
Abstract
Objective:
To compare the clinical effect of the self-made wire-rope button plate and cortical screw in the treatment of the distal tibiofibular syndesmosis separation.
Methods:
Total 26 patients with distal tibiofibular syndesmosis separation were treated with internal fixation with a self-made wire-rope button plate and cortical screw. They were divided into a self-made wire-rope button plate group and cortical screw group. self-made wire-rope button plate group: 12 cases of inferior tibiofibular syndesmosis were reconstructed by self-made wire-rope button plate. Cortical screw group: 14 cases of inferior tibiofibular syndesmosis were reconstructed by cortical screw. The follow-up data of 2, 6, 12 weeks and 6 and 12 months after operation were collected.
Results:
There was no significant difference in operative time, the amount of intraoperative bleeding and postoperative complications between the two groups (P > 0.05). Comparison of postoperative complications: There was no loosening and rupturing of internal fixation in the self-made wire-rope button plate group. In the cortical screw group, the rupture of screws was found in 1 case, which occurred in the 10th weeks after the operation, and the broken screws were removed after 1 year with other internal fixations. Within 12 weeks of reoperation to remove the internal fixation rate: There was a significant difference in the rate of reoperation to remove the internal fixation within 12 weeks (p < 0.05). At the last follow-up, the AOFAS score of the ankle joint were 94 ± 4.79 in the self-made wire-rope button plate group and 92.8 ± 6.73 in the cortical screw group. There was no significant difference (P > 0. 05).
Conclusion:
The self-made wire-rope button plate and cortical screw can effectively treat the separation of the tibiofibular syndesmosis. It provides a new choice for the treatment of inferior tibiofibular syndesmosis.
Introduction
Torsional violence to the ankle can lead to separation of the lower tibiofibular syndesmosis, which can occur alone or in combination with ankle fractures. At present, most scholars advocate lower tibiofibular syndesmosis screw fixation for the treatment of lower tibiofibular syndesmosis injury. 1,2 However, the cortical screw fixation has the risk of limiting the physiological micromotion of the tibiofibular syndesmosis, and the screw loosening and fracture occur in the later stage, which requires early secondary surgical removal. With the deepening understanding of the separation of the inferior tibiofibular syndesmosis and the development of internal fixation materials, the Endobutton plate and tightrope were applied to treating such injuries. 3 However, the internal fixation device is expensive and its use in primary hospitals is limited. Based on the Endobutton plate technology principle, we used the self-made wire-rope button plate to treat the separation of the lower tibiofibular syndesmosis and achieved satisfactory results.
Methods
General information
Structure and characteristics of the self-made wire-rope button plate: According to the technical principle of the Endobutton plate, the self-made wire-rope button plate consists of inner and outer clamps and one steel plate. The clamps are made of six-hole and or seven-hole phalangeal plates. The U-shaped cable is tightened and fixed after passing through the screw hole of the phalangeal plate. If the patient has a fracture of the fibula, the screw hole of the fibula plate can be crossed. After the self-made wire-rope button plate is fixed, the fibula can be pronated and supinated. Because of the gap between the tibia and fibula and the elasticity of the cable, the fibula can be slightly moved longitudinally, which conforms to the biomechanical characteristics of the lower tibiofibular syndesmosis. The mechanical strength of the cable is significantly better than that of the screw, which can avoid the complications such as loosening and screw breakage caused by the fixation of the cortical bone screw (Figure 1, Support Information 1).
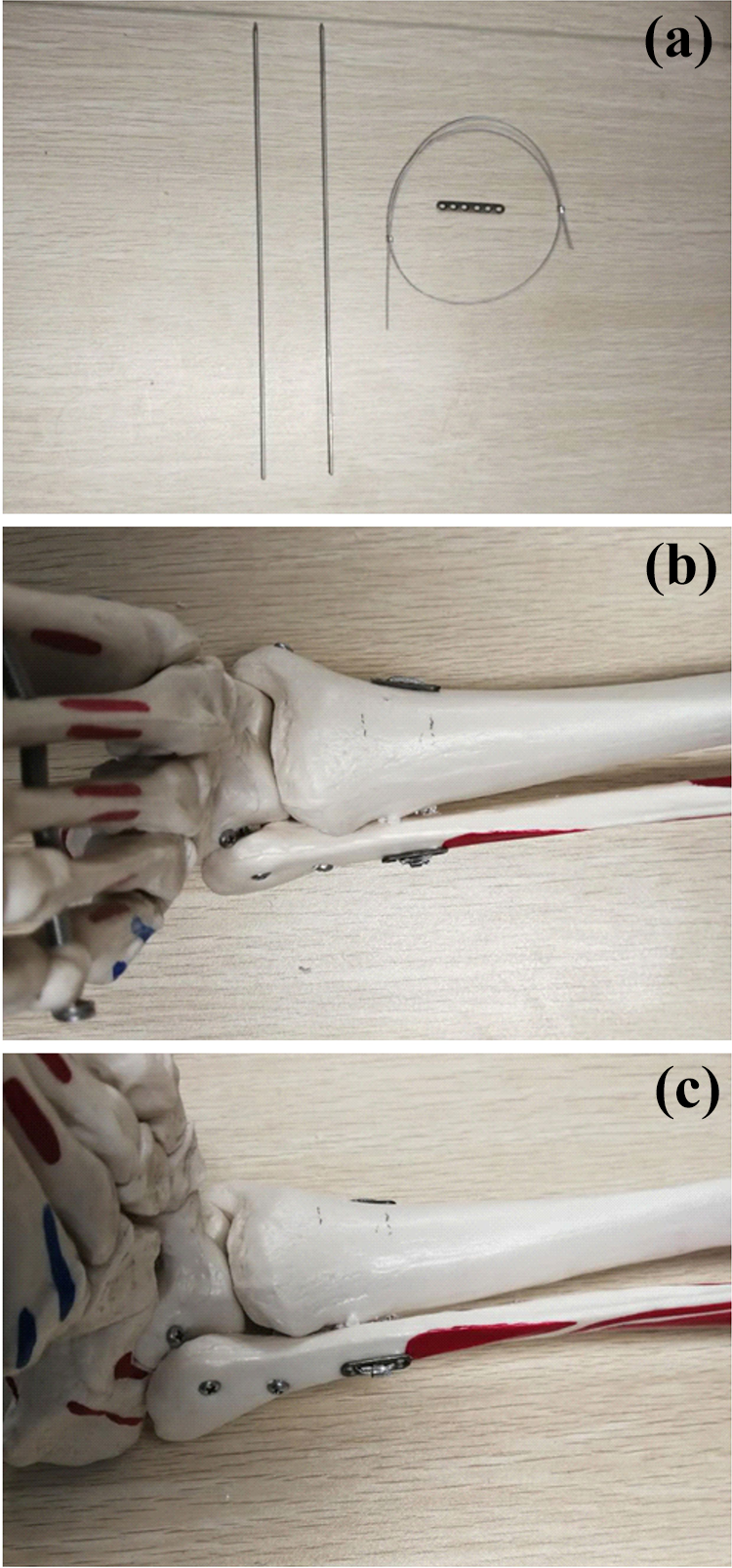
Components of the self-made wire-rope button plate and its fixation on the tibia and fibula. (a) is a component of the self-made wire-rope button platform. (b) and (c) are the fixation methods of the self-made wire-rope button plate on the tibia and fibula.
Patients
From May 2016 to February 2018, patients with distal tibiofibular syndesmosis separation who were treated in the first people’s hospital of Yibin city and the sixth hospital of Wuhan, affiliated hospital of Jianghan University with or without ankle fracture were selected. Inclusion criteria: ① Ankle radiographs showed widening of ankle points, lower tibiofibular syndesmosis space >6 mm or tibiofibular overlap <6 mm or positive intraoperative Hook test; ② Acute injury. Exclusion criteria: ① Open injury; ② Old fracture with ligament injury; ③ Combined with severe osteoporosis; ④ Pathological fracture.
According to the above criteria, a total of 26 patients were enrolled and divided into two groups according to the fixation method of the lower tibiofibular syndesmosis by random number table: the group with the self-made wire-rope button plate and the group with the cortical bone screw. Among them, 12 cases were fixed with self-made wire-rope and 14 cases were fixed with the cortical bone screw. The group with the self-made wire-rope button plate: eight males and four females; aged from 19 to 63 years, average (39.2 + 11.6) years; injury causes: nine cases of fall sprain, two cases of heavy pound injury, one case of traffic injury; injury classification: two cases of the isolated inferior tibiofibular syndesmosis, three cases of Danis-Weber type B, seven cases of type C; two cases were combined with fractures of other parts, including one case of rib fracture and one case of distal radius fracture; the time from injury to admission was 30 min–48 h, and eight cases were treated with calcaneal traction after admission. Cortical bone screw group: 10 males and 4 females; age range 20–72 years, average (42.2 + 12.8) years; injury causes: fall sprain in 10 cases, heavy pound injury in 2 cases, traffic injury in 2 cases; injury classification: isolated inferior tibiofibular syndesmosis in 1 case, 5 cases of Danis-Weber type B, 8 cases of type C; 1 case was complicated with fracture of other parts, including one fracture of the distal radius and one fracture of proximal humerus; the time from injury to admission was 1–72 h, and 8 cases were treated with calcaneal traction after admission. There were no significant differences in general data such as gender, age and injury type between the two groups (P > 0.05). This study has been reviewed by the Hospital Ethics Committee. All patients had signed a written informed consent before surgery.
Surgical procedures
Surgery in both groups was performed in the first people’s hospital of Yibin city and the sixth hospital of Wuhan by the same surgical process.
Anesthesia mode: epidural anesthesia or general anesthesia.
Surgical methods: patients were treated with upper balloon tourniquets in the supine or healthy lateral position, and a posterolateral incision of the ankle joint was used to expose and fix the fracture of the posterior ankle and lateral ankle, respectively. The medial malleolus fracture was exposed through an anteromedial arc incision and then fixed. We examined the stability of the inferior tibiofibular syndesmosis by the intraoperative Hook test. In case of instability, we used bone tenaculum to clamp the tibiofibular at the tibiofibular syndesmosis so that the tibiofibular was repositioned or positioned satisfactorily. Then, about 2–4 cm above the ankle joint, Kirschner wires parallel to the ankle joint and inclined 30 degrees forward were used to fix, requiring that the Kirschner wires must pass through the center of the fibular marrow cavity. The lower tibiofibular syndesmosis was fixed in two groups as follows:
① Self-made wire-rope button plate group: Two 2.0 Kirschner wires were used to fix the lower tibia and fibula, then one Kirschner wire was removed and the cable was passed from the fibula to the tibia side along its channel. A 2–3 cm incision was made in the anteromedial part of the tibia at the exit of the drill hole, and the prepared three-hole steel plate was placed longitudinally. After the cable passed through the steel plate, the cable passed through another drill hole to the fibula side and fixed another three-hole steel plate. Placed the patient’s foot in dorsal extension and 95–100 degrees with the tibia, tightened the cable and fixed it (Figure 2a–e). When the patient can tolerate the pain, the ankle joint active flexion and extension functional exercise can be started, and early weight-bearing activities can be carried out. The self-made wire-rope button plate can be removed after 1 year with other internal fixation devices or not.

Surgical procedure in which the self-made wire-rope button plate is fixed to the tibia and fibula. Two 2.0 Kirschner wires were implanted at about 2-4cm above the ankle joint in the direction parallel to the ankle joint and tilted forward 30 degrees. A: Anteroposterior position after implantation. B: Anteromedial position after implantation. C: Pull out a Kirschner wire and implant the cable into the fixation channel. D: The steel plates of inner and outer loops are placed and locked on the inner side to fix the steel cables. E: Anterolateral position after implantation. F: The latch is located on the outside. G: Picture of the front inside with the latch on the outside.
② Cortical bone screw group: Four layers of cortex were fixed with two 3.5 mm diameter cortical screw that could or could not pass through the fibular plate screw hole. Active ankle flexion and extension exercise was started when the patient could tolerate pain, and partial weight-bearing activity was started at 6–8 weeks. The inferior tibiofibular syndesmosis cortical screw was removed at 12 weeks after surgery.
There were three cases of a medial deltoid ligament injury in the two groups, respectively. After the reduction and fixation of the lateral malleolus, the position of the ankle joint was good and was not explored and repaired. There were no cases with infection after surgery in both groups.
Evaluating indicator
The operation time, intraoperative bleeding volume, postoperative complications, and internal fixation rate after reoperation within 12 weeks were compared between the two groups, and the follow-up data at 2, 6, 12 weeks, 6 and 12 months after operation were collected. The ankle function score was determined by the American Orthopaedic Foot and Ankle Society (AOFAS). 4
Statistical analysis
SPSS 20.0 statistical software was used for statistical analysis. The measurement data were expressed as mean and standard deviation (Mean ± SD), t-test was used for comparison. Count data were expressed as the number of cases and percentages, and χ2 test was used for comparison between groups. P < 0.05 was considered as statistical significance.
Results
There were no significant differences in operation time, intraoperative blood loss and postoperative complications between the two groups (P > 0.05, Table 1). All patients were followed up and all incisions healed in phase I. No loosening or fracture of internal fixation occurred in the self-made wire-rope button plate group, and 1 case had limited dorsal extension, which led to squatting difficulty. After removing the loop cable device 12 weeks later, squatting symptoms improved significantly. In the cortical bone screw fixation group, one case had a fracture of the lower tibiofibular screw at the 10th week after the operation, which was removed when the internal fixator was removed after fracture healing. At the 12th month follow-up, the AOFAS score of ankle joint in the self-made wire-rope button plate group was 94 ± 4.79, and that in the group with the cortical bone screw was 92.8 ± 6.73. There was no significant difference between the two groups (P > 0.05).
Comparison of operative time, intraoperative bleeding volume and postoperative complications between the two groups.

In the self-made wire-rope button plate group, the loop cable was taken out at 12th week in one patient. Two patients had the discomfort of ankle joint tension. After physical therapy, the symptoms improved, but no internal fixation was taken out. In other cases, the fixators were removed together with other internal fixators 1 year later. In the group of cortical bone screw fixation, one case had screw fracture, and the fixation was taken out together with other internal fixations 1 year later. The internal fixators of other cases were taken out at 12 weeks. The difference between the two groups was statistically significant (P < 0.05, Table 2).
Reoperation and internal fixation removal in two groups within 12 weeks.

Note: The price of a bone screw is 50¥, and the Endobutton is 9800¥. The removal of these internal fixations is usually performed in day surgery and costs about 500 ¥.
Discussion
Ankle torsion violence is very common in daily life. Pronation-external rotation and pronation-abduction are most likely to lead to the injury of the tibiofibular syndesmosis, but supination-external rotation is rare. Torsional violence results in talus abduction or external rotation in the ankle point, causing tibiofibular syndesmosis injury. 5 It has been reported that talus was displaced 1 mm and articular surface coverage was reduced by 42%, 6 resulting in ankle pain, functional degeneration, traumatic arthritis. If improperly treated or missed diagnosis, it often brings physical and mental pain to patients. Therefore, it is important to restore the anatomical relationship of the inferior tibiofibular syndesmosis and maintain its stability.
In clinical work, the separation of the inferior tibiofibular syndesmosis is mainly determined by X-ray and CT. Tibiofibular space >5 mm on anteroposterior X-ray film, tibiofibular overlap <10 mm on anteroposterior X-ray film or <1 mm on ankle acupoint X-ray film, that is, the presence of inferior tibiofibular separation. 7 This is a relatively broad and recognized standard. However, there are differences in the depth of the inferior tibiofibular notch, so the bilateral comparison is recommended to improve the accuracy. CT examination can make the bilateral comparison to judge whether the ligament is broken by the widening of the lower tibiofibular syndesmosis. It has been reported that the application of MRI in the diagnosis of lower tibiofibular syndesmosis injury, 8,9 but the price of ankle joint MRI examination is expensive, the equipment requirements are high, and the wide application is limited. In this study, X-ray and CT examinations were performed before surgery and the Hook test was performed intraoperatively in patients suspected of distal tibiofibular syndesmosis separation. After fixation of the medial and lateral malleolus fractures, the patient’s fibula was clamped with a bone tenaculum, and lateral stress was applied. Under ankle acupoint fluoroscopy, if the patient has a lateral displacement of the inferior tibiofibular syndesmosis of more than 3–4 mm, the instability should be considered and the inferior tibiofibular ligament should be fixed surgically.
Surgical treatment is currently recommended for patients with definite distal tibiofibular syndesmosis separation. 10 Anatomical reduction of the lateral malleolus and reduction of the lower tibia and fibula must be ensured simultaneously for fixation of the lower tibia and fibula. In the past, the cortical screw was used to fix the inferior tibiofibular syndesmosis, but it limited the physiological micromotion of the inferior tibiofibular joint in the early stage, and the risk of screw loosening and fracture may occur in the later stage. 11 In order to avoid screw breakage, it is generally necessary to remove the cortical screw in about 12 weeks after surgery. Removal of cortical screw earlier than 6 weeks may lead to limited ankle stability due to poor healing of the lower tibiofibular syndesmosis. Removal of the cortical screw after 12 weeks may affect ankle function due to the disappearance of tibiofibular physiological micromotion, and the risk of screw loosening and fracture is great. In this study, 1 case of fracture of the inferior tibiofibular screw occurred in the cortical bone screw group at the 10th week after the operation, and the internal fixator was removed when the fracture healed. Based on the problems of screw fixation, more and more scholars have proposed the use of elastic fixation (e.g. Endobutton system) for the treatment of inferior tibiofibular syndesmosis. 12– 16 This fixation method is more in line with physiological micromotion, which can promote more stable healing and avoid secondary surgery. 17 However, such expensive instruments are lacking in primary hospitals, and more inexpensive and reliable internal fixation materials need to be further developed. Degroot et al. 18 used button suture in the treatment of acute lower tibiofibular syndesmosis injury. Although there were complications such as local stimulation, osteolysis, heterotopic ossification and so on, the average AOFAS score was 94 points, indicating that button suture technique is an effective method for the treatment of lower tibiofibular syndesmosis injury, but the secondary surgery rate caused by its complications was higher than expected.
In this study, a simple self-made wire-rope button plate was made according to Endobutton’s technical principle for the treatment of inferior tibiofibular syndesmosis separation. The device has strong stability, can provide reliable fixation, while retaining the micromotion function of the inferior tibiofibular syndesmosis, so that the injured inferior tibiofibular syndesmosis can restore its physiological state. Because of its stable and reliable fixation, patients can take early weight-bearing exercises. The self-made wire-rope button plate has the advantages of a low probability of internal fixator fracture and no need for early surgical removal. Especially in obese and osteoporotic patients, the advantages are more obvious, because these patients have a greater risk of cortical screw fracture and loosening. In this study, the AOFAS score of the self-made wire-rope button plate group was higher than that of the cortical screw group, and the weight-bearing activity could be achieved in the early stage without loosening or fracture of the internal fixation. The fixation was stable and reliable. Although there were two patients with ankle tightness and discomfort, the symptoms improved after physical therapy. Only one patient had limited dorsal extension, which led to squatting difficulties. After removing the self-made wire-rope button plate at 12 weeks, squatting symptoms improved significantly. The reason for this was that the talus was wide anteriorly and narrow posteriorly, and the compression of the steel cable was too tight, which limited the dorsal extension of the ankle joint. Therefore, it is recommended to tighten the cable in the 95–100 degrees dorsal extension position of the foot when using the self-made wire-rope button plate to treat the separation of the lower tibiofibular syndesmosis, and the pressure should not be too large. There was only one case of reoperation and internal fixation removal within 12 weeks in the self-made wire-rope button plate group, which occurred in the early stage of this study. There was a significant difference in the rate of reoperation and internal fixation removal within 12 weeks between the two groups. The use of the self-made wire-rope button plate reduced the number of operations, and alleviated patient suffering. In addition, the cost of our self-made plate was much cheaper than that of Endobutton. The steel plate was about 1000 yuan, and the wire-rope was about 800 yuan, which was much lower than the cost of Endobutton, which was about 10000 yuan. The significant lower price of the self-made wire-rope button plate greatly alleviated the economic burden of patients and was conducive to the promotion of clinical application. The price of a bone screw is 50¥, and the Endobutton is 9800¥. The removal of these internal fixations is usually performed in day surgery and costs about 500 ¥.
This study provides new options with lower cost and easier operation for the surgical treatment of patients with lower tibia and fibula separation. Also, it overcame the disadvantages of fibula rotation and shortening. Even so, there are some limitations of this study. First, it is a preliminary study from a single center. Large random controlled trial from multiple centers are needed to further confirmed the results. Second, the sample size of this study is relatively small, which will be enlarged in future studies. Third, the strength of cable tightening depends on the individual differences of different patients, which is difficult to define accurately.
Conclusion
The self-made wire-rope button plate device is cheap, easy to operate and easy to popularize in primary hospitals. However, further studies are needed to summarize the fixed angle of the device, the spacing between placement, the strength of locking and tightening, and the specific angle of ankle dorsal extension. These will be further refined in future studies.
Footnotes
Availability of data and materials
All data and materials regarding the study are available from the corresponding author.
Author contributions
XKW and GWJ contributed to the study design and drafting of manuscript. YS and JHW contributed to statistical analysis and drafting of the manuscript. JT contributed to the literature search and revision of the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
This study was approved by the Affiliated Hospital of Jianghan University and conducted in compliance with the Helsinki Declaration. Written consent was acquired for all patients.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.