
Abstract
Background
Malnutrition is a prevalent issue among older patients with hip fracture and is significantly associated with poor outcomes. The Geriatric Nutritional Risk Index (GNRI) and Prognostic Nutritional Index (PNI) are nutritional screening tools that may assist in predicting outcomes in older patients undergoing hip fracture surgery. This study aimed to evaluate the effects of GNRI and PNI on 1-year mortality after hip fracture surgery in older patients.
Methods
This retrospective study included 577 patients aged 60 years and older with hip fractures treated surgically at a single center from January 2018 to December 2021. Nutritional status was evaluated using GNRI and PNI. The primary outcomes were 180-day and 1-year mortality, while secondary outcomes included short-term postoperative complications and length of stay. Univariate and multivariate analyses were performed to identify independent risk factors for 1-year mortality. Subgroup analysis was employed to identify potential population heterogeneity.
Results
Patients with low GNRI and low PNI had significantly higher 1-year mortality rates and short-term postoperative complication rates compared to those with higher scores. Low GNRI was an independent risk factor for one-year mortality (95% CI 1.09 - 3.25, P = 0.022). Subgroup analyses revealed significant heterogeneity, with males patients and patients with ASA III-IV showing higher hazard ratios for 1-year mortality associated with low GNRI. Pulmonary infections and older age were also identified as independent risk factors for one-year mortality.
Conclusion
This study demonstrated that low GNRI was the risk factor for 1-year mortality after hip fracture surgery in older patients.
Keywords
Introduction
Hip fracture is one of the most common orthopedic injuries.1,2 As the global population continues to age, the incidence of hip fractures is projected to nearly double over the next 20 to 30 years. 3 Due to substantial morbidity and mortality risks, hip fracture represents a significant health challenge in the older population.3-5 It is of great clinical significance to comprehensively assess the patient’s health status to screen out older patients with hip fracture who may have poor prognoses.
Malnutrition is prevalent among older patients with hip fractures. 6 Insufficient nutritional intake in older patients with hip fractures has been demonstrated to exacerbate their already compromised nutritional status. 7 Nutritional status is considered a critical factor of postoperative prognosis in older hip fracture patients.8,9 European Society of Parenteral and Enteral Nutrition (ESPEN) guidelines recommended early nutritional supplementation for all older patients after orthopedic surgery. 10
The geriatric nutritional risk index (GNRI) is calculated using serum albumin levels, actual body weight and ideal body weight. It was designed to predict the risk of nutrition-related complications and mortality in older patients who are hospitalized. 11 The GNRI has been demonstrated to be a predictor of outcomes in many diseases, including cancer, hemodialysis, and heart failure.12-14 The prognostic nutritional index (PNI) is an index that evaluates nutritional status by calculating serum albumin levels and absolute lymphocyte counts. The PNI was initially employed to evaluate the nutritional status of patients undergoing gastrointestinal surgery. 15 Furthermore, PNI has been demonstrated to be significantly related to the prognosis of various tumors.16-18
Nevertheless, few studies have examined the association between nutritional screening tools and postoperative mortality and complications in older patients after hip fracture surgery.19,20 The aim of this study was to evaluate the effects of GNRI and PNI on 1-year mortality after hip fracture in older patients and to investigate their relationship with short-term postoperative complications.
Methods
Study design and populations
This study included 577 patients aged 60 and above who had undergone emergency or elective surgery for hip fractures at a teaching hospital in a China’s eastern province between 1 January 2018 and 31 December 2021. The inclusion criteria were: (1) confirmed hip fracture and surgical treatment; (2) over 60 years old at the time of injury; (3) the time of admission was 2018.01 - 2021.12. Exclusion criteria were: (1) pathological and periprosthetic fractures; (2) conservative treatment; (3) loss of follow-up; (4) miss data. The flow diagram of patients enrolled in this study is shown in Figure 1 . The sample size should be at least 10 times the number of variables, and there were 20 variables in the current study, thus the sample size in this study should be at least 200.
21
This work has been reported in line with the “Strengthening the Reporting of Observational Studies in Epidemiology” ( STROBE ) checklist. (A) Flow Diagram of Patients Enrolled in this Study. (B) Survival Curves of Patients with High and Low GNRI. (C) Survival Curves of Patients with High and Low PNI.
Data Collection
The demographic characteristics, clinical characteristics, and laboratory test results of 577 patients were obtained from electronic medical records. The demographic data included age, gender (male and female), body mass index (BMI), and general health status according to the American Society of Anaesthesiologists (ASA) classification and comorbidities (consisting of hypertension, diabetes, and heart disease). Injury-related data included fracture type (femoral neck fracture or intertrochanteric fracture). The surgery-related data included type of anesthesia, duration of surgery, and type of surgery (THA, HHA, and internal fixation). Hospitalization data included laboratory tests on admission, time from admission to surgery, perioperative blood transfusion requirements, short-term postoperative complications (consisting of pulmonary infections, urinary tract infections, neurological complications, and cardiovascular or cerebrovascular complications) and length of stay (LOS). Investigators routinely followed up at 30 days, 90 days, 180 days, and 1 year after surgery by telephone interview or outpatient review. The follow-up data included patient survival status and date of death. The endpoint event was defined as either all-cause mortality or the conclusion of the study, whichever occurred first.
Definitions
The GNRI was calculated using the following formula: GNRI = [14.89×serum albumin level (g/dL)] + [41.7×actual body weight/ideal body weight]. The GNRI nutritional assessment level determination: high nutritional risk (GNRI ≤98) and low nutritional risk (GNRI >98). 11 The population was divided into the following two groups based on GNRI nutritional assessment level: the high GNRI group (GNRI ≤98) and the low GNRI group (GNRI >98). And the PNI was calculated using the following formula: PNI = serum albumin level (g/L) + 5×absolute lymphocyte count (109/L). 15 The PNI nutritional assessment level determination: high nutritional risk (PNI ≤ 38) and low nutritional risk (PNI > 38). The population was divided into the following two groups based on PNI nutritional assessment levels: the high PNI group (PNI ≤ 38) and the low PNI group (PNI > 38). Patients were divided into older (60 - 85) and super-older (≥ 85) groups based on age. Delayed surgery was defined as surgery performed more than 48 hours after the patient’s admission to the hospital. The American Society of Anesthesiologists (ASA) classification is divided into classes I-II and III-IV. Short-term postoperative complications were defined as complications that occurred during the hospitalization period and within 30 days of follow-up.
Outcome Measures
The primary outcomes of this study were 180-day mortality and 1-year mortality. The secondary outcomes included short-term postoperative complications (consisting of pulmonary infections, urinary tract infections, neurological complications and cardiovascular or cerebrovascular complications) and length of stay (LOS).
Statistical Analysis
The distributions of all continuous variables were evaluated for normality using the Shapiro–Wilk test. For variables that were normally distributed, the mean and standard deviation were used to represent the baseline characteristics of the patients. Median and interquartile range were used to represent variables with skewed distributions. Comparisons of characteristics between groups were conducted using appropriate statistical tests. The Student's t-test was employed for continuous variables with normal distributions, the Mann-Whitney U test for continuous variables with skewed distributions, and the chi-square test for categorical variables. Survival curves were calculated using the Kaplan-Meier method. Subsequently, univariate and multivariate analyses were used to further examine the independent influencing factors of 1-year mortality. Potential population heterogeneity was identified by examining interactions between low GNRI/low PNI and various subgroups. All statistical analyses were completed using R version 4.3.0 (2023-04-21). All descriptive studies were tested for significance using two-sided tests, and the significance level was P < 0.05.
Results
Characteristics and Outcomes of Patients in the Low and High GNRI Groups
Characteristics of Patients in the High and Low GNRI Groups.
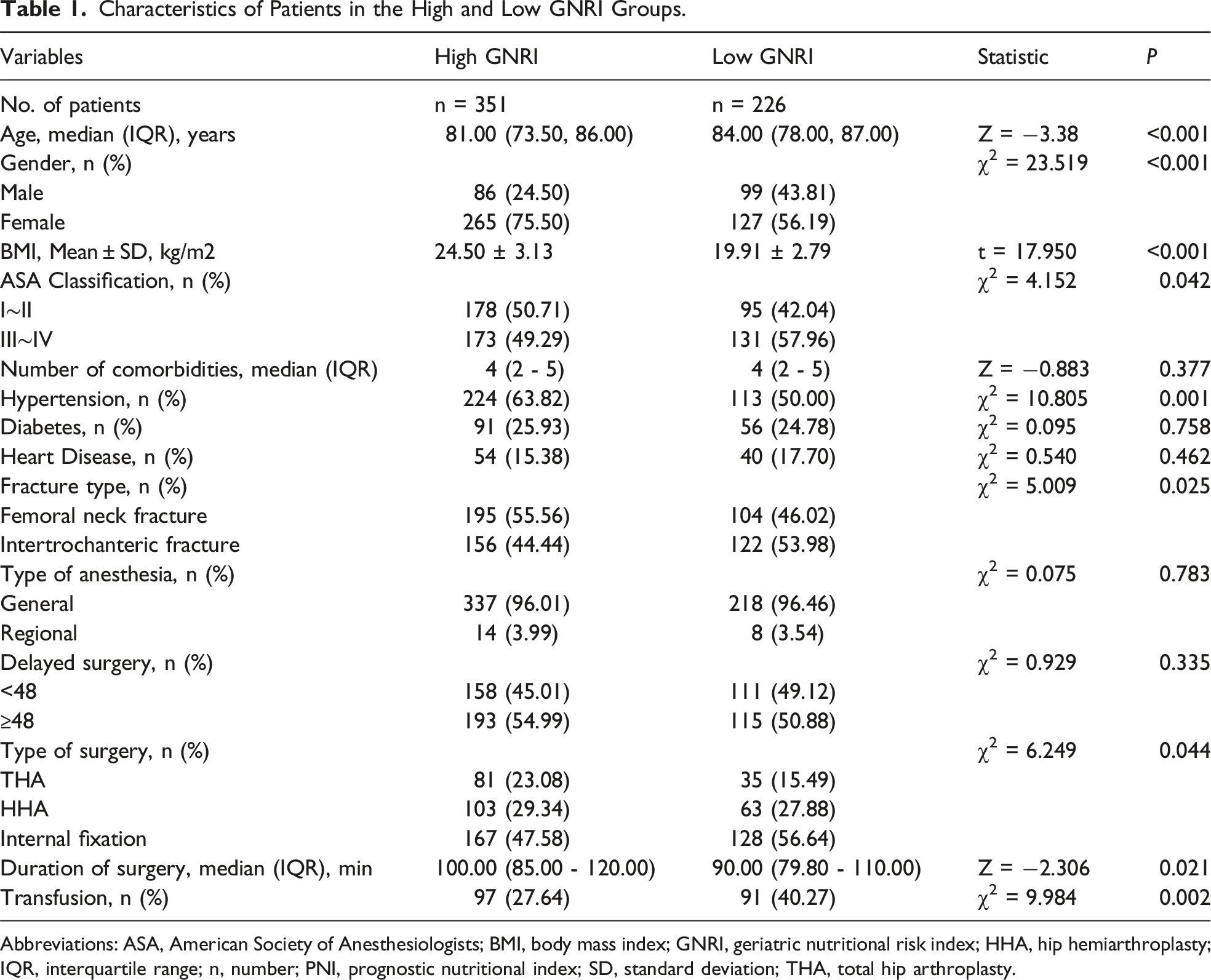
Abbreviations: ASA, American Society of Anesthesiologists; BMI, body mass index; GNRI, geriatric nutritional risk index; HHA, hip hemiarthroplasty; IQR, interquartile range; n, number; PNI, prognostic nutritional index; SD, standard deviation; THA, total hip arthroplasty.
Outcomes of Patients in the High and Low GNRI Groups.

Abbreviations: GNRI, geriatric nutritional risk index; IQR, interquartile range; LOS, length of stay; n, number.
Characteristics and Outcomes of Patients in the Low and High PNI Groups
Characteristics of Patients in the High and Low PNI Groups.
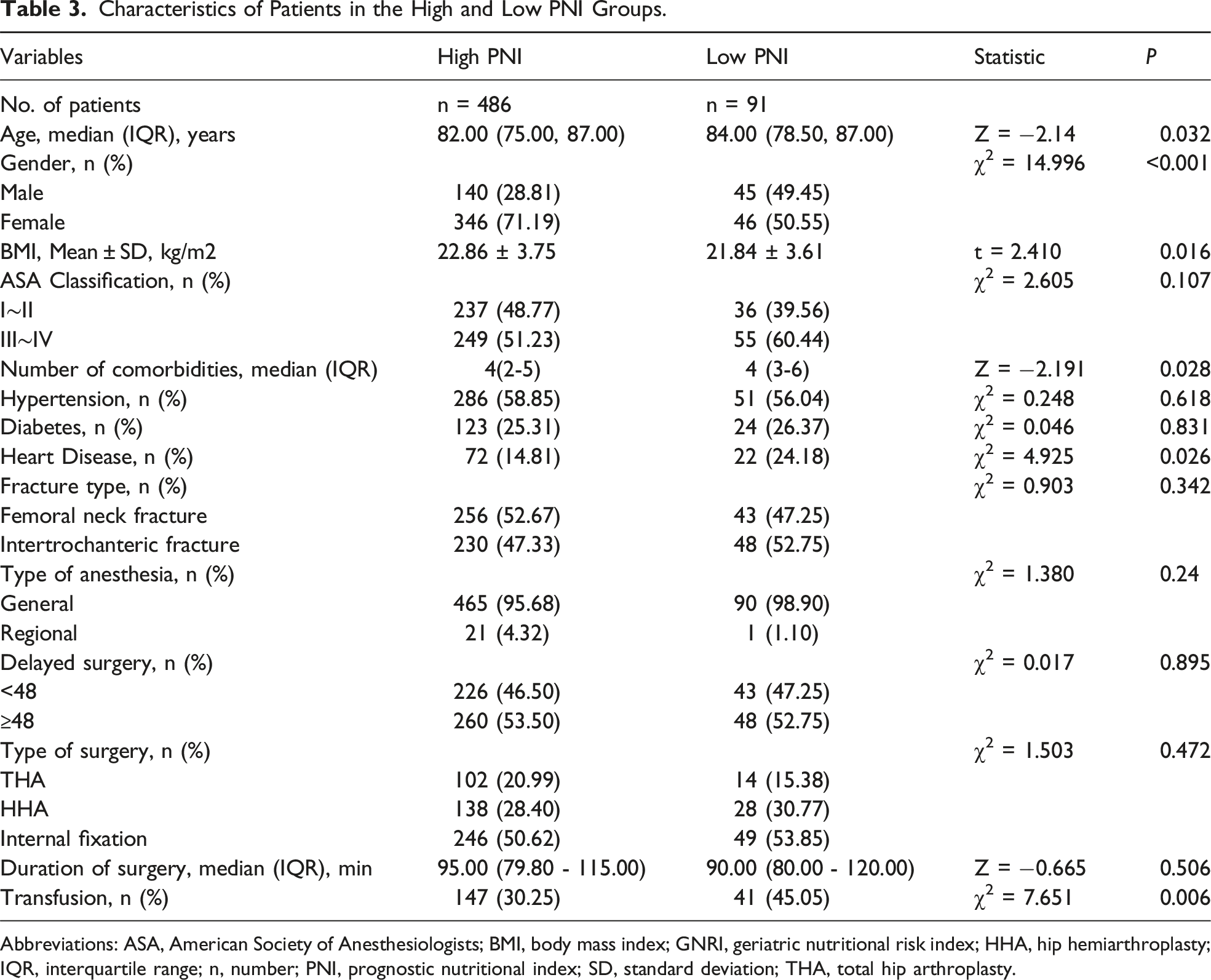
Abbreviations: ASA, American Society of Anesthesiologists; BMI, body mass index; GNRI, geriatric nutritional risk index; HHA, hip hemiarthroplasty; IQR, interquartile range; n, number; PNI, prognostic nutritional index; SD, standard deviation; THA, total hip arthroplasty.
Outcomes of Patients in the High and Low PNI Groups.
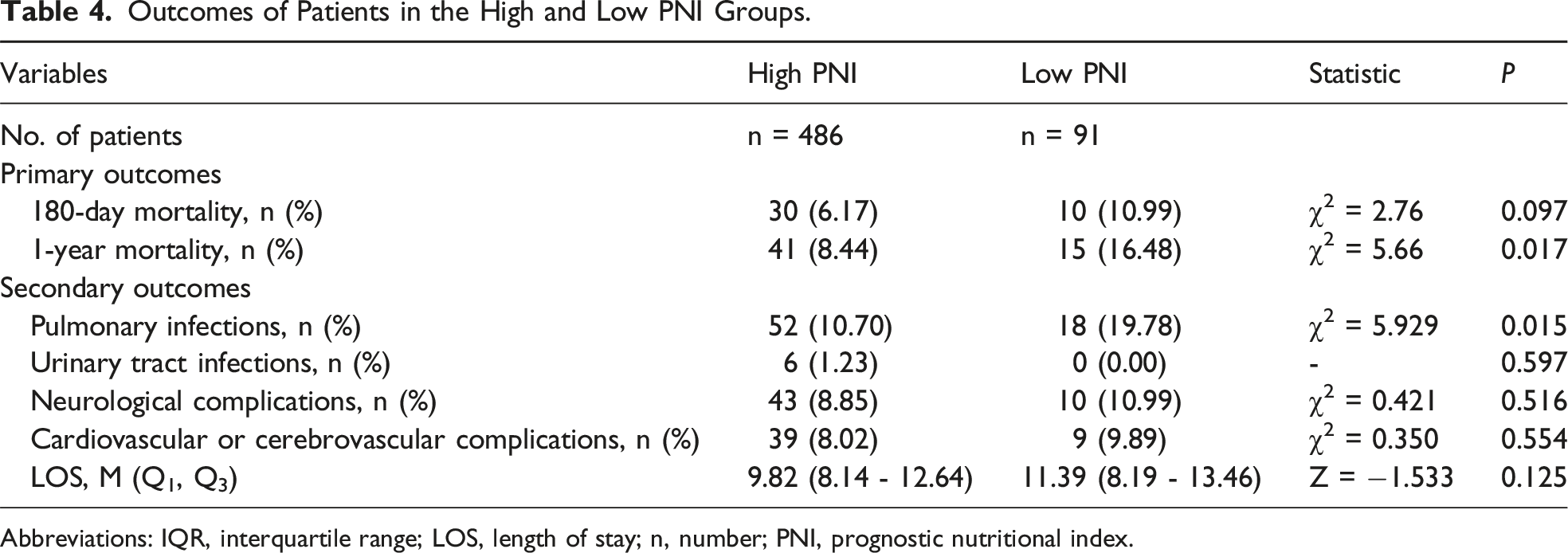
Abbreviations: IQR, interquartile range; LOS, length of stay; n, number; PNI, prognostic nutritional index.
Univariate Analysis of One-Year Mortality
Univariate Analysis of 1-Year Mortality.

Abbreviations: ASA, American Society of Anesthesiologists; CI, confidence interval; GNRI, geriatric nutritional risk index; HHA, hip hemiarthroplasty; LOS, length of stay; HR, hazard ratio; PNI, prognostic nutritional index; THA, total hip arthroplasty.
Multivariate analysis of one-year mortality
Multivariate Analysis of 1-Year Mortality (including Low GNRI).
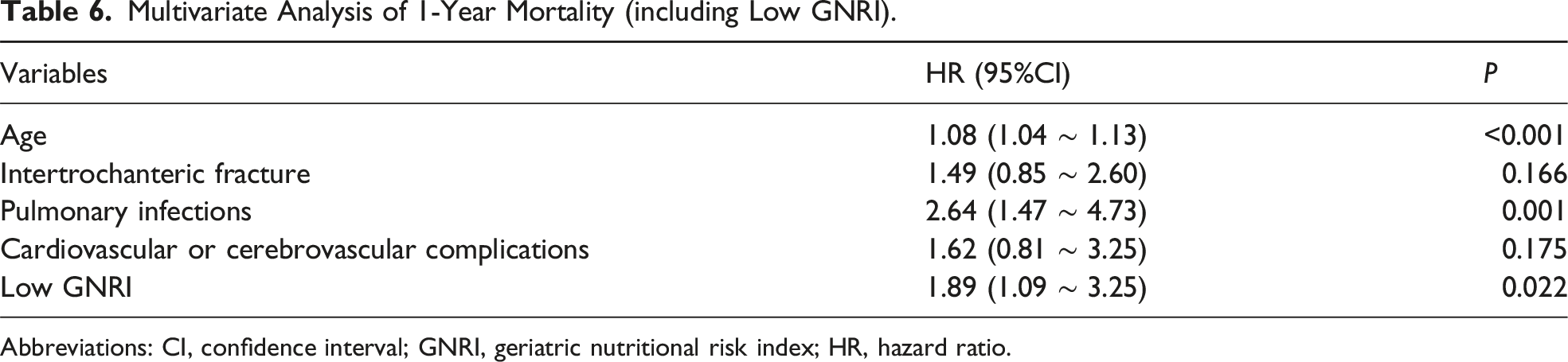
Abbreviations: CI, confidence interval; GNRI, geriatric nutritional risk index; HR, hazard ratio.
Multivariate Analysis of 1-Year Mortality (including Low PNI).

Abbreviations: CI, confidence interval; HR, hazard ratio; PNI, prognostic nutritional index.
Subgroup Analysis
The forest graphs showed the correlation between low GNRI and the risk of one-year mortality in different subgroups of age, sex, ASA classification, fracture type and delayed surgery. The results showed that in the subgroup analysis of low GNRI and one-year mortality risk, the HRs of the subgroups aged 60-85 years, male, ASA III-IV, femoral neck fracture, non-delayed surgery and delayed surgery remained significant with values of 2.71 (95% CI, 1.14 - 6.42), 10.23 (95% CI, 2.40 - 43.63), 4.25 (95% CI, 2.00 - 9.04), 3.61 (95% CI, 1.44 - 9.06), 2.40 (95% CI, 1.14 - 5.09), and 2.56 (95% CI, 1.19 - 5.53), respectively (Figure 2). Of these, significant interactions and increased risk estimates of one-year mortality associated with low GNRI risk were observed in the subgroups of male and ASA III-IV (P for interaction <0.05). The Association of Low GNRI with the Risk of 1-Year Mortality in Various Subgroups. ASA, American Society of Anesthesiologists; CI, Confidence Interval; GNRI, Geriatric Nutritional Risk Index; n, Number; HR, Hazard Ratio.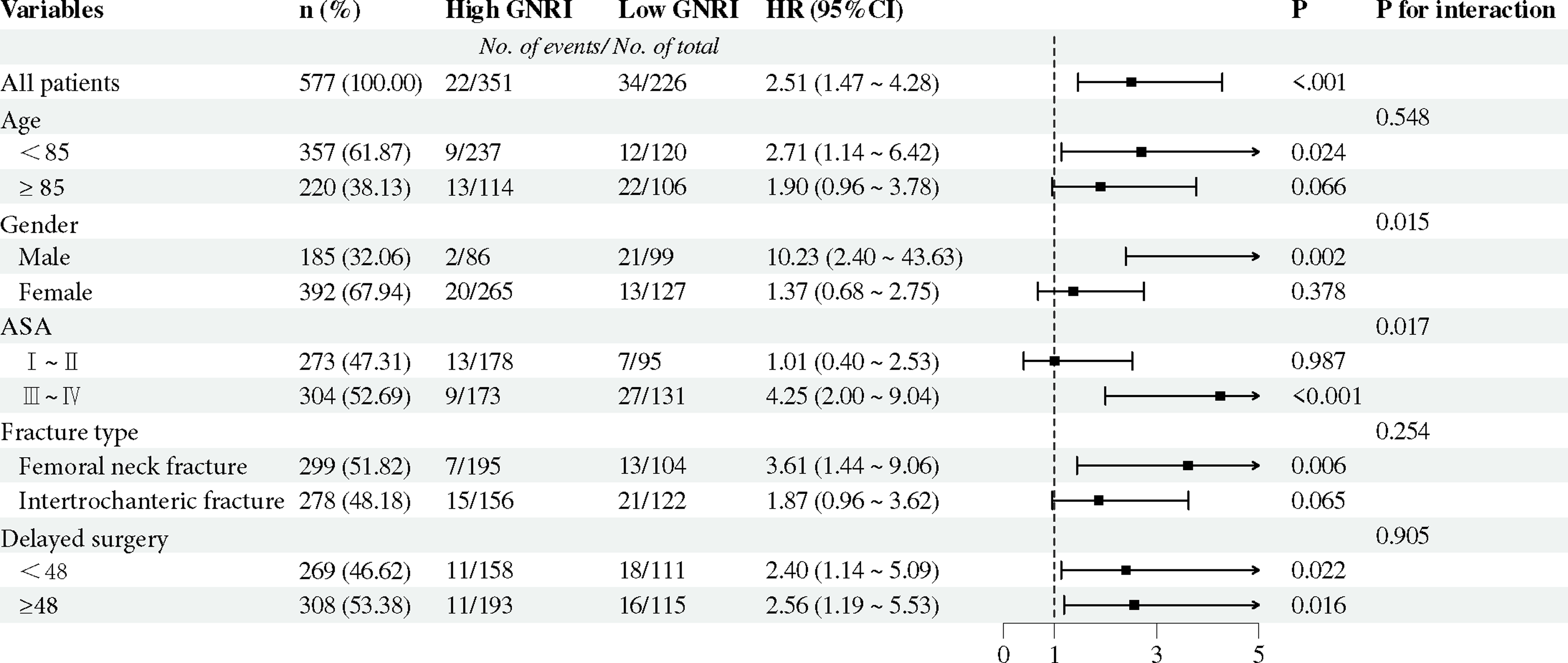
Discussion
Our current retrospective study found that patients with low GNRI and low PNI had significantly higher 1-year mortality rates and short-term postoperative complication rates compared to those with higher scores. Low GNRI was identified as the independent risk factor for 1-year mortality following hip fracture surgery in older patients. Additionally, subgroup analyses showed statistically significant heterogeneity were present in the subgroups of gender and ASA classification. These findings of this study indicated that enhancing nutritional status could serve as an effective preventive measure against mortality following hip fractures in the older population.
Malnutrition is a prevalent issue among older patients with hip fractures, and early detection of malnutrition is crucial to improving prognosis. 22 A variety of nutritional screening and assessment tools have been employed in an effort to achieve this objective among hospitalized patients. 23 This study demonstrated the advantages of utilizing GNRI and PNI to evaluate the nutritional status of older patients with hip fractures who are hospitalized. Firstly, the GNRI and PNI can be easily calculated using serum albumin level, weight, height and lymphocyte count. A meta-analysis demonstrated that serum albumin concentration and total lymphocyte count on admission were effective predictors of mortality in patients with hip fracture. 24 A study by Sheriff D. Akinleye et al. demonstrated that patients with hip fractures and low body weight exhibited a higher mortality rate. 25 Secondly, the simplicity and ease of use of GNRI and PNI enable medical teams to rapidly and accurately assess patients’ nutritional status, thereby enabling the timely formulation of personalized nutritional intervention plans and improving patient recovery and survival rates. Several studies have demonstrated that early surgical intervention within 48 hours of admission is beneficial for older patients with hip fractures.26-28 The rapid and convenient assessment of GNRI and PNI is well aligned with this requirement. Thirdly, GNRI and PNI employ objective body measurements and laboratory outcomes, which effectively mitigate potential biases associated with interviews and self-reports, such as recall and judgment errors. In contrast, the Mini-Nutritional Assessment Short Form comprises six items, including food intake, recent weight loss, mobility impairment, acute disease/stress, neuropsychological problems, and body mass index. 29 It is challenging for older adults to provide accurate health information. A review of 39 studies revealed a high prevalence of dementia and cognitive impairment among older adults with hip fractures. 30
The precise mechanisms underlying these findings remain to be fully elucidated. The GNRI and PNI are nutritional screening tools that typically indicate malnutrition when values are low. Numerous previous studies have consistently shown a clear association between malnutrition and poor outcomes after hip fracture, including an increased risk of complications and higher mortality rates.7,31 Reduced skeletal muscle mass and delayed bone healing may be the major causes. Malnutrition in the older adults is frequently associated with a reduction in protein intake, which is the fundamental component of muscle metabolism. 32 In patients who have sustained trauma, elevated protein catabolism during the stress response accelerates the loss of skeletal muscle amino acids, resulting in severe skeletal muscle atrophy. 33 The implications of this are particularly profound in the context of hip fracture recovery, where muscular strength and mass are integral to the restoration of mobility and independence. In addition, malnutrition has been identified as a significant risk factor for impaired bone healing. 34 The balance between osteoblastic bone formation and osteoclastic bone resorption is crucial for the process of bone repair. 35 L. Henry Goodnough et al found that chronic inflammation associated with aging can disrupt this balance. 36 This imbalance can result in ineffective healing of the bones following a fracture. Therefore, adequate nutrition is crucial for supporting the body’s natural healing processes and for improving the overall clinical outcomes for these patients.
The subgroup analysis revealed that significant heterogeneity and higher HR of low GNRI for 1-year mortality were observed in the subgroups of male and ASA III-IV. This indicated that focusing on and optimizing the nutritional status within these subpopulations might be especially critical in reducing the risk of mortality after hip fractures. With regard to the relationship between gender and mortality after hip fracture, a population-based prospective paired cohort study found that male hip fracture patients exhibited higher mortality than female patients in the first year after injury. 37 In the non-randomized intervention study by F. Reguant et al, patients with poorer health status, specifically those with ASA III-IV, showed that a multidisciplinary pre-surgical optimization could potentially reduce postoperative complications, hospital stay, and mortality. 38 These findings highlighted the necessity of targeted interventions focused on optimizing nutritional status in high-risk subpopulations to enhance outcomes and decrease mortality rates. Our study also found that older age and pulmonary infections were independent risk factors for mortality in multivariate analysis. This finding was consistent with the results of multiple previous studies.39-41
This study had several limitations. Firstly, this was a retrospective study, with all data sourced from a single centre. Consequently, the possibility of selection bias was higher than in multicentre studies. As the hospital participating in this study is university-affiliated and has a Level I trauma centre, it is possible that the included cases may have experienced severe fractures or had complex comorbidities. Secondly, this study did not consider the potential influence of dietary intake, psychological factors, physical activity, and medication use on patient outcomes. Thirdly, the sample size of this study was relatively small, and further prospective cohort studies are required to determine the effects of GNRI and PNI in older patients with hip fracture.
Conclusion
In conclusion, this study demonstrated that low geriatric nutritional risk index was the risk factor for 1-year mortality in older patients undergoing hip fracture surgery. Furthermore, increased risk estimates were observed in the subgroups of male and ASA III-IV, which underscored the importance of nutritional interventions for these populations. These findings suggest that timely nutritional assessment and intervention are essential for geriatric patients with hip fractures.
Footnotes
Acknowledgement
We thank all the participants included in this study.
Ethical Statement
This study was approved by the Ethics Committee of Zhongda Hospital Affiliated to Southeast University (2022zdsyl183-p01). Consistent with national laws and institutional protocols, written informed consent was not required from study participants.
Author contributions
Wei Wu, Huanyi Zhu, Yucheng Gao, Chuwei Tian and Chen Rui contributed to the data acquisition. Wei Wu and Huanyi Zhu conducted the analysis and interpretation of the data. Wei Wu and Xiangxu Chen drafted the initial manuscript. Wei Wu, Tian Xie, Liu Shi, Yingjuan Li and Yunfeng Rui provided substantial revisions to the manuscript. All authors read and approved the final manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Winfast Charity Foundation (YL20220525).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Due to data use agreements with the participating hospital, we are unable to provide the data used in this study.