
Abstract
Study Design
Retrospective multicenter study.
Objectives
The effectiveness of early surgery for cervical spinal injury (CSI) has been demonstrated. However, whether early surgery improves outcomes in the elderly remains unclear. This study investigated whether early surgery for CSI in elderly affects complication rates and neurological outcomes.
Methods
This retrospective multicenter study included 462 patients. We included patients with traumatic acute cervical spinal cord injury aged ≥65 years who were treated surgically, whereas patients with American Spinal Injury Association (ASIA) Impairment Scale E, those with unknown operative procedures, and those waiting for surgery for >1 month were excluded. The minimum follow-up period was 6 months. Sixty-five patients (early group, 14.1%) underwent surgical treatment within 24 hours, whereas the remaining 397 patients (85.9%) underwent surgery on a standby basis (delayed group). The propensity score-matched cohorts of 63 cases were compared.
Results
Patients in the early group were significantly younger, had significantly more subaxial dislocations (and fractures), tetraplegia, significantly lower ASIA motor scores, and ambulatory abilities 6 months after injury. However, no significant differences in the rate of complications, ambulatory abilities, or ASIA Impairment Scale scores 6 months after injury were observed between the matched cohorts. At 6 months after injury, 61% of the patients in the early group (25% unsupported and 36% supported) and 53% of the patients in the delayed group (34% unsupported and 19% supported) were ambulatory.
Conclusions
Early surgery is possible for CSI in elderly patients as the matched cohort reveals no significant difference in complication rates and neurological or ambulatory recovery between the early and delayed surgery groups.
Introduction
The number of cervical spinal injury (CSI) cases among the elderly is increasing1-5 because of the aging of the population in many countries worldwide. 6 Because early rehabilitation is crucial for the management of CSI, 7 and patients with fractures and dislocations with instability require surgical treatment. Furthermore, surgery may be indicated even if there is no complicating fracture.8-11 However, because the functional reserve of major organ systems decreases with advancing age, these patients have more comorbidities, including frailty; consume more oral medications, such as anticoagulants; and have a higher risk of postoperative complications.12-14 Therefore, older age may influence surgeons’ decision making in surgical planning for elderly patients with CSI. 15
Among them, the timing of surgery is a concern in surgical treatment for CSI. “Time is spine” 16 or the effectiveness of early surgery for traumatic CSI has been demonstrated; however, those studies were based on data from relatively young patients.17-26 Our previous study, which was limited to spinal cord injuries without fractures, found no advantage of early surgery in elderly patients. 26 Elderly patients have various comorbidities and limited physical capacity; therefore, early surgery may increase perioperative complications. The background of elderly patients who are rushed to the hospital because of trauma is often unclear, which makes it difficult to determine whether early surgery can be performed safely. Thus, time may be needed to optimize the patient’s medical condition, wait for the effects of anticoagulants to dissipate, and assess and plan for the entire body before surgery. 27
Moreover, early surgery may not allow elderly patients to recover properly because information on the differences in spinal recovery potential after CSI between elderly and younger patients is limited. A difference may exist in spinal recovery capacity between elderly and young patients because elderly patients have poorer postoperative neurological recovery in degenerative cervical myelopathy, which is a type of chronic spinal cord injury. 28 Thus, elderly patients with CSI may not fully benefit from early surgery, similar to in degenerative cervical myelopathy.
Given these circumstances, the advantages and disadvantages of early surgical treatment should be considered in elderly patients with CSI. Our previous study 26 focused on spinal cord injuries without fractures; however, few studies have comprehensively examined the appropriateness of early surgery, including the presence or absence of fractures, which may change the usefulness of early surgery. Surgery for spinal cord injury with fractures is more invasive than that for spinal cord injury without fractures and may have a greater impact on the prognosis of the elderly; however, the difference between surgery with and without fractures is unclear.
This study investigated the effect of early surgery on perioperative complications and neurological outcomes in the elderly. We hypothesized that early surgery would increase perioperative complications in elderly patients with CSI, although it would be effective in improving neurological symptoms. The primary outcome was the degree of recovery from neurological deficits and ambulation. Furthermore, the secondary outcome was the complication rate. We compared each outcome in the overall and matched cohorts.
Methods
Patient Population
This multicenter study was based on a retrospective database of patients aged ≥65 years who were hospitalized for CSI between 2010 and 2020. This study was conducted by the Japan Association of Spine Surgeons with Ambition group. 29 The minimum follow-up period was 3 months. Thirty-three medical institutions participated in data collection. This study was approved by the Institutional Review Board (No. 3352-1) of each of the 25 representative institutions. Because this was a retrospective study, informed consent was not required for submission. The opt-out form for this study was posted on a website (https://web.sapmed.ac.jp/orsurg/guide/hj0g2h00000007ax-att/pgsps60000000g3l.pdf), and no inquiries were received. Consequently, 1512 patients were enrolled in the database.
The inclusion criteria for the study were patients aged ≥65 years with traumatic acute CSI and a neurological deficit who were followed up for at least 6 months after surgical treatment. We excluded patients with ASIA Impairment Scale (AIS) E, those with unknown operative procedures, and those waiting for surgery for >1 month. Of the database, 903 patients (59.7%) underwent surgery. In total, 266 patients with AIS E and three patients with unknown surgical procedures were excluded. Moreover, 90 patients whose treatment plan was changed from conservative therapy to surgery >1 month after admission were excluded. Additionally, 82 patients with <6 months of follow-up, other than those who died, were excluded. Thus, 462 patients were included in the analysis (Figure 1). Spine surgeons at each institution performed a comprehensive evaluation of the patients’ conditions and determined whether to prioritize the beginning of the surgery or stabilize their conditions. After that, they decided when the surgery should be performed. Early surgery was defined as surgery within 24 hours from injury. Delayed surgery was defined as any other surgery after 24 hours. Additionally, a sub-analysis within early surgery was performed; in the sub-analysis, ultra-early surgery was defined as surgery within 8 hours, and surgery after 8 hours but within 24 hours was defined as relatively early surgery. Both early and delayed surgeries were performed by orthopedic spine surgeons. Patient selection flowchart.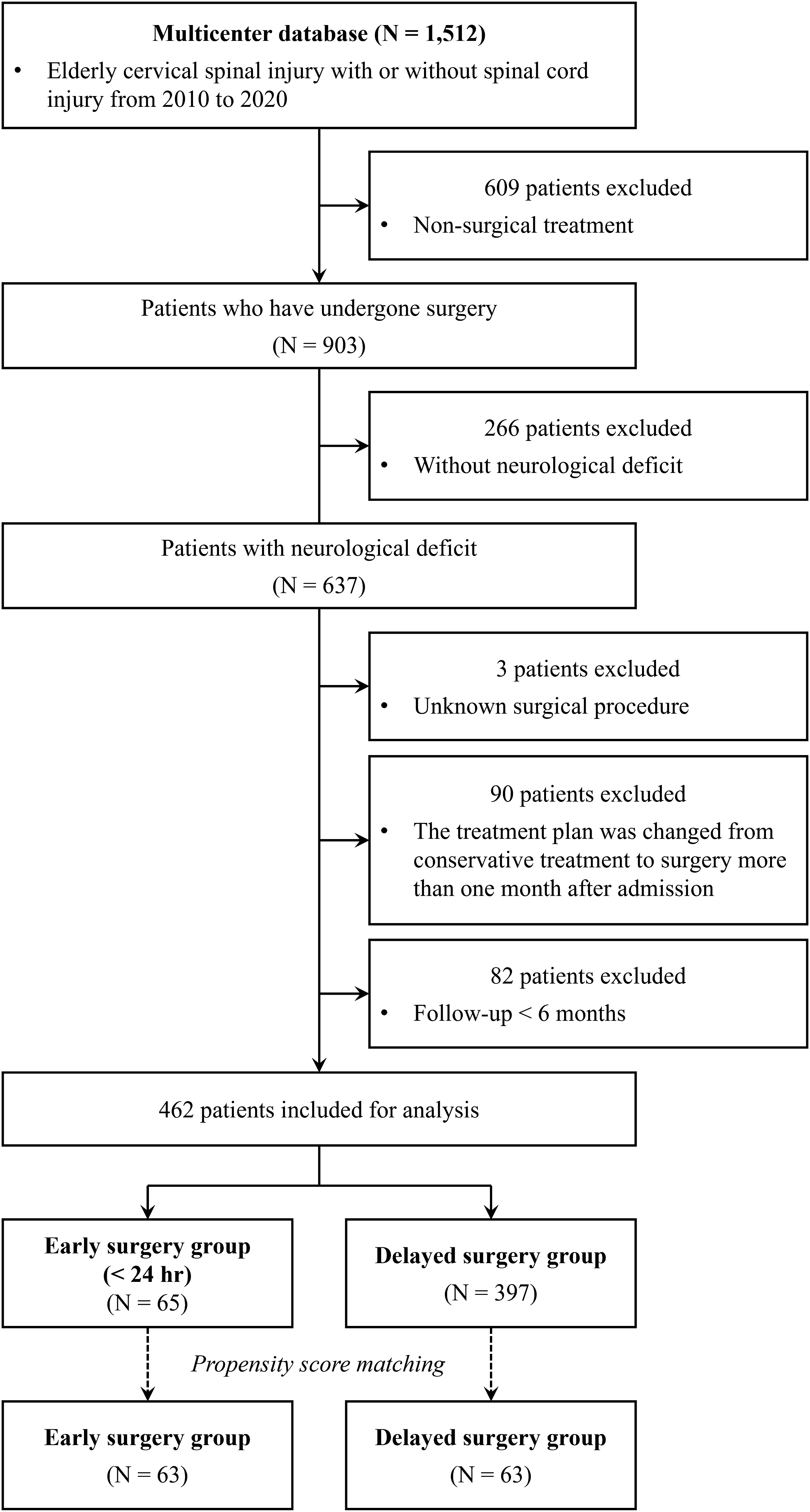
Patients’ Demographic and Operative Data
Age, sex, cause of injury, diagnosis with the presence of fracture/dislocation and injury levels, mode of CSI and ASIA motor score, AIS, presence of concomitant injuries (particularly head, chest, and vertebral artery injuries), presence of comorbidities, and regular medications were recorded. Furthermore, the surgical procedure, operative time, blood loss, presence of blood transfusions, intraoperative complications, and inpatient complications were recorded; moreover, ambulatory abilities and AIS at discharge and ambulatory abilities and AIS 6 months after injury were evaluated.
Rehabilitative care was provided to the postoperative patients whenever possible. If the patients’ wounds and general conditions were stable, they were discharged. However, if going home was difficult, patients were transferred to other hospitals for rehabilitation and nursing care.
Statistical Analysis
Data are presented as means ± standard deviations for continuous variables and as numbers and percentages for categorical variables. All statistical analyses were performed using R (version 4.2.1; https://www.R-project.org) using the Wilcoxon rank-sum test, Fisher’s exact test, and Pearson’s chi-square test. P-values < .05 were used to denote statistical significance. Propensity score matching was performed using the MatchIt package (https://cran.r-project.org/web/packages/MatchIt). The following items were selected to adjust for patient background: age, sex, fracture, dislocation, ASIA motor score, tetraplegia, major comorbidities, diabetes mellitus, and anticoagulant and/or antiplatelet medications. Major comorbidities were defined as cardiac, respiratory, and chronic kidney diseases. Additionally, comparisons were made using the inverse probability weighting method, and the average treatment effect was estimated.
Results
Patients Demographics for Overall Analysis.
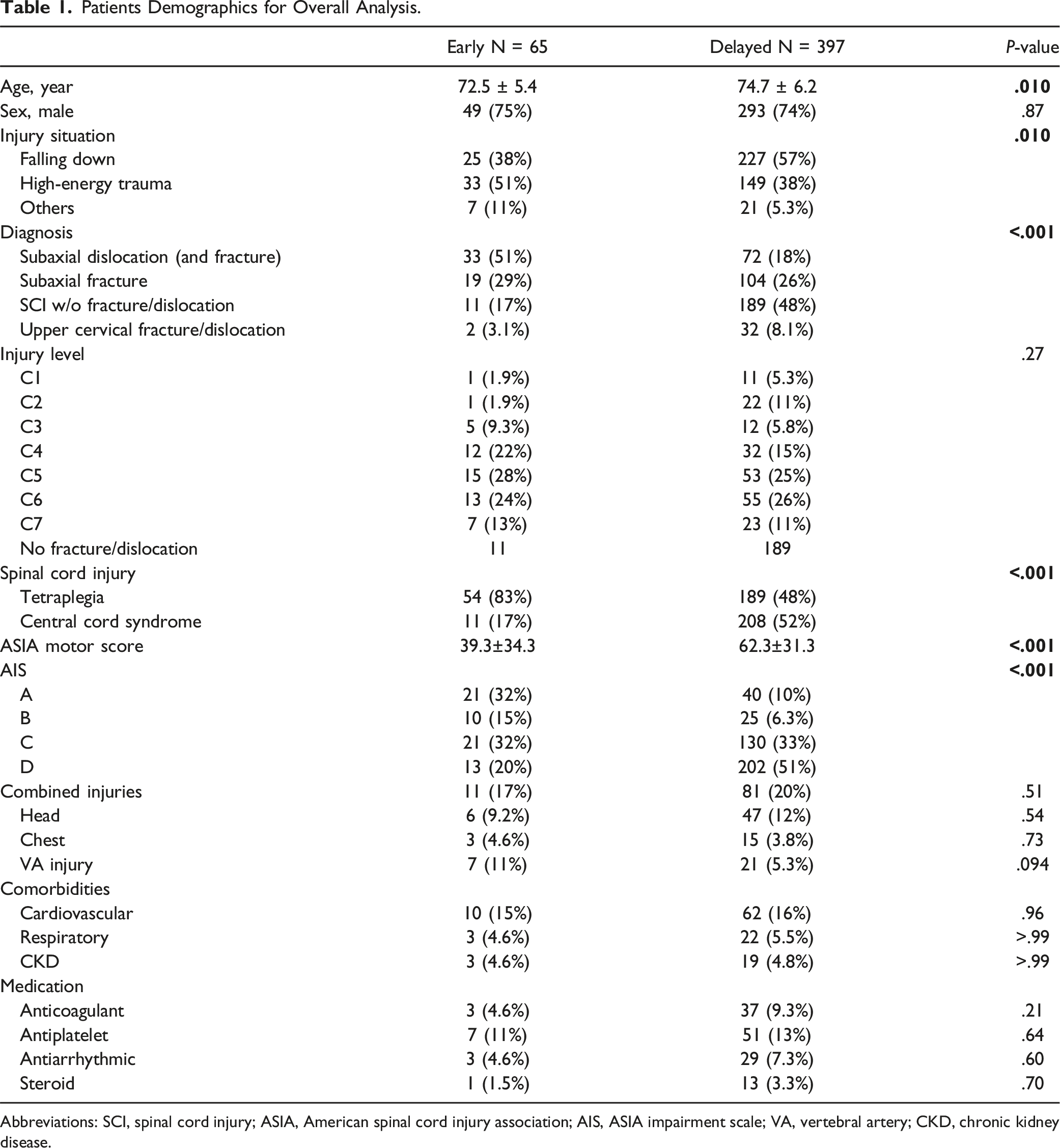
Abbreviations: SCI, spinal cord injury; ASIA, American spinal cord injury association; AIS, ASIA impairment scale; VA, vertebral artery; CKD, chronic kidney disease.
Treatment Progress for Overall Analysis.
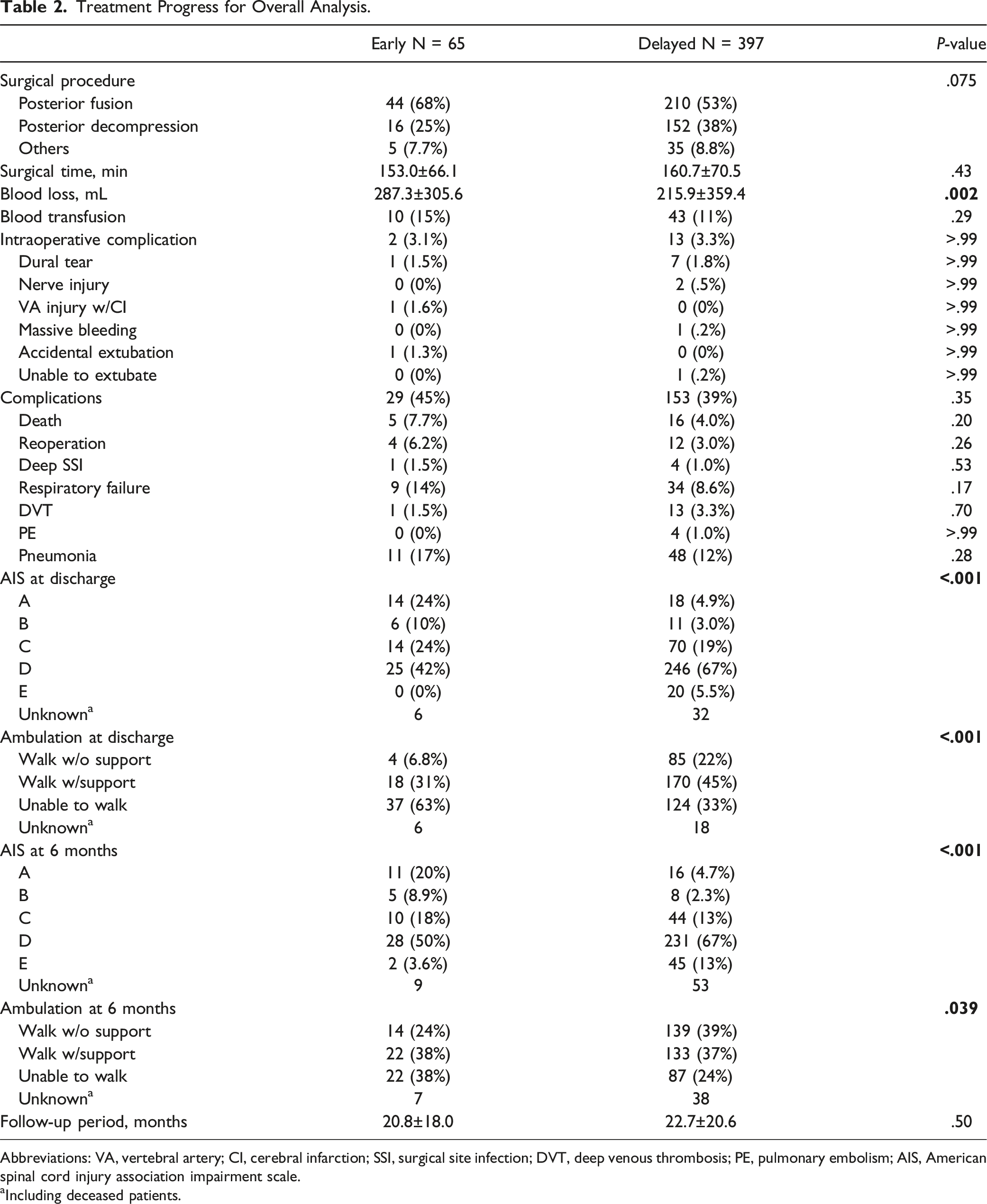
Abbreviations: VA, vertebral artery; CI, cerebral infarction; SSI, surgical site infection; DVT, deep venous thrombosis; PE, pulmonary embolism; AIS, American spinal cord injury association impairment scale.
aIncluding deceased patients.
Significant differences in patient ambulatory abilities and AIS were found at both discharge and 6 months after surgery, with the early group being inferior (Table 2). At discharge, 39% of the patients in the early group (6.8% unsupported and 31% supported) and 67% in the delayed group (22% unsupported and 45% supported) were ambulatory; 6 months later, 62% of the patients in the early group (24% unsupported and 38% supported) and 76% of the patients in the delayed group (39% unsupported and 37% supported) were ambulatory.
In the early surgery group, 29 patients underwent ultra-early surgery (mean time to surgery was 6.4 ± 1.5 h), whereas the remaining 36 patients underwent relatively early surgery (mean time to surgery was 15.3 ± 5.0 h). Although no significant differences in patient demographic characteristics were observed between the ultra-early and relatively early groups, the proportion of patients with AIS A was higher in the ultra-early group (38% vs. 28%). No significant differences in the incidence of complications during hospitalization, including mortality and respiratory failure, and AIS or ambulation (at discharge or 6 months later), were observed between the 2 groups (Supplementary Tables A and B).
Comparison of Propensity Score-Matched Cohort Between Early (<24h) and Delayed (24h) Surgery Cases
Patients Demographics for Matched Cohort Analysis.
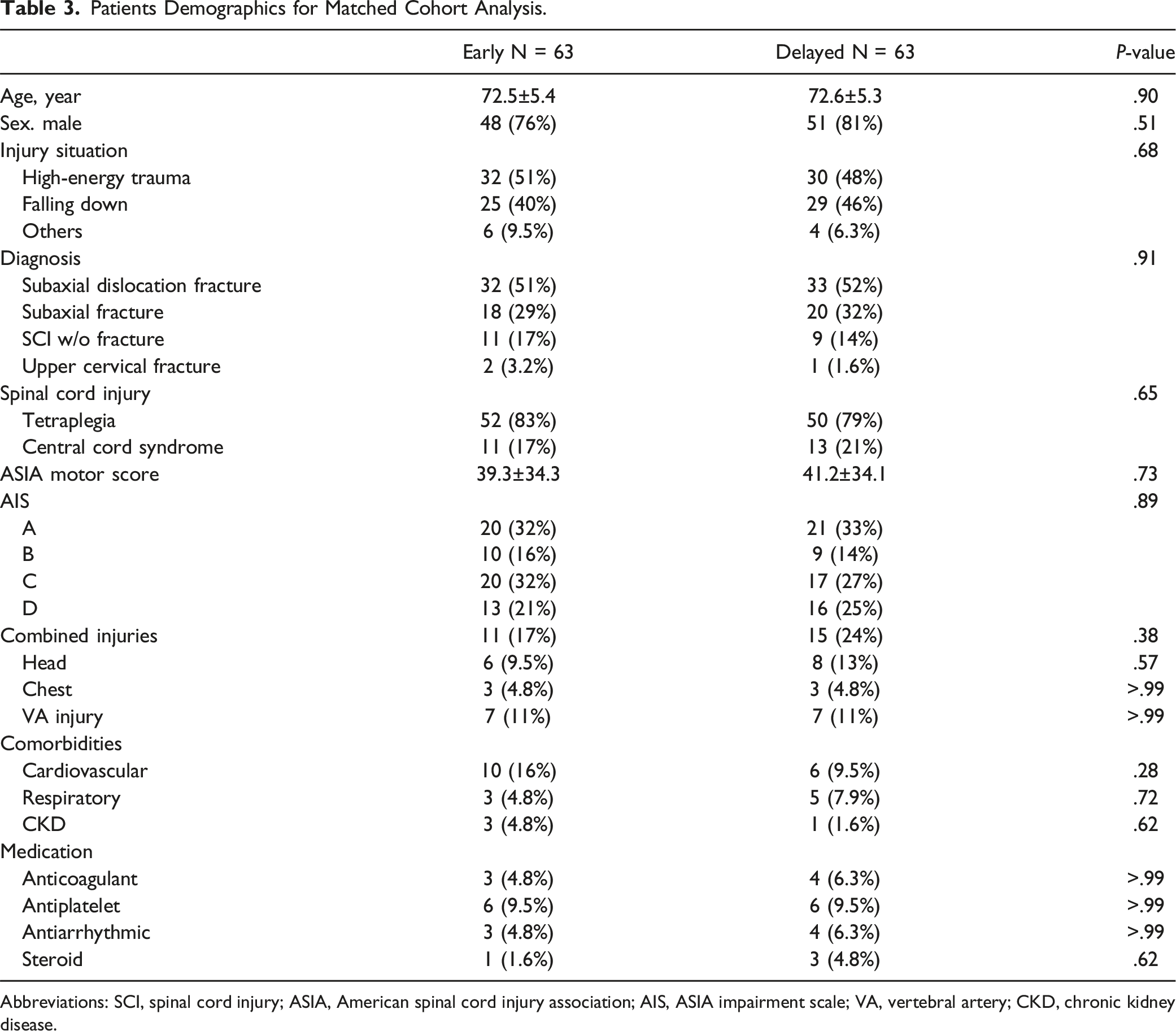
Abbreviations: SCI, spinal cord injury; ASIA, American spinal cord injury association; AIS, ASIA impairment scale; VA, vertebral artery; CKD, chronic kidney disease.
Treatment Progress for Matched Cohort Analysis.
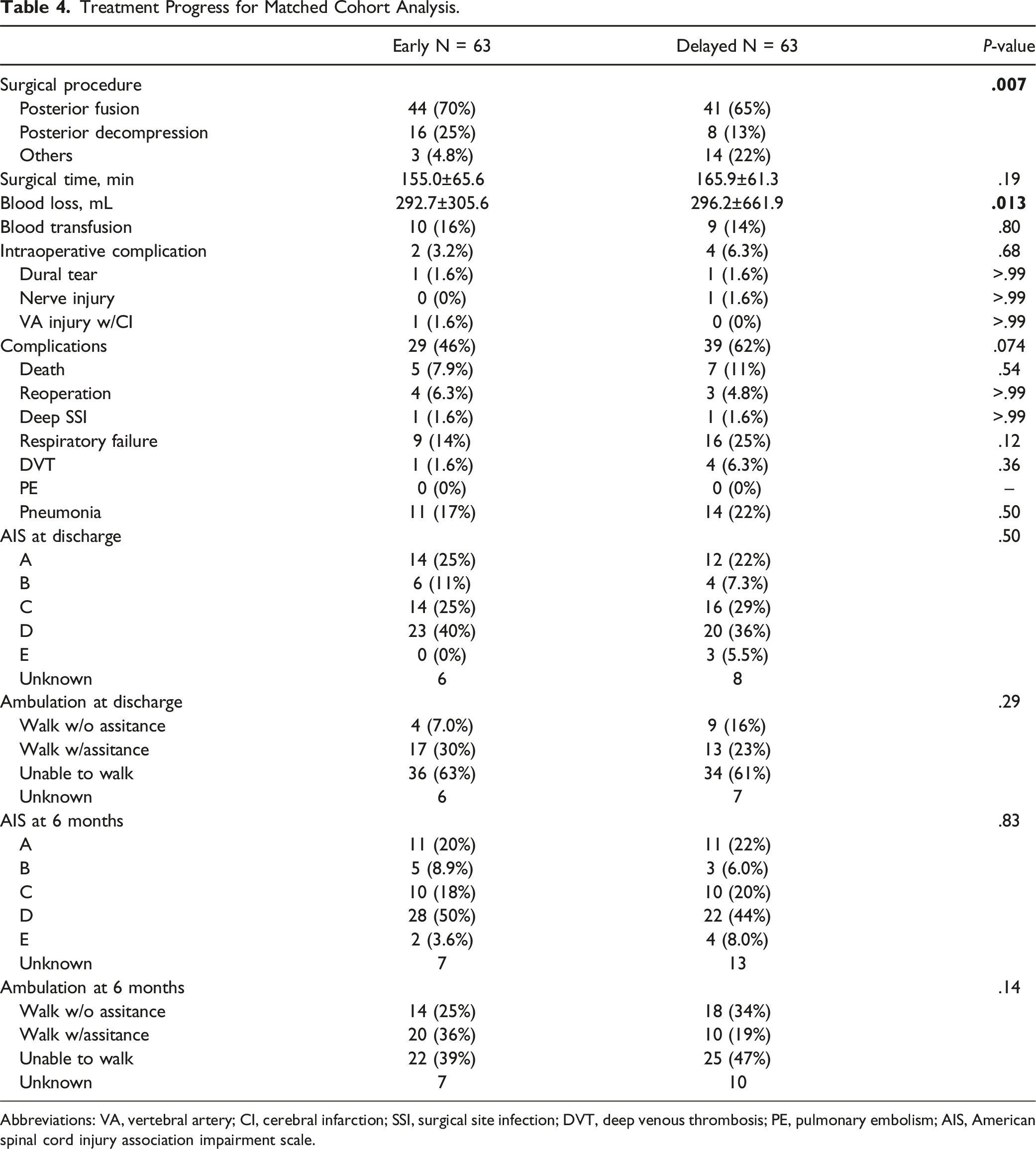
Abbreviations: VA, vertebral artery; CI, cerebral infarction; SSI, surgical site infection; DVT, deep venous thrombosis; PE, pulmonary embolism; AIS, American spinal cord injury association impairment scale.
AIS Grade Conversion in Matched Cohort Early Group.
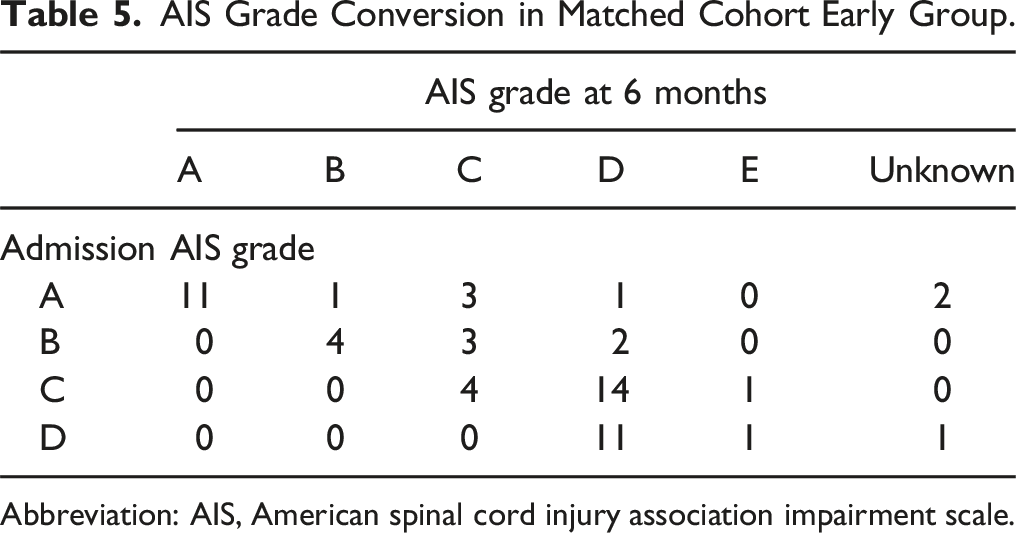
Abbreviation: AIS, American spinal cord injury association impairment scale.
AIS Grade Conversion in Matched Cohort Delayed Group.
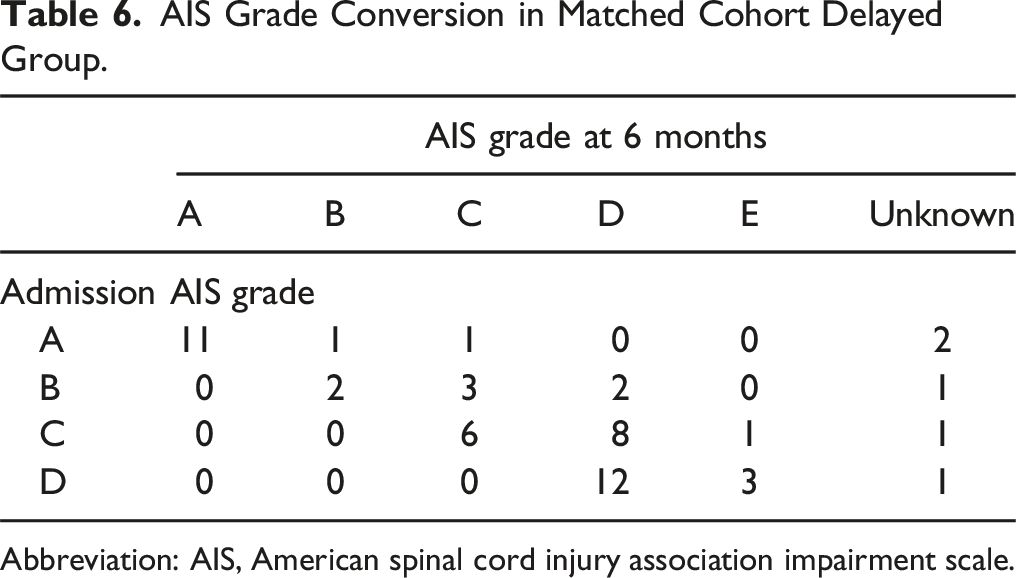
Abbreviation: AIS, American spinal cord injury association impairment scale.
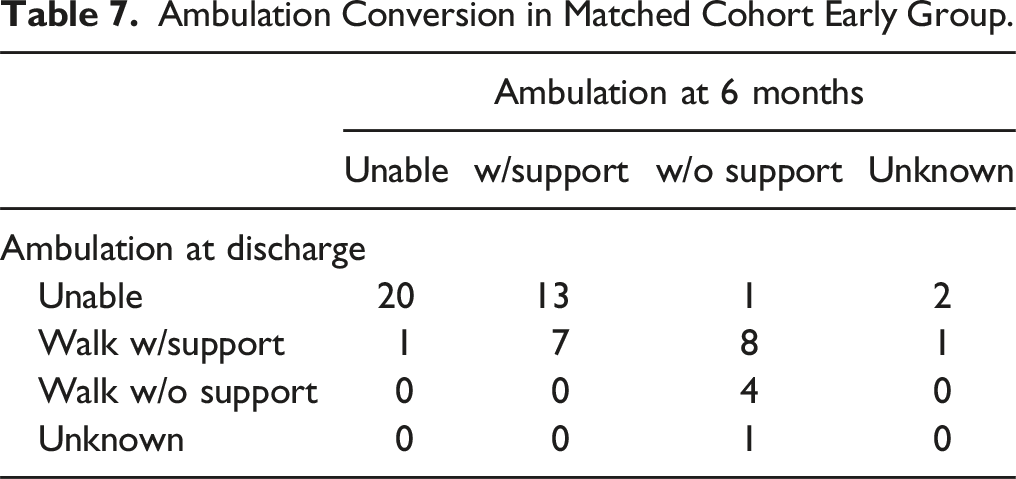
Ambulation Conversion in Matched Cohort Early Group.
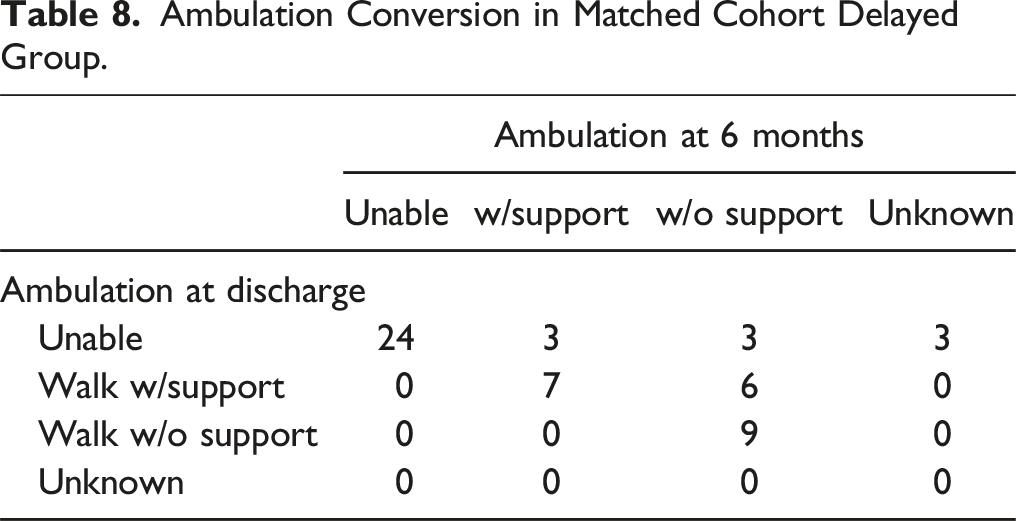
Ambulation Conversion in Matched Cohort Delayed Group.
Discussion
This large-scale retrospective study of the surgical treatment of elderly patients with CSI examined complications and treatment effects based on whether early surgery should be performed. A previous study 26 revealed that surgical treatment within 48 h for elderly patients with CSI without fractures did not affect neurological outcomes; however, we further expanded the scope of the subject to include patients with fractures to investigate the impact of early surgery. Approximately 15% of the patients underwent early surgery, including many patients with cervical dislocation and severe tetraplegia. The differences in complication rates and neurological outcomes between the early and delayed groups were not statistically significant when adjusted for propensity score matching.
One of the key points of this study is the constant complication rate when the baselines were aligned in both the early and delayed groups. Patients in the early group were expected to have an increased risk of potential complications because of insufficient time for preoperative systemic evaluation or insufficient time to medically optimize their conditions. 27 However, this expectation was not met. The early group included significantly more patients with high rates of postoperative complications, such as cervical dislocations and cases of severe tetraplegia, making the early and delayed groups quite different. We performed a baseline-aligned comparison using propensity score matching to address this issue. The proportion of patients on anticoagulants was also matched. Early surgery did not increase complications even when management was not necessarily optimized for surgery. Therefore, early surgery is acceptable in elderly patients with CSI.
Elderly patients have more comorbidities, such as cardiovascular, respiratory, and cerebrovascular diseases and dementia, which are assumed to increase the risk of perioperative adverse events.27,30 According to Ahn et al, elderly patients with spinal cord injury had a significant delay from admission to surgery compared with younger patients. 27 The complex management of comorbidities, in addition to the ambiguous optimal treatment for CSI in the elderly, may cause surgeons to hesitate in making treatment decisions and delay surgery to medically optimize the patients’ conditions. 27 Surgical delays can prolong immobilization, increase the risk of medical complications, and increase mortality in older patients. 27 However, careful clinical judgment is required because patients with medical complications may be unable to undergo early surgery safely. 23 Therefore, each patient should be evaluated individually because their pre-injury condition affects surgical tolerability. 31 Clinical judgment is required for high-risk patients, both in early surgery and in a cautious approach to risk management.
Overall, surgical treatment of elderly patients with CSI had a high complication rate; for example, approximately half of the patients in both groups experienced some complications in the matched cohort. However, no increase in fatal complications was observed owing to early surgery. Because the elderly are frail,12-14 mortality is high in these patients with traumatic spinal cord injury. 32 Furthermore, patients with CSI have high mortality rates. A retrospective study of patients with surgical spinal trauma using data from 2015 to 2018 (not limited to the elderly) by McGee et al revealed that CSI had the highest 30-day mortality rate at 7.3%. 33 Thus, it can be undoubtedly said that the risk of death in elderly patients with CSI was even higher. Furthermore, the overall incidence of respiratory failure and pneumonia was high. Respiratory care may be important in elderly patients with CSI with or without early surgery.
Another key point of this study concerns neurological outcomes. Several clinical studies17-24,26 suggest that early surgical decompression promotes neurological improvement in patients with CSI. Some studies has reported that early decompression is effective, particularly in patients with incomplete neurological damage.17,25,34 However, these studies are biased because they are based on data from relatively young patients. Few studies on early surgery are limited to elderly CSI cases. Inoue et al 31 revealed that early surgery (within 24 h) was associated with good neurological improvement in elderly patients (>65 years old) with CSI without associated fractures. However, a previous report 26 on elderly patients with CSI without fractures, using the same dataset as this study, did not find an advantage of surgical treatment within 48 h. Furthermore, ambulatory abilities and neurological assessment in terms of AIS at discharge and 6 months after injury did not differ significantly between the groups in the matched cohorts in this study. Thus, there was no advantage of performing early surgery in the elderly.
However, the effectiveness of early surgery cannot be ruled out based on these results, and it is hasty to conclude that early surgery for CSI is less effective in the elderly. Patients develop more comorbidities and become frailer as they age12-14; thus, neurological and ambulatory recoveries may not correspond linearly. Rehabilitation after CSI is effective even in the elderly. 35 Although patients with fractures or dislocations are forced to rest because of spinal instability, and early surgery for a fracture or dislocation enables prompt and aggressive rehabilitation. Our study did not provide accurate data on the vulnerability of each patient or detailed data on rehabilitation. Because of these limitations, individual patient characteristics persisted, even after matching. Alternatively, elderly patients may require more personalized medical care. Therefore, it is not accurate to deduce that the effect of early surgery in elderly patients with CSI is minimal.
This study has several limitations. First, selection bias may have existed because of the retrospective nature of this study. Second, the indications for early surgery depended on the judgment of the surgeon at each facility. Third, only short-term follow-up results were available because of patient dropout. Furthermore, the number of cases was insufficient to perform subanalyzes, such as limiting the analysis to patients without fractures or those taking anticoagulants. Additionally, performing a sub-analysis by matching “ultra-early,” “relatively early,” and “delayed” cases was impossible because of the small number of early cases, and comparison among patients with tetraplegia and patients with central cord syndrome was also not possible due to the small number of patients with central cord syndrome who underwent early surgery. However, this study included data from a wide area and allowed evaluation of outcomes in elderly patients with CSI.
Conclusion
We conducted a retrospective study of complications and treatment outcomes to determine the benefits of early surgery for elderly patients with CSI. Analysis of the matched cohort showed no significant difference in complication rates and neurological or ambulatory recovery between the early and delayed surgery groups. Although early surgery for elderly patients with CSI may not improve treatment outcomes, it did not increase complication occurrence. Therefore, early surgical treatment is possible for elderly patients with CSI.
Supplemental Material
Supplemental Material - Early Versus Delayed Surgery for Elderly Traumatic Cervical Spinal Injury: A Nationwide Multicenter Study in Japan
Supplemental Material for Early Versus Delayed Surgery for Elderly Traumatic Cervical Spinal Injury: A Nationwide Multicenter Study in Japan by Naoki Segi, Hiroaki Nakashima, Sadayuki Ito, Noriaki Yokogawa, Takeshi Sasagawa, Kota Watanabe, Satoshi Nori, Toru Funayama, Fumihiko Eto, Hideaki Nakajima, Yoshinori Terashima, Ryosuke Hirota, Ko Hashimoto, Yoshito Onoda, Takeo Furuya, Atsushi Yunde, Shota Ikegami, Masashi Uehara, Hidenori Suzuki, Yasuaki Imajo, Hiroshi Uei, Hirokatsu Sawada, Kenichi Kawaguchi, Kazuo Nakanishi, Nobuyuki Suzuki, Yasushi Oshima, Tomohiko Hasegawa, Yoichi Iizuka, Hitoshi Tonomura, Hidetomi Terai, Koji Akeda, Shoji Seki, Masayuki Ishihara, Gen Inoue, Haruki Funao, Toshitaka Yoshii, Takashi Kaito, Katsuhito Kiyasu, Hiroyuki Tominaga, Kenichiro Kakutani, Daisuke Sakai, Tetsuro Ohba, Bungo Otsuki, Masashi Miyazaki, Kenta Murotani, Seiji Okada, Shiro Imagama, and Satoshi Kato in Global Spine Journal
Footnotes
Acknowledgments
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
ORCID iDs
Supplemental Material
Supplemental material for this article is available online
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.