
Abstract
Purpose:
The purpose of this study is to explore if the surgical treatment will accelerate the progression of spinal cord injury (SCI) in patients with cervical Ossification of the posterior longitudinal ligament (OPLL) and if surgery will have better curative effect than conservative treatment.
Methods:
An extensive search of literature was implemented in PubMed, EMBASE, and other online databases. The quality of the included articles was evaluated according to the Newcastle-Ottawa Quality Assessment Scale, as recommended by the Cochrane manual, and meta-analysis was performed using the review manage5.3 software.
Results:
No obvious statistical difference was observed in the rate of SCI progression (P > 0.05, OR 1.15 [0.66, 2.00]), cervical range of motion, (P > 0.05, weighted mean difference (WMD) 4.52 [−5.75, 14.79]), and Japanese Orthopedic Association scores before surgery (P > 0.05, WMD −2.78 [−7.87, 2.32]) between the surgical group and conservative treatment group. However the surgical group illustrated obviously higher neurofunctional recovery rate (P < 0.05, OR 6.07 [1.55, 23.78]) and postoperative JOA score of the surgery group (P < 0.05, WMD −0.77 [−1.21, −0.33]) than conservative group.
Conclusions:
Based on this meta-analysis, there is not enough evidence to indicate that surgery will accelerate the progress of SCI with OPLL. However, the superiority of surgical efficacy can be observed over conservative treatment in terms of relieving neurological symptoms.
Keywords
Introduction
Ossification of the posterior longitudinal ligament (OPLL) of the cervical spine is characterized by ectopic bone formation in spinal ligaments, 1 the progressive ossification of the ligament will cause compression of the spinal cord, leading to neurological decline. 2 OPLL is a common disease in Asian countries. The incidence of OPLL in Japan is from 1.9% to 4.3%, and that in other Asian countries is about 3.0%. Notably, about 30% of patients with spinal cord injury (SCI) have OPLL in cervical spine. 3
For patients with cervical spine OPLL with severe spinal cord compression, the effect of surgery is significantly better than conservative treatment. However, patients with mild and slowly progressing OPLL of the cervical spine can be free of symptoms and signs of severe spinal cord compression for a long time. Generally, the pathogenesis of OPLL is mechanical compression, 4 and surgery is the inevitable choice. In fact, it is controversial whether implemented operation for cervical OPLL patients with incomplete SCI. Some experts recommended conservative treatment because the incomplete SCI might heal within months or even years. 5 –9 For example, Pham et al. demonstrated, among non-surgical OPLL patients, patients without myelopathy might remain progression-free, while patients with myelopathy have high rates of SCI progression. 7 Meanwhile, secondary neurological impairment caused by calcified ligaments pressing the spinal cord is irreversible, and some other articles reported that surgery would accelerate the progress of SCI in OPLL patients. 10 –13 For example, Chen et al. showed that patients with OPLL who underwent conservative treatment have the highest incidence of SCI, at 4.1 cases per 1,000 person-years, and the incidence of SCI was lower in such patients who received surgical treatment, at 3.7 cases per 1,000 person-years. 13 Thus, it still remains controversial whether surgical treatment for patients with OPLL would be better than conventional treatment.
Accordingly, we compared the outcomes for patients with OPLL underwent surgery and conventional treatment, including cervical range of motion (ROM), Japanese Orthopedic Association (JOA) score, neurofunctional recovery rate, and SCI progression rate. This systematic review and meta-analysis was conducted to evaluate whether surgery will have better results than conservative treatment, and if surgical treatment was performed, will it accelerate the progression of spinal cord injury (SCI) in patients with cervical OPLL?
Methods
This article was performed following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 14
Search strategy
An extensive search of literature was performed in PubMed, EMBASE, EBSCO host, the Cochrane Library, China National Knowledge Infrastructure (CNKI), Wanfang, VIP databases from the database up to March 2020. We also manually searched the reference lists of articles and reviews for possible related studies. Comprehensive search for potentially relevant research.
The search strategy was as follows:
(1) Ossification of Posterior Longitudinal Ligament OR Posterior Longitudinal Ligament Ossification OR Posterior Longitudinal Ligament Calcification OR Calcification of Posterior Longitudinal Ligament OR OPLL; (2) “Surgical Procedures, Operative” OR Operative Surgical Procedure OR “Surgical Procedure, Operative” OR “Procedure, Operative Surgical” OR “Procedures, Operative Surgical” OR Operative Procedures OR Operative Procedure OR “Procedure, Operative” OR “Procedures, Operative” OR Operative Surgical Procedures OR “Surgery, Ghost” OR Ghost Surgery; (3) Conservative Treatment OR Conservative Treatments OR “Treatment, Conservative” OR “Treatments, Conservative” OR Conservative Management OR Conservative Managements OR “Management, Conservative” OR Conservative Management OR Conservative Therapy OR Conservative Therapies OR “Therapies, Conservative” OR “Therapy, Conservative”; (4) Cohort Study OR Cohort Studies OR Control Groups OR Clinical Study OR Randomized Controlled Trial OR Controlled Clinical Trial OR Randomized Controlled Trials OR “Clinical Trials, Randomized” OR Non-Randomized Controlled Trials OR Quasi-Experimental Study OR “Clinical Trials, Non-randomized” OR Non-randomized Clinical Trials OR Prospective Studies OR Retrospective Studies OR Concurrent Studies OR Closed Cohort Study OR Cohort Analysis; (1), (2), (3) AND (4).
Eligibility criteria and exclusion criteria
Studies would be included in the meta-analysis if they met the following criteria:
(1) Radiographic examination confirmed OPLL on the cervical spine; (2) Subjects had no progressive exacerbation of clinical symptoms, and manifested as symptoms and signs of incomplete spinal cord compression; (3) Subjects in the intervention group underwent surgical treatment, including anterior cervical decompression with fusion and posterior cervical decompression with fusion; (4) Subjects in the control group underwent non-surgical treatment, including rest in bed, nutritional nerves, orthotics and traction; (5) Outcomes had been reported in the article including SCI progress rate, neural function recovery rate, Japanese Orthopedic Association(JOA) score, and cervical spine range of motion(ROM), etc.; (6) The study was designed as randomized controlled trials or non-randomized controlled trials.
Studies were excluded if they were:
(1) case report; (2) reviews or meta-analysis; (3) correspondence; (4) repeated publication of the same data; (5) case review and observation of non-control studies; (6) animal studies; (7) OPLL of the thoracic spine.
Data extraction
Study characteristics and outcomes in the included studies were extracted as follows: (1) author and year; (2) type of study design; (3) sample size of the surgical and conservative groups; (4) gender ratio and age of patients; (5) follow-up. Data were extracted independently by two reviewers. Any disputes would be resolved through consultation with a third researcher.
Quality assessment
Two reviewers assessed the quality of the studies according to the Newcastle-Ottawa Quality Assessment Scale (NOS), as recommended by the Cochrane Non-Randomized Studies. This scale included three items: selection of study groups (four points); comparability of groups (two points); ascertainment of exposure and outcomes (two points) for case control and cohort studies, respectively.
The study scored six or more was eligible for data-pooling and the study scored seven or more was considered high quality. 15 Any disagreement would be solved by discussion or consulted with a senior reviewer.
Data analysis
We implemented all statistical analyses using the Review Manager (RevMan version 5.3; the Cochrane Collaboration). Not directly supplied data of the standard deviation were estimated using the range and sample size. 16 Heterogeneity among the included studies was quantified via calculating I2 statistic. P < 0.05 or I2 ≥ 50% were considered statistical significance. Standard mean difference (SMD) or weighted mean difference (WMD) were calculated for the continuous variables in accordance with the consistency of measurement units, whereas the odds ratio (OR) was used for calculating the dichotomous variables. Continuous variables were presented in the form of WMD and 95% confidence intervals (95% CI), while dichotomous variables were presented as OR and 95% CI. When P < 0.05 and I2 ≥ 50%, the random effects model was used. When P ≥ 0.05 or I2 < 50%, the fixed effects model would be used. Publication bias was formally assessed by funnel plot. Sensitivity analysis was performed to find sources of heterogeneity by eliminating one or more study.
Result
Search results
In the initial search, 198 potentially relevant articles were identified. After removing 41 duplications, the titles and abstracts of 157 articles were screened according to the inclusion and exclusion criteria, and the full text of 11 studies was finally reviewed. Two reviewers completed the screening of literature independently. In case of differences, they were discussed and resolved with the third author. Finally, eight studies were identified and included in this meta-analysis. 6,13 –15,17 –20 The process is shown in Figure 1.

The flow chart shows the process for identifying relative studies.
General characteristics and quality assessment
All eight articles that included in our meta-analysis were non-randomized controlled studies: six were retrospective studies and two were prospective studies. Years of literature publication range from 2004 to 2018. The baseline characteristics of these included studies were presented in Table 1. A total of 1553 patients were reported, and the mean age ranged from 53.1 to 66.2. The quality of included studies was all relatively high according to the NOS scale (Table 2). Among these articles, three are graded eight points, and five are graded seven points.
The general characteristic of the included studies.
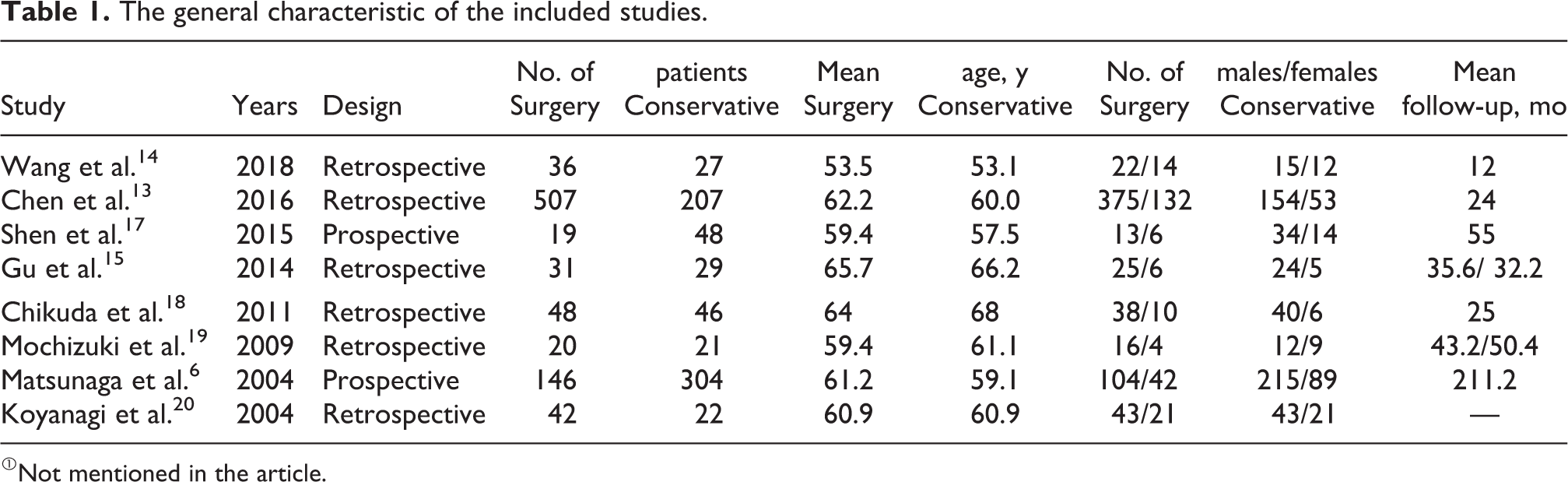
①Not mentioned in the article.
Quality evaluation according to the Newcastle-Ottawa Quality Assessment Scale.

SCI progression rate
Six articles (n = 1002 patients; 654 in the surgical group and 348 in the conservative group) containing the rate of SCI progression were analyzed. No significant heterogeneity was calculated between the studies, and the fixed effects model was used to pool data (I2 = 27%, P = 0.23). There was no significant difference in the SCI progression rate between the two groups (P > 0.05, OR 1.15 [0.66, 2.00], Figure 2). Tests for funnel plot asymmetry are generally only performed when at least 10 studies are included in the meta-analysis. As our analysis included less than 10 studies for each variable, publication bias was not assessable.

Odds ratio of SCI progress rates between the surgery group and the conservation group. CI confidence interval, M-H Mantel-Haenszel.
Neurofunctional recovery rate
Three literature (n = 287 patients; 207 in the surgical group and 80 in the conservative group) reported the rate of neurological recovery. The recovery rate of nerve function in the surgery group was higher than the conservative group (P < 0.05, OR 6.85 [3.78, 12.42], Figure 3). Significant heterogeneity existed in these three studies (I2 = 78%, P = 0.01). According to the results of the sensitivity analysis, after removing one study, the heterogeneity was reduced between the studies. The remaining literature data was statistically analyzed using the fixed-effect model. The results showed that the neurological recovery rate in the surgical group was higher than the conservative treatment group (P < 0.05, OR 3.02 [1.33, 6.87], Heterogeneity: P = 0.37, I2 = 0%, Figure 4).

Odds ratio of the neurofunctional recovery rate between the surgery group and the conservative group. CI confidence interval, M–H Mantel–Haenszel.

Odds ratio of the neurofunctional recovery rate between the surgery group and the conservative group after removing one study.
Preoperative and postoperative JOA score
Two articles (n = 108 patients; 39 in the surgery group and 69 in the conservative group) reported preoperative and postoperative JOA score. No statistically significant difference exists in the preoperative JOA score between the two groups (P > 0.05, WMD −2.78 [−7.87, 2.32], Figure 5). Notably, significant heterogeneity occurred between the two articles (P < 0.001, I2 = 99%). In contrary, the postoperative JOA score was visibly higher in the surgery group compared with conservative group without significant heterogeneity (P < 0.001, WMD −0.77 [−1.21, −0.33], Heterogeneity: P = 0.18, I2 = 43%, Figure 6).

Weighted mean difference of preoperative JOA score between the surgery group and the conservation group. SD standard deviation, CI confidence interval, IV inverse variance.

Weighted mean difference in postoperative JOA score between the surgery group and the conservative group. SD standard deviation, CI confidence interval, IV inverse variance.
ROM
Two literature (n = 101 patients; 51 in the surgery group and 50 in the conservative group) reported ROM. Significant heterogeneity was calculated (P = 0.02, I2 = 82%), and the random effects model was used to pool data. No significant difference on ROM between the surgery group and the conservative treatment group was found (P > 0.05, WMD 4.52 [−5.75, 14.79], Figure 7).

Forest plots of postoperative cervical ROM in the surgery group and the conservative group.
Discussion
This study found that the neurological recovery rate and the postoperative JOA score of the surgical group was higher than the conservative treatment group. No significant difference was found on JOA score before surgery, ROM of cervical, and SCI progression rate between the surgical group and the conservative treatment group. Then, we concluded there was not enough evidence to indicate that surgery will accelerate the progress of SCI with OPLL. However, the superiority of surgical efficacy can be observed over conservative treatment in terms of relieving neurological symptoms.
Since OPLL is known to be a typical progressive disease, and there is little evidence that non-surgical treatment will stop or reverse its progression. Risk factors which can promote the development of SCI in OPLL patients should be taken into account. According to the study by Matsunaga et al., 21 22% of 167 cervical OPLL patients receiving conservative treatment exacerbated myelopathy, with an average follow-up of 11 years and 2 months. Their analysis showed that a residual sagittal diameter of the spinal canal less than 6 mm was the decisive factor for the development of myelopathy. A research conducted by Data from the study by Koyanagi and his collegues 20 showed that the remaining sagittal diameter of the spinal canal less than 8 mm is more likely to trigger lower limb motor dysfunction based on the spinal canal diameter of 64 patients with OPLL cervical spine. The invasiveness of surgery and postoperative complications should also be considered. A multi-center study by Chiba et al. showed that approximately 60% of patients who underwent laminoplasty had OPLL progression (thickness or length of 2 mm). The incidence of ossification progression after 2 years was 56.5%. 8 Lee and his colleagues concluded that laminoplasty was inclined to the progress of OPLL as compared with fusion surgery. 9 Other complications include C5 nerve root paralysis, postoperative cervical axial pain, cerebrospinal fluid leakage and injury of spinal cord, cervical arteriovenous, laryngeal reflex nerve. 22,23
Understanding the natural course of myelopathy in patients with cervical OPLL can provide evidence to the choice of treatment methods. Wu et al. reported a cohort study that used a national database to assess the incidence of SCI of 265 cervical spondylosis patients with OPLL who underwent conservative treatment. 24 The conclusions had been drawn after the subjects received 34,723.5 person-years of follow-up that compared with controls (composed of age- and sex-matched people), patients in the OPLL group were more likely to develop cervical SCI and related disabilities. Many OPLL patients do not experience neurological symptoms in their daily lives, and some patients are unaware of OPLL. When suffering a small applied force, even a minor trauma can promote the occurrence of cervical SCI. Koyanagi reported a study in which 61% of patients with OPLL were triggered and hospitalized because of a flat fall. 25 Therefore, early identification and proper management are the key to guaranteeing the quality of life of OPLL patients. 26
Limitations
As with other studies, several limitations in the present study have forced us to interpret the results carefully. First, due to the inconsistency in the evaluation criteria of severity of cord injury in the included studies, the subgroup analysis cannot be conducted. However, each of the article explain the severity of cord injury that patients were evaluated at admission. All patients had sensory and motor function retention, which was classified as incomplete spinal cord injury. In addition, because of the insufficiency of included studies, no sensitivity analysis can be performed to find sources of heterogeneity. Although there are limitations, the results of this study still have useful guideline.
Conclusions
According to this meta-analysis, there is no enough evidence to prove that surgical treatment will accelerate the progress of SCI. To better understand the progress of SCI in patients with cervical OPLL, it’s worth more research and long-term follow-up clinical studies. However, we could discern that surgery performed much better than conservative treatment at relieving neurological symptoms. Therefore, patients with OPLL with myelopathy were advised to undergo an operation to relieve neurological symptoms, even if surgery gives rise to trauma, more complications and even a second operation. While conservative treatment should be selected with caution, protecting patients from illness for a long time. Considering the limitations of our meta-analysis, a well-designed, prospective, randomized controlled study with large samples ought to be needed to acquire a more convincing conclusion.
Supplemental material
Supplemental Material, sj-doc-1-osj-10.1177_2309499020981782 - Does surgical treatment increase the progression of spinal cord injury in patients with ossification of posterior longitudinal ligament of cervical spine? A systematic review and meta-analysis
Supplemental Material, sj-doc-1-osj-10.1177_2309499020981782 for Does surgical treatment increase the progression of spinal cord injury in patients with ossification of posterior longitudinal ligament of cervical spine? A systematic review and meta-analysis by Bi Zhang, Yufei Zhang, Bin Ma, Junchi Ma, Xiaoyong Chen, Junjie Li and Haifeng Yuan in Journal of Orthopaedic Surgery
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by The National Natural Science Foundation of China (no. 81760231; no. 81160220), The Natural Science Foundation of Ningxia Province (no. NZ17153; no. NZ11197).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.