
Worley et al 17 showed that the OR of renal failure for medical complications was 1.29 (95%CI 1.13-1.47). The incidence of complications may be different in hemodialysis patients because of the difficulty in controlling circulatory dynamics and electrolyte balance. However, there was no report focusing on the relationship between hemodialysis and ASD surgery. Han et al 68 reported that in 12 patients with hemodialysis who underwent lumbar spine surgery, one patient died of sepsis due to pneumonia, and three patients developed delirium. In a study of lumbar spine surgery, Hori et al reported that the mortality rate was significantly higher in hemodialysis group (29 patients) than in the non-dialysis group (57 patients) (17.2% vs 0%, P = .003) at mean follow-up 2.4 years. 69 Maruo et al 70 also reported that 6 of 36 patients who underwent lumbar fusion surgery died within 1 year after surgery. Spinal surgery in hemodialysis patients has a high postoperative mortality rate, and the indication for surgery should be carefully considered.
Rheumatoid Arthritis
RA leads to osteoporosis and decreased immune status due to the use of steroids and immunosuppressive drugs.71-73 In fact, Benstein et al reported in a database-based study in ASD patients that postoperative infections (1.76% vs 1.20% P = .032) and urinary tract infections (6.23% vs 4.09% P < .001) were significantly higher in RA patients. 74 Mesfin et al conducted a comparison between 14 patients with RA and 14 non-RA patients after ASD surgery, reporting a total of 23 major complications in the RA group (compared to 11 in the non-RA group, P < .001). Among these, the most frequent serious complications identified were SSI, death, and respiratory complications. 75 In contrast, another study suggested RA is not associated with postoperative medical complication (OR .95, 95%CI .87-1.04, P = .261) and mortality (OR .93, 95%CI .37-2.35, P = .882). 17 Although there are few reports focusing on RA and ASD, the use of steroids or disease modifying drugs may influence the outcome in these patients.
Psychological Burden
There are reports that scoliosis can affect mental status.76,77 Diebo et al 77 showed that 37.5% of patients with fusion surgery of 4 levels or more had at least one psychiatric comorbidity. This includes 16% depression, 7.1% sleep disorders, and 6.7% anxiety disorders. On the other hand, it is shown that comorbid mental health disorder was a significant predictor of any complication (OR 1.17, 95%CI 1.04-1.32, P = .01) and readmission (OR: 1.32, 95%CI 1.17-1.5 P < .001). Mental health disorder was the strongest predictor of any revision (OR: 1.56, 95%CI 1.56, P < .001). 78 Moreover, there is a report that mental illness had significantly increased rates of infection (OR 1.743, 95%CI 1.10-2.76, P = .022) and respiratory complications (OR = 1.492, 95%CI 1.08-2.07, P = .02) at the 90-day postoperative period. 79
Movement Disorders
Comorbidity of MD, such as Parkinson's disease, affect postoperative adverse events. The incidence of delirium in MD patients is significantly higher at 5.7-10.3%.80-82 According to a database study among ASD surgery by Valshneya et al, the medical complication rate for MD patients was 44.6% and for the controls 35.6% (P = .009). 82 The two most common perioperative complications were acute-posthemorrhagic anemia (26.9% vs 20.8%, P < .05) and deficiency anemia (15.5% vs 8.5%, P < .05). At 90 days, MD patients were more likely to be readmitted (17.4% vs 13.2%, P < .05) and have a higher total cost ($94,672 vs $85,190, P < .05). MD was also reported to be a significant risk factor for postoperative medical complications (OR 1.464, 95% CI 1.170-1.830) and inpatient readmission (OR 1.386, 95% CI 1.023-1.843, P = .0295).
Frailty
It is well known that frailty is a significant predictor of postoperative adverse events, mortality and length of hospital stay.83-86 This concept, proposed by Buchner et al in 1992, became internationally known with the report by Fried et al in 2001.87,88
Fried et al presented a phenotypic model using the following five items: 1. weight loss (unintentional), 2. weakness of grip strength, 3. exhaustion, 4. slowness of walking speed, and 5. low activity. They defined Frail as when three or more of the five items were met, and Prefrail as when one or two items were met.
The Factors for Adverse Event.
The Variables of Adult Spinal Deformity-Frailty Index.
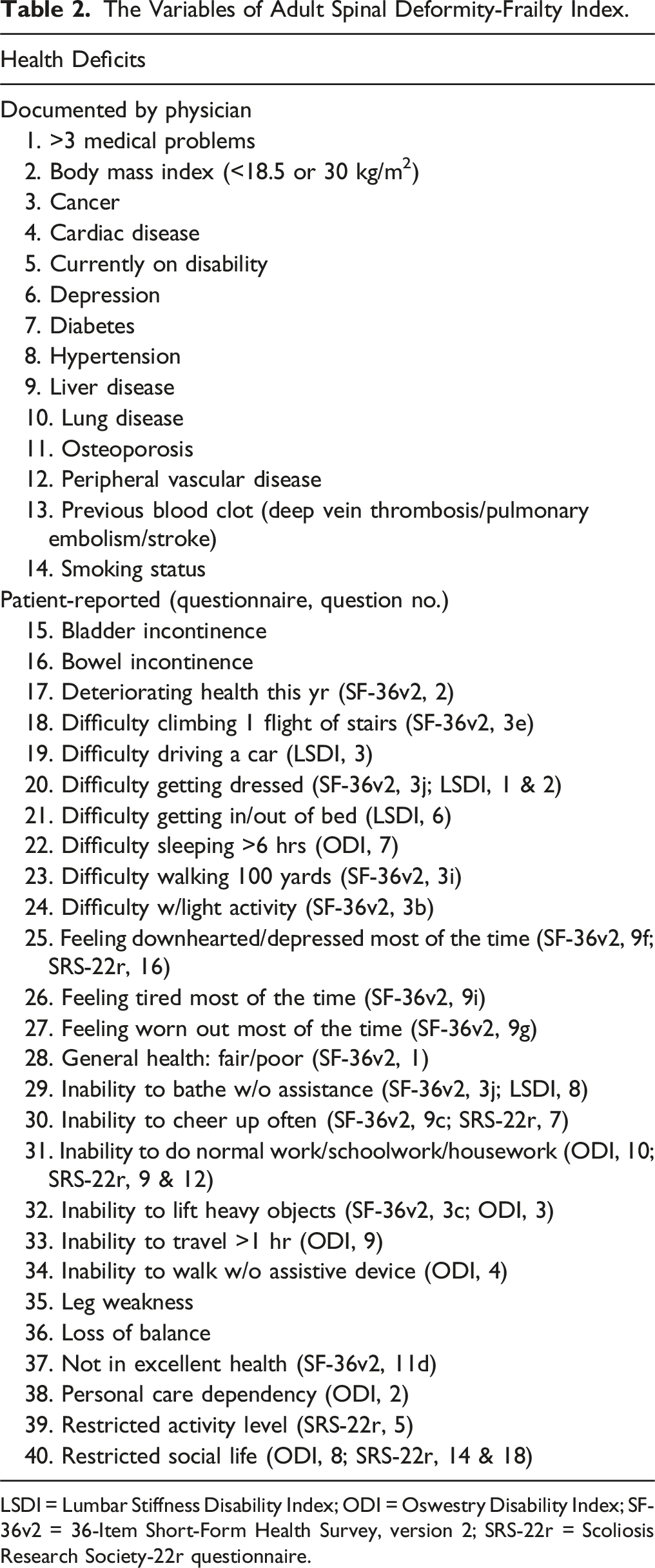
LSDI = Lumbar Stiffness Disability Index; ODI = Oswestry Disability Index; SF-36v2 = 36-Item Short-Form Health Survey, version 2; SRS-22r = Scoliosis Research Society-22r questionnaire.
Future work on the assessment of frailty should include the development of an established scale that is simple and easy to use.
ASA Classification
Few articles have focused on ASA classification and adverse events in ASD surgery; Somani et al 96 compared each ASA classifications in a database study of 5805 patients. Multiple logistic regression analysis revealed that ASA class Ⅳ was associated with any complication (OR 3.58, 95%CI 2.00-6.39), length of stay over 5 days (OR 3.34, 95%CI 1.91-5.84), pulmonary complication (OR 8.81, 95%CI 1.14-68.33), intra-/postoperative RBC transfusion (OR 2.52, 95%CI 1.37-4.62) and reoperation (OR 11.03 95%CI 1.42-85.61) compared to ASA class I. Similarly, Soroceanu et al also reported that ASA classification was a significant risk for medical complications (IRR 1.33, P = .01). 7
Charlson Comorbidity Index
The age of patients undergoing ASD surgery is increasing. Passias et al 97 reported that from 2003 to 2012, the CCI of patients undergoing ASD surgery increased from .77 to 1.44 (P < .001). Pitter et al 98 reported that CCI is a significant risk for prolonged hospital stay (CCI 1-2: OR 1.81 95%CI 1.29-2.54, CCI 3-9: OR 2.49, 95%CI 1.42-4.35) and readmission within 90 days postoperatively (CCI 1-2: OR 1.83 95%CI 1.20-1.29). Oe et al 11 reported significantly higher CCI in the malnourished group using PNI (CCI score .5 vs .3, P = .038). However, it is unclear which specific complications are associated with CCI, and which of the CCI components are independently associated with adverse events.
Management of Medical Complications
Reversible Factors
Significant Comorbidity for Medical Complications and Mortality.
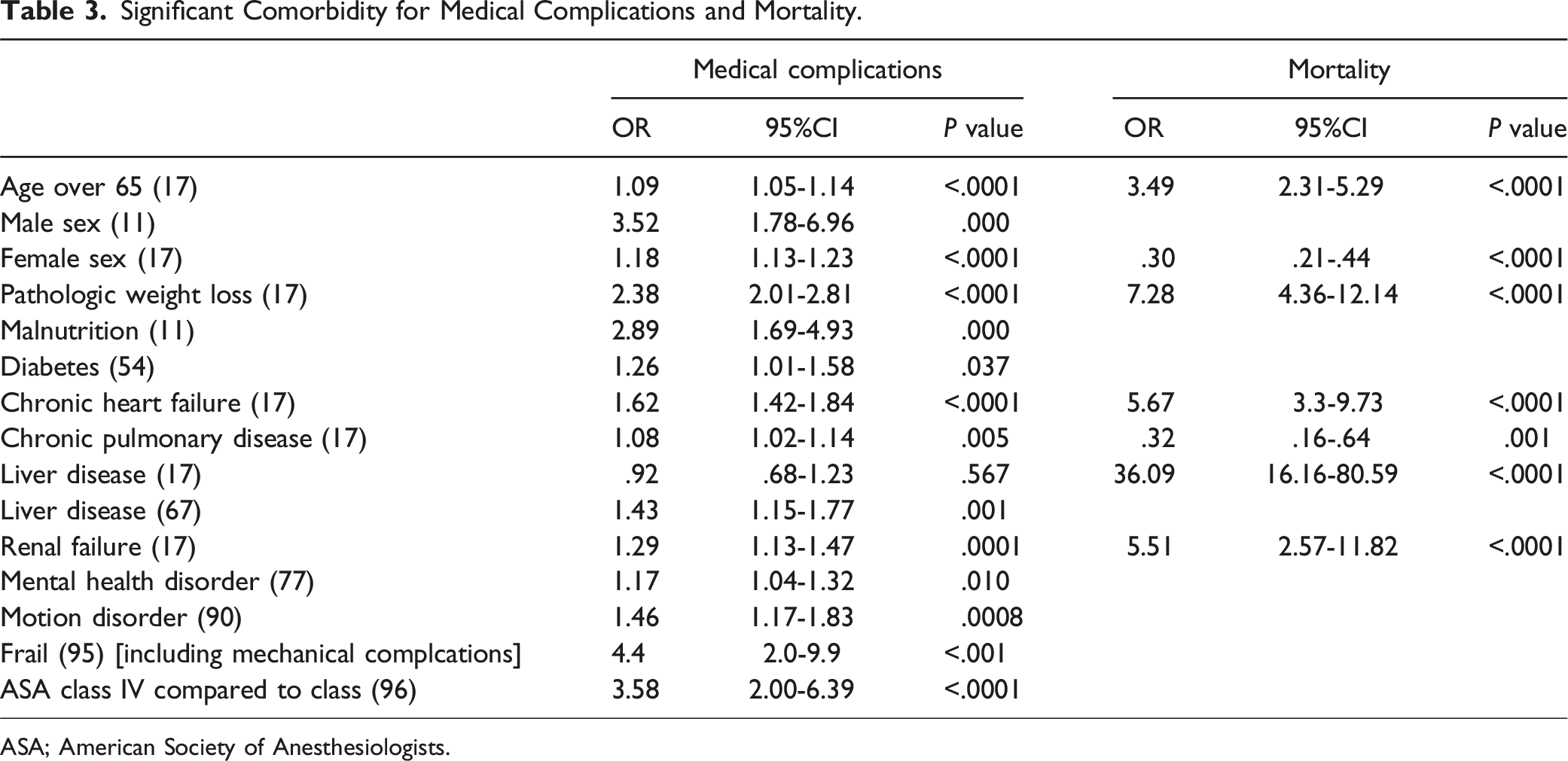
ASA; American Society of Anesthesiologists.
Evidence has been accepted for exercise therapy in spinal patients without neurological or other symptoms. 99 In addition, patients with spinal deformity were also recommended core strengthening exercise. Although not studied in ASD, preoperative resistance exercise interventions have been reported to be more beneficial to physical and mental status as well as clinical outcomes than perioperative or postoperative interventions. 100 Moreover, Oe et al reported that in a study of malnourished ASD patients, the incidence of medical complications was significantly lower in the group that received preoperative nutritional intervention (25% vs 53.6%). 101 The potential benefit of prehabilitation programs in patients undergoing ASD surgery has not been reported, and further work is needed to determine whether these programs can have a positive impact in the perioperative period.
Conclusion
With the increasing need for ASD surgery, it is important to determine factors that contribute to the high incidence of perioperative medical complications as well as to determine whether partially or fully reversing these factors can affect complication rates and outcome.11,12 Typical examples include smoking cessation, alcohol abstinence, weight management, nutritional intervention, exercise therapy, respiratory function training, and blood sugar control. Table 3 summarizes articles that calculated the odds ratios of significant comorbidities to medical complications using single or multiple regression analysis. High OR for medical complications were observed in males (OR 3.52), 11 pathological weight loss (OR 2.38), 17 malnutrition (OR 2.89), 11 frailty (4.4), 93 and ASA class IV (OR 3.58). 94 Similarly, for mortality, important risk factors included age >65 years (OR 3.49), morbid weight loss (OR 7.28), chronic heart failure (OR 5.67), liver disease (OR 36.09), and renal failure (OR 5.51). 17 Among these, nutritional status, glucose control and frailty can be improved preoperatively. Whether preoperative rehabilitation programs can impact the rate of adverse events and LOS has yet to be determined.
Limitation
While the majority of the references used in this study were from the year 2000 onwards, in certain instances, earlier references were included due to the limited availability of papers for evaluating specific risk factors. Consequently, no strict chronological restrictions were imposed. Furthermore, it should be noted that this paper provides a summary of relevant literature related to peri-operative morbidity, encompassing studies with varying patient backgrounds and statistical methodologies. To enhance the understanding of the risk-benefit ratio associated with ASD surgery, future research should consider prospective investigations into the peri-operative course, complications, and mortality rates for the risk factors presented in this study.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Shin Oe belong to donated fund laboratory called Division of Geriatric Musculoskeletal Health. It is supported by Medtronic Sofamor Danek Inc., Japan Medical Dynamic Marketing Inc., and Jyuzen Memorial Hospital.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This supplement was organized and financially supported by AO Spine through the AO Spine Knowledge Forum Deformity, a focused group of international Adult Spinal Deformity experts. AO Spine is a clinical division of the AO Foundation, which is an independent medically-guided not-for-profit organization. Support was provided directly through AO Network Clinical Research.