
Abstract
Study Design:
Retrospective cohort study.
Objective:
We aimed to evaluate the improvement in neurological deficit following early versus late decompression and stabilization of thoracolumbar junctional fractures.
Methods:
This is a retrospective evaluation of all patients with a traumatic spinal cord injury (SCI) from T11 to L2 treated at a teaching hospital between 2010 and 2017. Grouped analysis was performed comparing the cohort of patients who received early surgery within 24 hours (group 1) with those operated within 24 to 72 hours (group 2) and more than 72 hours after SCI (group 3). The primary outcome was the change in ASIA (American Spinal Injury Association) motor score at 12-month follow-up.
Results:
There were 317 patients (225 males and 92 females with mean age of 31.55 ± 12.43 years). A total of 144, 77, and 96 patients belonged to groups 1, 2, and 3 respectively. Improvement of at least 1 grade on ASIA classification was observed in 80, 45, and 33 patients in groups 1, 2, and 3 respectively (P = .001). Overall, 32, 12, and 10 patients improved ≥2 grades on ASIA classification in groups 1, 2, and 3, respectively (P = .069). On logistic regression analysis, early surgery and severity of initial injury (complete [ASIA A] vs incomplete SCI [ASIA B-D]) were found to significantly influence the potential for neurologic improvement (P = .004 and P < .0001, respectively).
Conclusion:
We believe that the earlier the decompression, the better. The 72-hour cutoff represents the most promising time window during which surgical decompression has the potential to confer a neuroprotective effect in the setting of incomplete SCI (ASIA B-D) in the distal region of the spinal cord (conus medullaris).
Keywords
Introduction
The role and timing of surgical decompression after an acute spinal cord injury (SCI) remains one of the most controversial topics in spine surgery because of the absence of well-designed and well-executed randomized controlled trials. 1 Predicting neurologic improvement is a complex process; there is only sparse literature detailing neurologic improvement, particularly after thoracic and lumbar (conus) SCIs. 2 Some studies report no difference in neurological outcome in early versus late stabilized spinal fractures, 3 -5 while other studies report a significantly better neurological outcome in early-operated patients. 1,6 -10
The likelihood and degree of neurologic improvement after surgical decompression and stabilization after traumatic SCI is influenced by the anatomic region as well as degree of spinal injury. The effect of early surgery for complete traumatic SCI (ASIA [American Spinal Injury Association] A, ie, where neither motor nor sensory function is preserved at the most caudal level below the lesion) is generally believed to be poor. 11 A recent survey of spine surgeons showed a trend toward delaying surgical decompression in complete SCI compared with incomplete SCI. 12,13
Upper thoracic SCI are more often complete with less potential for meaningful neurologic improvement believed to be due to the tenuous blood supply in this region as well as the high-energy mechanism needed to create an injury due to the stability of the chest wall and spinal column in the region. On the contrary, in the thoracolumbar region of the spine, the unique anatomy of conus medullaris with greater proportion of lower-to-upper motor neurons in the distal spinal cord combined with capacious medullary canal offers a distinct advantage of better chances of neurological recovery compared to upper spinal cord. This tendency of the lower motor neurons at the site of an SCI to recover is referred to as root escape. 2 The purpose of this study was to evaluate neurological recovery following inadvertent delayed decompression and stabilization of the thoracolumbar spine fractures and compare outcomes with patients in whom early decompression was achieved.
Patients and Methods
Over an 8-year period between January 2010 to December 2017, 376 patients with spinal injuries were seen, evaluated, and treated at the Ghurki Trust Teaching Hospital, Lahore, Pakistan. Patients were included in the analysis if they met the inclusion criteria of a non-penetrating traumatic SCI (ASIA A–D) at the thoracolumbar junction (T11 to L2), age more than 14 years, with complete initial and 1-year ASIA examinations. Fifty-nine patients were lost to follow-up and were therefore excluded from analysis. Final analysis was performed on 317 patients. Magnetic resonance imagings (MRIs) were used to confirm that the involved segment had cord involvement, as opposed to the cauda equina. Excluded from analysis were cauda equina, peripheral nerve injuries (lumbar plexus), and cases, where physical examinations were not reliable because of concurrent injuries (ie, closed head injury). Patients with fractures involving L3 to L5 level were also excluded. As our study was retrospective in nature and did not influence patient care, the need for ethical approval was waived by institutional review board.
Initial examinations on admission as well as sequential follow-up examinations were performed and recorded using the ASIA grading system. As per institutional policy, intravenous steroids were not administered to any patient. Patient records were maintained in an institutional review board–approved SCI database. Specific data points for gender, age, location of neurologic injury, functional grade, etiology of injury, and mortality rate were documented.
All patients were evaluated with plain radiographs, computed tomography scans, and MRI to ascertain the amount of retropulsion of bony fragments into the spinal canal, status of posterior elements, and pedicles of the adjacent vertebrae. All patients underwent posterior short segment fixation (with pedicle screws one level above and below the fractured vertebra) and decompression and posterolateral fusion. Fracture level may or may not have been included in the fixation, depending on the fracture pattern and integrity of the pedicles, which was decided intraoperatively by the surgeon. A mechanical distractor was used to perform indirect ligamentotaxis in an attempt to reduce the retropulsed fragments, and transpedicular decompression was carried out in all cases. Prophylactic antibiotics of a second-generation cephalosporin were initially used for 5 days postoperatively. A thoracolumbar orthosis was prescribed to all patients postoperatively for approximately 3 months.
Neurologic examinations were performed on admission, immediately after surgery, and at 1, 3, 6, and 12 months. The primary outcome measure was the change in ASIA grades. The ASIA grade is a 5-point ordinal scale, classified from A to E, to categorize motor and sensory impairment in individuals with SCI.
Patients were separated into 3 cohorts, depending on the timing of surgical decompression relative to the injury. The early-surgery cohort consisted of patients who underwent surgery within 24 hours of injury (group 1), intermediate group of patients whose surgery was done within 24 to 72 hours of injury (group 2), and the late-surgery cohort consisted of patients who underwent surgery after 72 hours of injury (group 3). Group assignment was primarily dependent on time elapsed between injury and presentation in indexed hospital. As per hospital’s policy, an attempt is made to operate all patients within 12 hours of admission.
All statistical analyses were performed using SPSS version 21 (IBM Corp, Armonk, NY). Student’s t test was used for statistical analysis of continuous variables. Mean values are presented as the mean ± SD. Chi-square test was used for quantitative data. Significance level was set at P < .05.
Results
During the 8 years of analysis, 317 patients underwent surgical decompression and stabilization at our institute. Mean age was 31.55 ± 12.43 years with male preponderance (71%). A total of 144 patients were operated upon within 24 hours of injury (group 1) whereas 77 and 96 patients belonged to the 24-72 hours (group 2) and more than 72 hours (group 3) categories. Table 1 shows patient characteristics across groups. There were no significant differences in sex, age, causes of injury, and ASIA grade at admission.
Demographic Profile of Patients Across Groups.
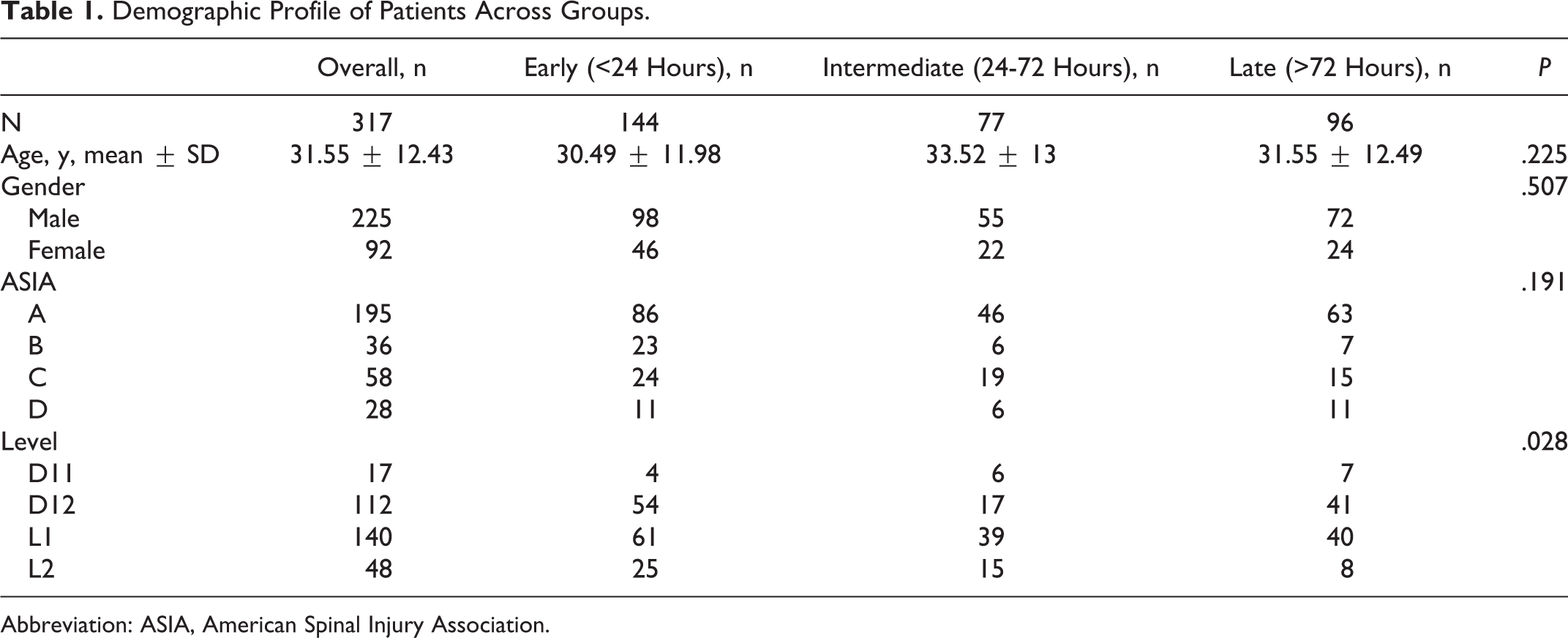
Abbreviation: ASIA, American Spinal Injury Association.
The neurologic recovery of patients was evaluated 12 months after surgery. The details of the ASIA grade on admission and during follow-up are shown in Table 2. The details of ASIA grade improvement in each subgroup are shown in Table 3. In the early group, 80 patients improved their ASIA score by 1 grade or more. Similarly, 45 and 33 patients improved their ASIA score by 1 grade or more in the intermediate and late groups (P = .001). Difference in neurological recovery was most pronounced in the early-operated patients. ASIA B and C subgroups support this result. The ASIA A subgroup approached but did not reach statistical significance (P = .176), In the early group, 32 patients had ≥2 grade ASIA improvement, compared with 12 and 10 patients in the intermediate and late groups, respectively. This difference was just shy of statistical significance (P = .069). On logistic regression analysis, early surgery and severity of initial injury (complete [ASIA A] vs incomplete SCI [ASIA B-D]) were found to significantly influence the potential for neurologic improvement (P = .004 and P < .0001, respectively).
Correlation Between Preoperative and Postoperative ASIA Classification.
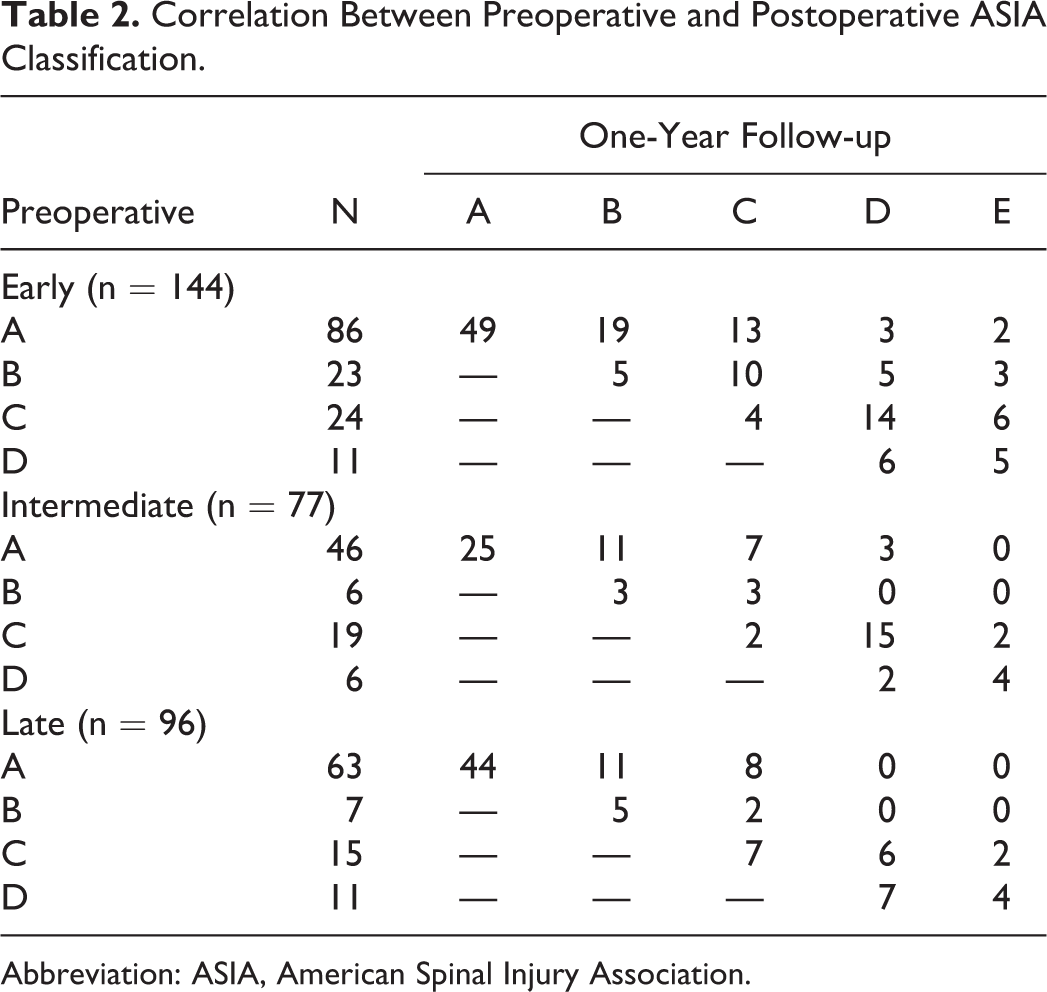
Abbreviation: ASIA, American Spinal Injury Association.
ASIA Impairment Scale Grade Improvement Measurement at 12 Months.
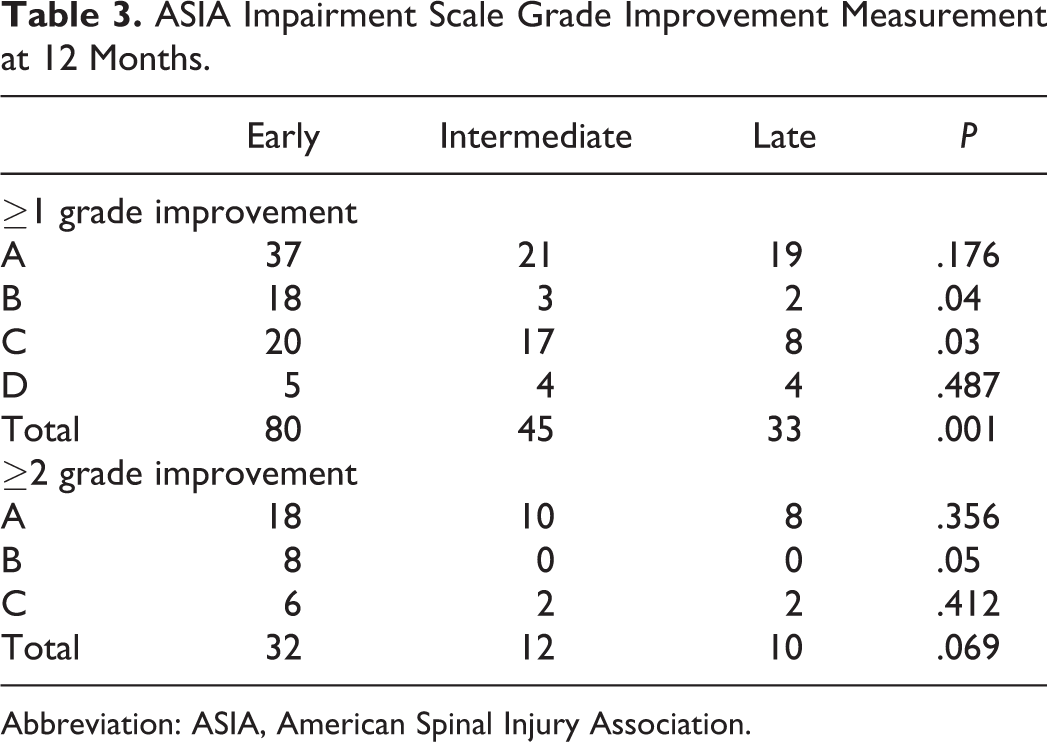
Abbreviation: ASIA, American Spinal Injury Association.
Discussion
The thoracolumbar junction represents the most common level for spinal fractures. 14 Despite its frequency, evidence regarding the timing of decompression in the specific setting of a thoracolumbar junction fracture with a neurologic deficit is sparse. Hence, a recent publication by the German Society for Orthopaedics and Trauma that performed a systematic review on the treatment of thoracolumbar fractures concluded, “There are no clear recommendations regarding the best time to carry out an operative procedure.” 15 One reason for the paucity of literature on timing of decompression for thoracolumbar injuries from T11-T12 to L1-L2 may be due to the admixture of the cell bodies in the conus medullaris and lower motor neuron axons of the cauda equina, both of which may have different pathophysiology and recovery potential. 2 The purpose of our study is to determine the influence of timing of surgical decompression/stabilization on MRI-verified spinal cord injuries at the thoracolumbar junction (T11 to L2) in adult patients. To our knowledge, this is the largest study to date focusing on acute spinal cord injury at the thoracolumbar junction. In the present study, an attempt was made to operate on all patients within 12 hours of admission. Only a minority of patients had polytrauma and required hemodynamic stabilization before surgery. In the majority of cases, the delay was caused by the time elapsed between the injury and presentation at a hospital. Facilities for spinal surgery are not widely available in Pakistan. Our hospital is the first and largest spine center in Pakistan and receives patients from all over the country, which results in inadvertent delay in surgical treatment.
We found that some degree of spinal cord recovery was seen in 49.8% of the patients who underwent surgical intervention. We found that a significantly greater proportion of patients who improved at least one ASIA grade were operated within 72 hours of SCI. The percentage of patients showing neurological recovery (≥1 grade in power on ASIA scale) did not appear to differ whether patients were operated within 24 hours or within 24 and 72 hours (55.5% vs 58.4%, P = .680) but dropped significantly to 34.3% after 72 hours. The difference in proportions of patients who improved 2 ASIA grades between the early, intermediate and late groups was just shy of statistical significance (P = .069) and may have reached significance with greater numbers. On subgroup analysis, 77 out of 195 patients with ASIA A SCI showed at least 1 grade improvement. However, timing of surgery did not influence neurological recovery in this subgroup. In patients with incomplete neurological deficits (ASIA B-D) at initial presentation, 81 out of 122 patients showed at least 1 grade improvement in neurologic function, with timing of surgery significantly influencing rate of neurological recovery. Our results suggest that neurological recovery can still be expected in about one-third of patients (34.4%) who present 72 hours after injury. While the efficacy of surgical intervention could not be determined in the absence of a control (nonsurgical) group, it would be unethical to have such a control.
None of our patients received steroids. The fact that none of our patients in the current study received intravenous steroids further highlights the positive impact of early surgical decompression on the chances of neurological recovery. Intravenous steroids for SCI remain a contentious topic. A recent systematic review published by Fehlings et al 16 in 2017 concluded that there was moderate evidence that the 24-hour NASCIS II (National Acute Spinal Cord Injury Studies) methylprednisolone regimen has no impact on long-term neurological recovery when all postinjury time points are considered. However, there is also moderate evidence that subjects receiving the same methylprednisolone regimen within 8 hours of injury achieve an additional 3.2 points of motor recovery compared with patients receiving placebo or no treatment. A possible explanation for this inference may be a synergistic neuroprotective effect from a combination of steroids and early surgery, as was also observed in the STASCIS study. 17 In a survey of 2659 spinal surgeons, 1198 opted to use steroids in acute SCI. However, 40.3% considered steroid therapy as “optional,” whereas only 18.3% considered it as “recommended.” 18
The concept of early surgery evolves around avoidance of secondary damage to the spinal cord. Multiple cutoffs for early surgery have been reported in the literature; ranging from surgery within 8 hours 1 to ≤24 hours 19 and ≤72 hours from injury. 5 Wilson et al 20 recently published a systematic review to evaluate the impact of timing of decompression in acute spinal cord injury. Their review included 6 studies. 7,17,19,21 -23 . One study focused on cervical cord injury 17 and another on acute central cord syndrome without instability. 23 One randomized, controlled trial exclusively included patients with thoracolumbar cord injury. 19 Studies by Bourassa-Moreau et al, 22 Dvorak et al, 21 and Wilson et al 7 included spinal cord trauma ranging from cervical to lumbar region. These studies have reported the influence of surgical decompression on neurological recovery without correlating the results with specific spinal cord segments, that is, cervical, thoracic, or lumbar. The review concluded that early decompression, compared with late surgery, may lead to clinically important improvements in neurologic status in patients with cervical injury; however, this was based on a single study and strength of evidence was rated as low. Evidence was very low across 2 studies in populations with mixed injury levels (cervical, thoracic, and lumbar) that early, compared with late, surgical decompression was statistically associated with clinically important neurological improvement at the time of discharge from inpatient rehabilitation (1 study) and in patients with incomplete SCI (1 study). 20
Bourassa-Moreau et al 12 evaluated the impact of early surgical decompression (<24 hours) on neurological recovery in 53 patients with complete (ASIA Impairment Scale A) SCI. Out of 33 patients with thoracolumbar SCI, only 6 patients had neurological improvement (4 out of 24 patients operated within 24 hours improved whereas 2 out of 9 patients operated after 24 hours improved). The authors concluded that timing of surgery did not influence neurological recovery in patients with thoracolumbar SCI (P = .99). These results are somewhat consistent with our findings. Neurological recovery for early-operated patients with ASIA A SCI approached but did not meet statistical significance (P = .179), However, we report 1 grade neurological improvement in 39.4% of such patients compared to 18.2% improvement reported by Bourassa-Moreau et al. 12 An argument can be made to attribute this higher rate of neurological recovery in complete SCI patients (ASIA A) to abatement of spinal shock rather than an effect of early decompressive surgery. Studies by Furlan et al 24 and Maynard et al 25 have shown that neurological examinations performed within the first 24 hours after SCI are valid and consistent with examination results obtained at 72 hours postinjury, except among patients with an associated traumatic brain injury. Based on recent evidence, spinal shock is now thought to represent an ongoing physiologic continuum consisting of 4 stages, occurring in virtually all patients with severe SCI, beginning within minutes after injury and continuing for up to 12 months. 26 Therefore, it may be inappropriate to identify an SCI patient as being “in” or “out of” spinal shock (based on the presence or absence of bulbocavernosus reflex) for purposes of classification within a study.17 We attribute the higher rate of neurological recovery in complete SCI to the unique anatomy of the conus medullaris, which has a greater mixture of lower to upper motor neurons and hence better chances of recovery.
In their randomized controlled trial on 27 patients with thoracolumbar SCI between T8 and L2, Cengiz et al 1 found that 10 out of 12 patients operated within 8 hours of injury improved. In contrast, in patients in whom surgery was delayed for 3 to 15 days, only 4 out of 15 patients showed neurological improvement. Interestingly, out of 6 initial ASIA A grade patients operated within 8 hours, 1 improved by 1 grade, 1 by 2 grades, and 2 by 3 grades, and 2 remained unchanged. In ASIA A patients who received delayed surgery only one out of seven patients improved by 1 grade. Similarly, we have reported that 39.4% patients with ASIA A showed neurological improvement. These findings indicate that patients with complete SCI may have the most to gain from early decompression, which is contrary to the bulk of published literature which favors delaying surgical decompression in complete SCI patients. These findings are contradicted by results of a randomized, controlled trial conducted by Rahimi et al 19 on 35 patients involving T5-L1 SCI. They defined early group as surgery performed within 24 hours. In patients with ASIA A paraparesis, 1 out of 6 patients in early surgery group and 1 out of 9 patients in the late-surgery group showed improvement of 1 grade on the ASIA scale. However, because of the small numbers involved, this was likely an underpowered study.
Controversy exists on the safety of surgery within the first 72 hours after an acute SCI. 27 McLain and Benson, 28 Kerwin et al, 29 and Croce et al 30 report a similar mortality in early and late procedures for thoracic or lumbar fractures. Kerwin et al 29 report a trend to a higher mortality, but only in the early treatment of cervical spine fractures. Since none of the studies report a higher mortality in early-operated patients with thoracic or lumbar fractures, we can conclude that early surgery is safe. However, from a feasibility standpoint, factors such as the time required for prehospital transport, medical stabilization and diagnostic investigation delay the delivery of definitive surgical care. One Canadian study and one European study have demonstrated that between 25% and 50% of patients underwent surgery before 24 hours postinjury. 31,32
There are a number of limitations to our study. First, this is a retrospective analysis. We feel that the retrospective design does not limit the strength of conclusions drawn from this study due to 2 reasons: First, due to the ethical constraints and impracticality of conducting a randomized, controlled trial on early versus late surgical intervention in human subjects and second, the strength of recommendations provided by a retrospective study and an observational prospective study are similar. Although retrospective in nature, to our knowledge, this is the largest study to date focusing on acute spinal cord injury in the thoracolumbar region. Our study is strengthened by the direct comparison of outcomes (in terms of neurological recovery) between early- and late-operated patients. Second, despite our large numbers, we approached but failed to reach statistical significance for 2 of our findings: for the proportion of patients who improved 2 ASIA grades between the early and late groups (P = .069) and the early- versus late-operated patients with ASIA A SCI (P = .179). We plan to continue to accrue more patients in these subgroups in the future until we have adequate power to determine if there is a true difference or not.
We have drawn 3 conclusions from our results. First, significantly greater number of patients show ≥1 grade neurological improvement if operated within first 72 hours of SCI. Second, ≥2 grade neurological recovery can be expected in greater proportion of patients operated within first 24 hours after SCI. Third, neurological recovery is not influenced by timing of surgery in patients with complete SCI (ASIA A).
Conclusion
We believe that the earlier the decompression, the better it is. However, practical constraints in the real world sometimes means that “early” is less than 72 hours. Our study shows that the 72-hour cutoff represents a promising and practical time window during which surgical decompression has the potential to confer a neuroprotective effect.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.