
Abstract
Objective:
To investigate the neurological recovery of Frankel A spinal giant cell tumor (GCT) patients after they had received a Total En Bloc Spondylectomy (TES).
Materials and Methods:
We retrospectively recorded data of three patients (two females) with mobile spine GCT (T6, T10, and L2) Enneking stage III with complete paralysis before surgery, who had undergone TES in our institute from January 2018 to September 2020. The duration of neurologic recovery to Frankel E was the primary outcome. The intra-operative blood loss, operative time, operative-related complications, and the local recurrence were the secondary outcomes.
Results:
The duration of suffering from Frankel A to TES surgery was 2 months for the T6 patient, 3 weeks for the T10 patient, and 1 month for the L2 patient. Three patients had achieved full neurological recovery to Frankel E within 6 months after TES (T6 for 5 months, T10 for 3 months, and L2 for 3 months). The average blood loss was 2833.33 ml and the mean operative time was 400 min. Up until the last follow-up (13–25 months), no evidence of local recurrences had been found in any of the three patients.
Conclusion:
Frankel A spinal GCT patients can achieve full neurological recovery after TES, if the procedure is performed within 3 months after complete paraplegia. TES can effectively control any local recurrences.
Keywords
Introduction
Giant cell tumors (GCTs) are benign aggressive primary tumors of the spine. 1 They usually occur at the sacrum, but occasionally can be found in the mobile spine. 2 –4 Due to their aggressiveness and high rate of local recurrence, complete resection surgery, such as total en bloc surgery (TES), is the procedure of choice in mobile spine GCTs, especially for Enneking stage III. 1,5 –14 However, because of the rarity of these types of tumors, most of the published literature consists of case reports. Few studies have focused on neurological recovery after TES, especially in pre-operative Frankel A patients.
The aim of this study was to report on neurological recovery after TES in Frankel A Enneking stage III mobile spine GCT patients.
Materials and methods
This study was approved by the institutional review board of Khon Kaen University’s ethics committee. We retrospectively investigated mobile spine GCT patients who underwent TES in our institute from January 2018 to September 2020. The inclusion criteria were (a) mobile spine GCT, (b) Frankel A neurological status before surgery, and (c) Enneking stage III. The exclusion criteria were (a) having undergone another method of surgery, (b) inability to undergo surgery, and (c) involvement of vital neurovascular structures.
All patients underwent plain radiography at the region of the affected spinal level, whole spine MRI, and chest X-ray for disease staging.
All total en bloc spondylectomy procedures were performed by a single surgeon (P.P.). The operation was performed using the posterior-only approach as detailed by Yonezawa et al. in two patients (T6 and T10). 13,14 The combined anterior-posterior approach was used in one patient at the level of L2. The left side anterior retroperitoneal approach was used in order to cut the diaphragmatic crus. A titanium mesh cage was used for anterior column reconstruction, and spinal shortening was performed to tighten the cage and increase spinal blood flow.
Post-operation, patients were immobilized using an orthotic brace for at least 3 months or until solid bony union was observed on CT and X-ray images. We followed-up with a plain radiograph monthly until month 3, followed by a plain radiograph and CT scan of the spine every 3 months until 1 year, and then with a plain radiograph and CT scan every 6 months until a 2-year follow-up.
The primary outcome in this study was Frankel neurological status and the duration of recovery after TES. We also recorded the amount of intraoperative blood loss, operative time, complications, time to last follow-up or death, local recurrence, and distant metastasis as the secondary outcomes of this study. Complications were defined as iatrogenic dural tear, spinal cord injury, major vessel injury, irreparable pleural tear, and wound dehiscence or infection.
Results
Five mobile spine GCT patients were treated in our institutes from January 2018 to January 2020. Two patients were excluded, one of whom underwent extended curettage and posterior stabilization, and the other of whom had Frankel neurological status D before surgery. Three (two female) patients met our inclusion criteria, and their demographic data and outcomes are shown in Table 1.
Showed all information of Frankel A and Enneking III spinal GCT who underwent total en bloc spondylectomy.

Case no 1
A 57-year-old female was referred to our institute from another tertiary care hospital. She had experienced back pain and worsening neurological status for 6 months. At 2 months before being referred to our institute, her neurological status had gradually worsesed to Frankel A below the T6 spinal level. An MRI revealed Enneking stage III at T6 (Figure 1(A) and (B)). She underwent TES using the single posterior approach in our institute without any operation-related complications (Figure 1(C) and (D)). Her neurological status gradually improved to Frankel E at 5 months after surgery (VDO in Online Appendix). The patient then received Zoledronic acid intravenously every month without any further chemotherapy nor radiation therapy. She could not afford Denosumab because of the financial problem and the health policy from ministry of health. The three-dimensional reconstruction computed tomography at her last follow-up showed no local recurrence (Figure 1(E)). Her MRI images at the last follow-up also showed no local recurrence as shown in Figure 1(F).
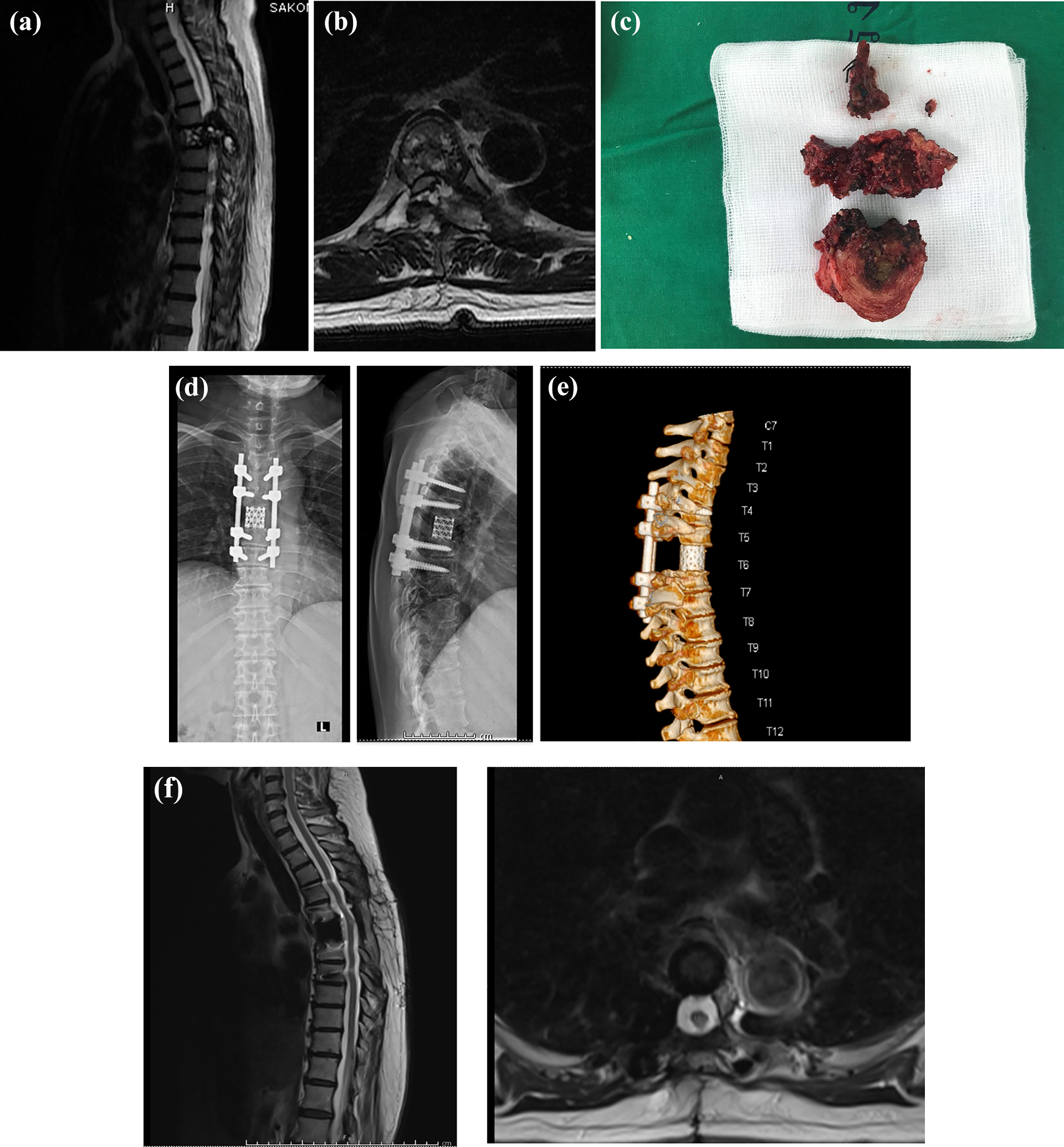
(A) The sagittal MRI showed Enneking III spinal GCT at T6 involved both anterior and posterior vertebral columns and nearly complete compression of the spinal cord. (B) Showed the axial cut of the MRI at T6 level. (C) Showed operative specimen of T6 Total En Bloc Spondylectomy. (D) Showed post-operative radiographic of this patient at the time of follow-up. (E) The three-dimension CT scan showed no radiographic osteolytic lesion around the TES level. (F) Demonstrated MRI at the last follow-up period.
Case no 2
A 35-year-old female was transferred to our institute because of rapid neurological deterioration to Frankel A after having undergone decompressive surgery for a spinal tumor at a provincial hospital 2 months earlier. The pathological report from the previous hospital revealed a GCT. The MRI before TES surgery showed an Enneking stage III GCT at T10 (Figure 2(A) and (B)). She underwent TES using the single posterior approach without any operation-related complications at our institute 3 weeks after developing Frankel A neurological status (Figure 2(C) and (D)). Three months after TES surgery, her neurological status had improved to Frankel E (VDO in Online Appendix). The MRI images at her last follow-up showed no local recurrence of the tumor (Figure 2(E)). As case no. 1, only Zoledronic acid was used for adjuvant therapy in this patient.
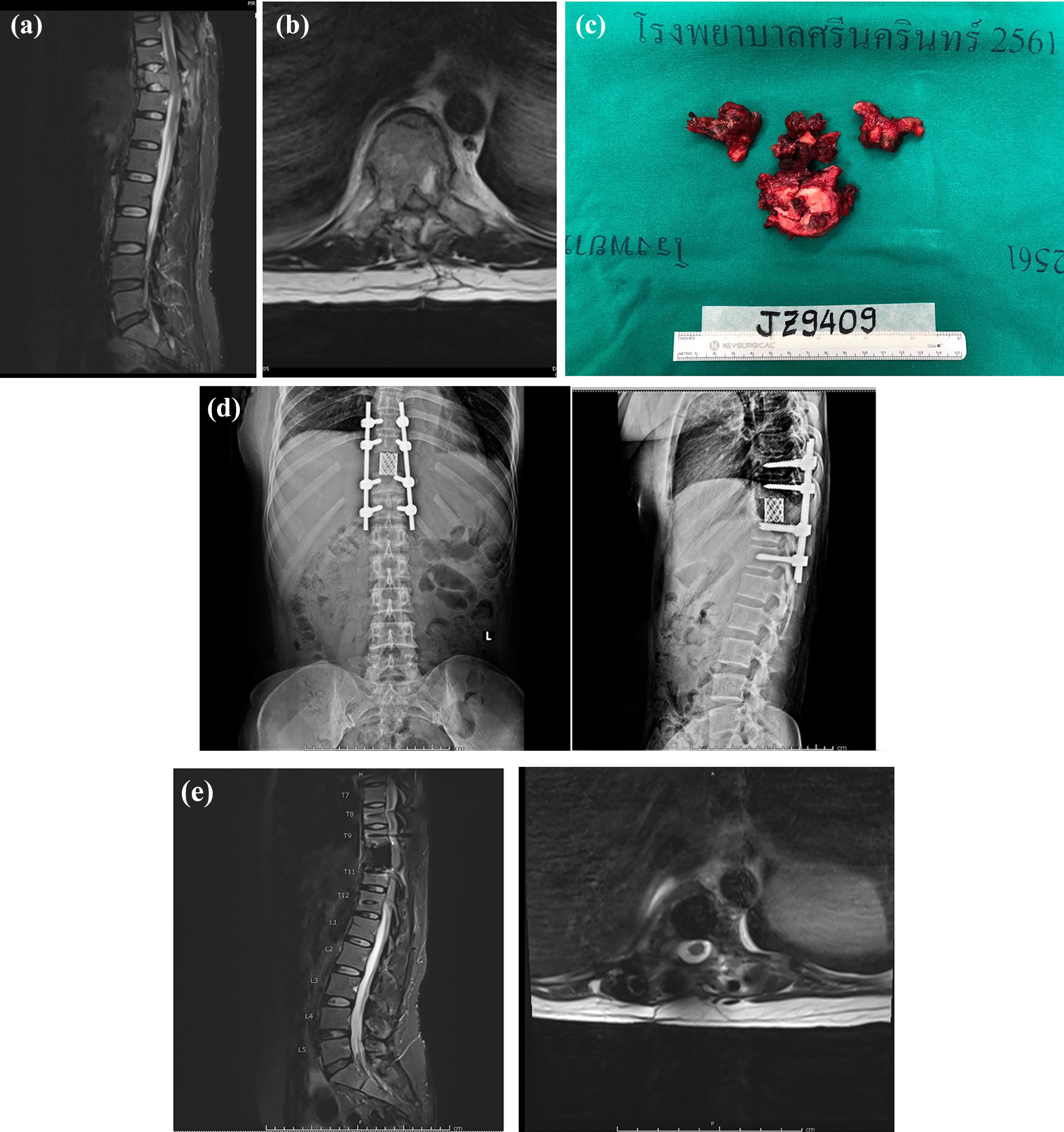
(A) Demonstrated the GCT of T10 spinal level and post-laminectomy procedure. (B) Showed axial cut of T10 level. (C) The Total en bloc spondylectomy specimen of this patient. (D) The follow-up plain radiograph of this patient. (E) Showed the last follow-up MRI of this patient.
Case no 3
A 27-year-old male was referred to our hospital from another tertiary care hospital. He had had severe lower back pain and Frankel A neurological status for 1 month. The MRI showed GCT at L2 with aggressive paravertebral extension (Figure 3(A) and (B)). Combined antero-posterior TES was performed without any operation-related complications, but a large amount of intra-operative blood loss (6000 ml). Figure 3(C) showed en bloc spondylectomy specimens and Figure 3(D) showed post-operative radiographic images. His neurological status gradually improved to Frankel E at 3 months post-operation (VDO in Online Appendix). At the last follow-up, the CT images showed no local recurrence of the tumor (Figure 3(E)). Same reason as case no. 1 and no. 2, Zoledronic acid was used monthly for adjuvant therapy without further chemotherapy nor radiation therapy.
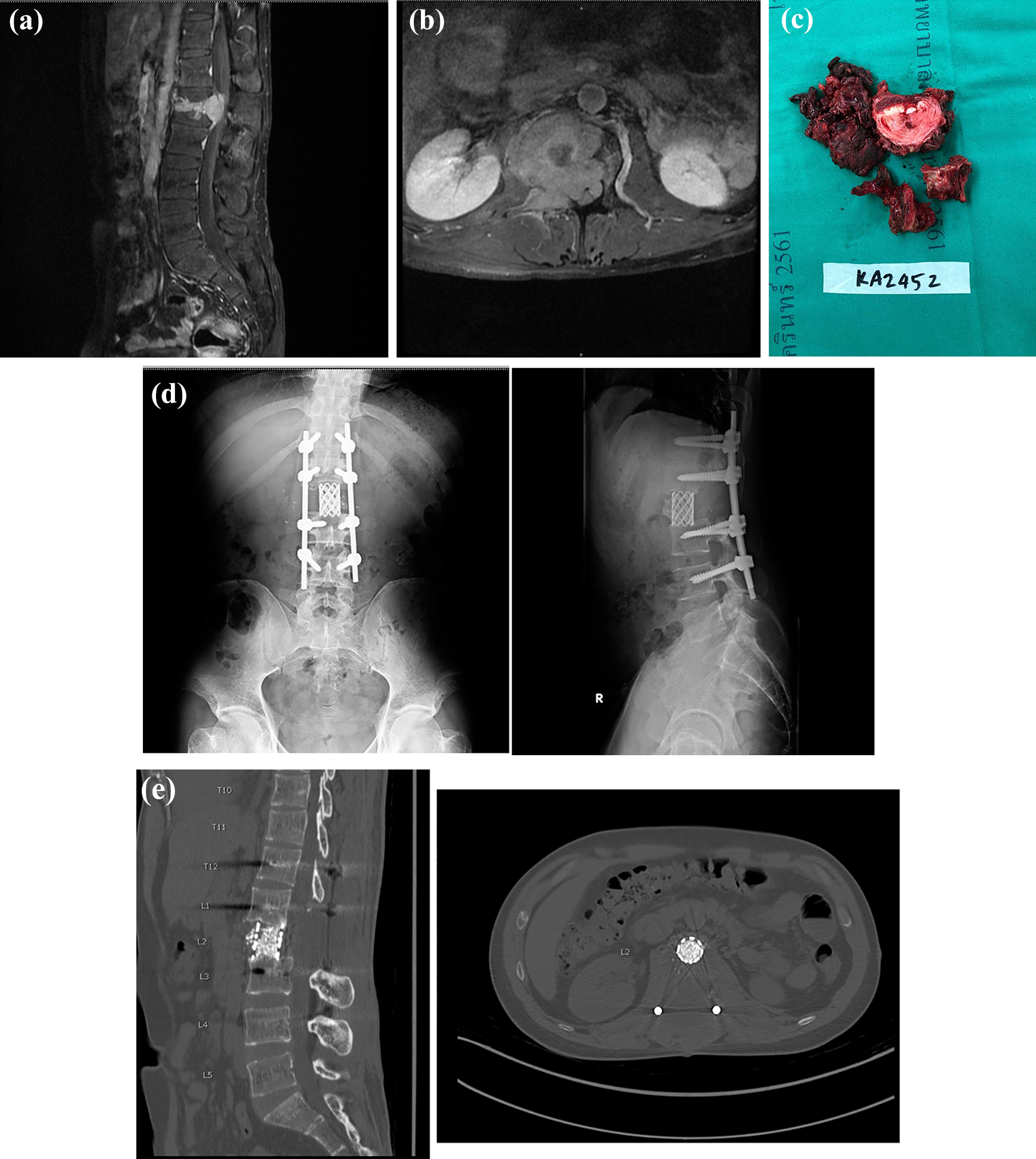
(A) The sagittal MRI showed the Enneking stage III spinal GCT at L2 level. (B) Showed extra-compartmental extension of the GCT at L2 level. (C) Total en bloc spondylectomy specimen of this patient. (D) Post-operative follows up plain radiograph of this patient. (E) Showed the CT scan of this patient at last follow-up.
Discussion
Spinal GCTs are very rare, accounting for only 2.7–6.5% of all musculoskeletal GCTs. 15 Most spinal GCT patients present with pain. 16 Up to 72% of patients with spinal GCTs may experience neurological deficits or radiculopathy. 11 Although new medication for treating this condition (Bisphosphonate and Denosumab) have been introduced, the mainstay of treatment is still total surgical removal, if feasible. 13,17 –20 The Spine Oncology Study Group recommends en bloc resection in spinal GCT patients. 21 Boriani et al. found a high rate of local recurrence after intralesional curettage, but that 90% of patients have a disease-free interval of at least 5 years if en bloc resection can be performed, especially in Enneking stage III patients. 1 A study of 12 patients with Enneking stage III mobile spine GCTs found that total en bloc spondylectomy (even intralesional pediculectomy) provided effective local disease control with no local recurrence based on a median follow-up time of 101 months. 14
In our study, we performed intralesional pediculectomy TES in all patients according to the procedure described by Tomita et al. 22 None of the three patients in our study have shown radiographic or clinical signs of local GCT recurrence, which supports the results of a study by Yokogawa et al. 14 However, this may be due to the short follow-up period (13–25 months) in our study, and a longer period may more accurately evaluate local recurrence in patients with Enneking stage III spinal GCT who undergo intralesional pediculectomy TES.
All of three Frankel A patients in our study demonstrated favorable recovery to Frankel E within 6 months after the operation. This is because none of the patients’ spinal cords were compressed longer than 3 months, meaning that blood flow was not permanently disturbed. 23,24 Regarding neurological recovery of spinal tumors patient after received spinal surgery, several literatures reported their neurological outcomes as followed. Li et al. 25 showed only 38.5% of complete paralysis spinal tumors patients recovered to neurological function of Frankel D or E. The study included all type of spinal tumors, both primary and secondary, which GCT only accounted for 17.9% and the study did not state clearly about type of spinal surgeries in each patient. The study of Quraishi et al. 26 and de Andrade et al. 27 demonstrated none of pre-operative Frankel A patients recovered to Frankel E after received operation. These studies recruited only metastatic spinal carcinoma and did not perform TES. Kurokawa et al. 28 studied 140 TES patients and showed ASIA impairment scale A patients still had neurological deficit for 1 year after underwent TES. This study included all type of spinal tumors including metastatic carcinoma and did not state the pre-operative and post-operative neurological status of 10 spinal GCT patients in the study. To the best of our knowledge, our study was the only study that report the full neurological recovery of Frankel A spinal GCT after received TES. The excellent neurological recovery results of our study could be explained by our patients were relatively young (less than 60-year-old). Age was considered one of the poor prognostic factors for neurological recovery after received surgery in spinal tumors patient. 25,27 The GCT was blood-rich tumor and had angiogenesis physiology. The neurological deficit from GCT may from mass compression predominantly rather than spinal cord infarction, which still provide a chance for spinal cord to recover after received en bloc tumor removal. 23,29 We thus recommend early TES for spinal GCT patients (within 3 months of development of Frankel A GCTs) to achieve spinal cord neurological recovery.
Our study had several limitations including (a) the small number of patients enrolled and (b) the follow-up period, which would be insufficient to detect local recurrence and distant metastasis.
In conclusion, TES can lead to complete neurological recovery in Frankel A Enneking stage III spinal GCT patients if it is performed within 3 months. In addition, intralesional pediculectomy TES might be able to effectively control local disease recurrence. Studies in more patients and with longer-term follow-ups are needed to further clarify these clinical outcomes.
Footnotes
Acknowledgements
The authors thank the patients for participation, the Department of Orthopaedics, Faculty of Medicine, and Musculoskeletal Oncology and Spinal Disorder Research Group, Khon Kaen University for support.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was granted by Faculty of Medicine, Khon Kaen University, Thailand (MN63305) and supported by Research and Graduate Studies, Khon Kaen University.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.