
Abstract
Study background:
A retrospective study to compare the rate of facet joint violation (FJV) in lumbar posterior spinal instrumentation using open pedicle screw, percutaneous pedicle screw, and cortical bone trajectory (CBT) technique. CBT is a new posterior spinal instrumentation technique in which a more caudal entry point can minimize iatrogenic damage to the cranial facet joint. Only one recent study reports incidence of FJV of 11%; however, no previous reports comment on radiological outcomes comparing to traditional open and percutaneous screws.
Methods:
We reviewed 90 patients who underwent lumbar posterior spinal instrumentation from January 2016 to June 2017. Postoperative computer tomography scans were performed to evaluate FJV. Incidence of FJV was graded by three reviewers according to Seo classification.
Results:
Totally, 446 screws (open 43.4%, percutaneous 37.8%, CBT 18.9%) were inserted. Among these, 6.3% (28/446) had screw head or rod in contact with facet joint and 0.9% (4/446) had screws directly invaded the facet joint. Overall, FJV was 7.2% (CTB = 3.4%, open = 10.4%, and percutaneous = 4.5%, p = 0.075).
Conclusion:
CBT technique has potential advantage in reducing FJV. It has a unique entry site at lateral aspect of pars interarticular with a caudomedial to craniolateral pathway. It is a reasonable alternative to open or percutaneous techniques in lumbar posterior spinal instrumentation.
Introduction
Lumbar posterior spinal instrumentation represents an effective surgical intervention for patients with spondylolisthesis, degenerative disease, spinal deformity, spinal tumor, and spinal fracture. 1 The pedicle screw and rod system became standard instrumentation for the procedure. Open pedicle screw and percutaneous pedicle screw are the two conventional insertion techniques. However, there is increasing concern about adjacent cranial FJV during placement of the proximal pedicle screw.
The development of pathology at the mobile segment next to a lumbar or lumbosacral spinal fusion has been termed adjacent segment disease. It is considered a potential late complication of spinal fusion that can necessitate further surgical intervention and adversely affect outcomes especially postoperative pain or major failure of spinal fusion surgery. 2,3 Potentially modifiable risk factors for the development of adjacent segment disease include fusion without instrumentation, protecting the facet joint of the adjacent segment during placement of pedicle screws, fusion length, and sagittal balance. For the part of FJV during screw insertion, previous studies have reported various rates ranging from 4% to 100% (Table 3). Babu et al. 10 revealed incidence of FJV as high as 34% and 40% for open and percutaneous techniques, respectively.
Recently, cortical bone trajectory (CBT) screw technique, which was first advocated by Santoni et al., 14 has been developed as an alternative to the conventional techniques for lumbar spinal instrumentation. CBT starts at the lateral aspect of the pars interarticularis and inserts in the craniolateral pathway so that the highest density of cortical bone is anchored. By inserting through a more caudomedial entry point, muscle dissection and iatrogenic injury to cranial facet joint can be minimized. Keitaro et al. reported FJV of 11.8% secondary to CBT technique. 13 A few recent studies have also shown good clinical results of CBT in terms of functional and radiological outcomes. 15,16 It is believed that CBT rarely causes FJV. However, to our best knowledge, no previous studies comparing the incidence of FJV of CBT to open pedicle screw and percutaneous pedicle screw has been shown so far.
Materials and methods
In the study period between January 2016 and December 2017, we identified 93 patients who underwent lumbar pedicle screw instrumentation using open pedicle screw, percutaneous pedicle screw, and CBT. Patients with a history of previous spinal surgery distorting facet anatomy were excluded. Totally, 90 patients were evaluated for cranial FJV, including 39 males and 51 females with a mean age of 67 years. There were 71 patients with spondylosis, 16 patients with lumbar vertebral fracture, and 3 others (Table 1).
Demographic data.
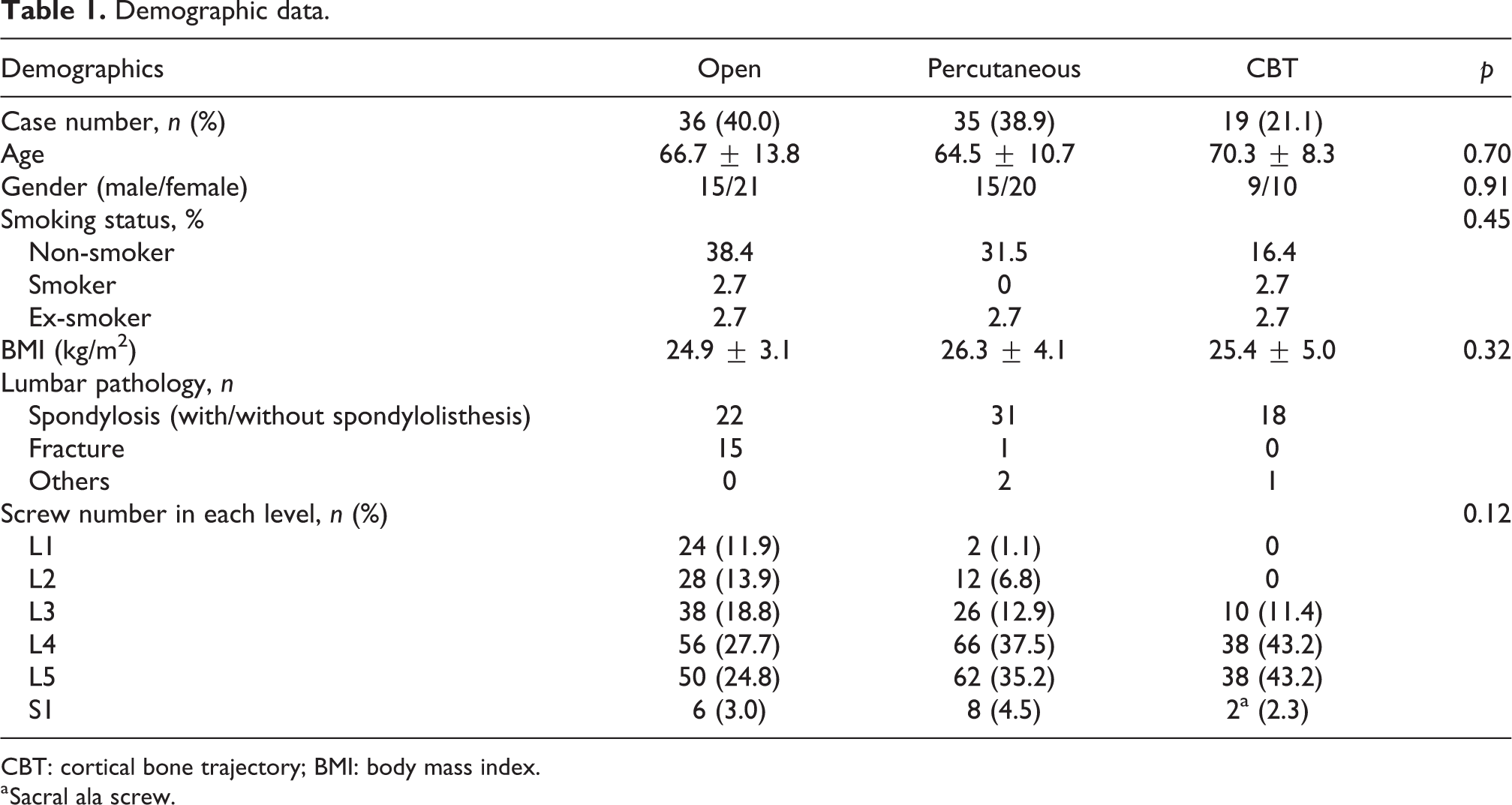
CBT: cortical bone trajectory; BMI: body mass index.
a Sacral ala screw.
Surgical techniques
All surgeries were performed by a single team of orthopedic surgeons using the same operative technique. Patients were under general anesthesia and positioned prone on a radiolucent table.
In open pedicle screw insertion, a midline longitudinal incision was made to expose the corresponding lumbar spine. Muscle and soft tissue dissection was performed up to the junction of the transverse process and lateral wall of the facet joint. The superficial cortex of the entry point was opened with an awl and a pedicle probe was used to navigate the trajectory. Fluoroscopic guidance was used if necessary. The screw was then inserted into the same trajectory created or after tapping if necessary.
In percutaneous screw insertion, the correct spinal level was confirmed with fluoroscopy. The skin incision was lateral to the image projection of the pedicle. After blunt dissection, cannulated needles were inserted followed by the guide wire. Tapping was performed until reaching the center of the vertebral body and screw was inserted subsequently.
In CBT screw insertion, a midline longitudinal incision was made to expose the corresponding lumbar spine. Dissection was performed until the lateral aspect of the pars interarticularis was identified and it was the entry point for CBT. 17 The entry hole was made using 2-mm high-speed round burr drill, directed laterally in the axial plane and cranially in the sagittal plane under fluoroscopic guidance (Figure 1). Pedicle marker pin was placed into the hole and the position was confirmed with fluoroscopy followed by tapping into the size of a planned screw. Screw insertion was then performed and the final position was confirmed with fluoroscopy.

Illustrations on CBT screw insertion with the entry point being a solid circle and trajectory being an arrow. (a) axial view, (b) posterior view, and (c) sagittal view.
Evaluation of FJV
FJV was evaluated using postoperative computed tomography that was performed routinely 6 months after operation in all patients to assess screw position relative to the cranial facet joint (Figure 2). Incidence of FJV was evaluated according to the classification described by Seo et al. 18 in which grade 0 = no violation, grade 1 = screw head or rod in contact with facet joint, grade 2 = screw directly invaded the facet joint (Figure 3). FJV was graded blindly by three observers. Consensus grade was considered when two or more observers agreed on the violation status.

Axial images showing direction of screw insertion using different techniques. (a) Open, (b) Percutaneous, and (c) CBT.
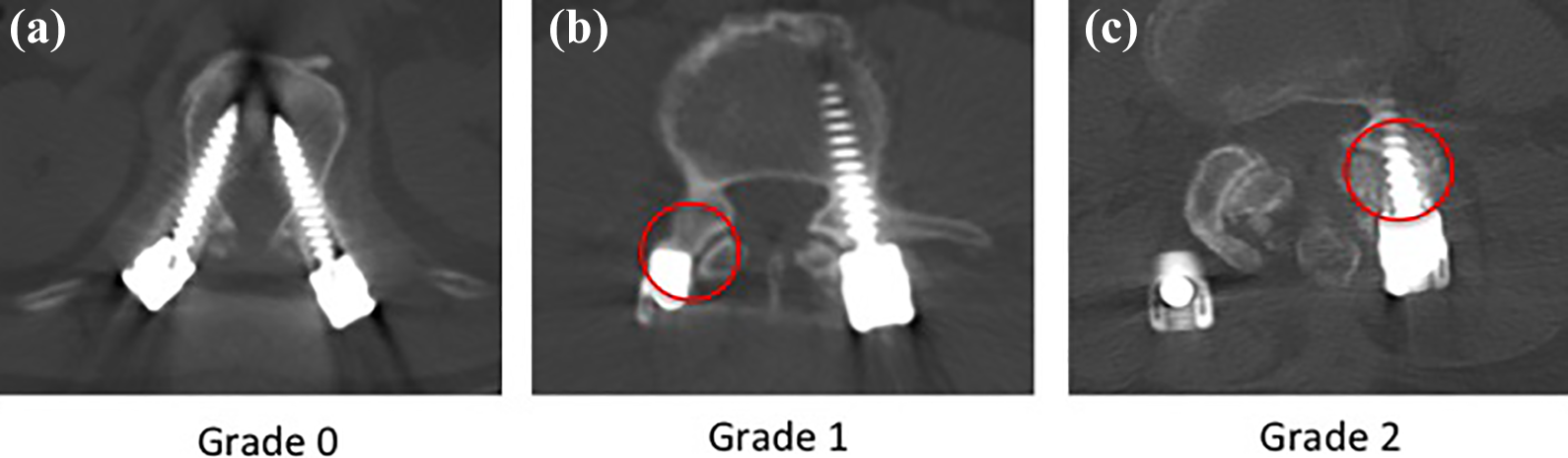
Axial images showing grading of Seo classification 18 . (a) grade 0, (b) grade 1, and (c) grade 2.
Statistical analysis
SPSS software version 24.0 was used for all data analysis. All results are expressed as mean ± standard deviation. Chi-square tests were used for ordinal and nominal variable while Student t-tests were used for continuous variables. Two-sided p values <0.05 were considered to be statistically significant.
Results
Totally, 446 screws were inserted in 90 patients with bilateral screw fixation in which 202 was open, 176 was percutaneous, and 88 was CBT. Using the consensus grades, the overall FJV was 7.2% (32/446). Among these, 6.3% (28/446) had screw head or rod in contact with facet joint (grade 1) and 0.9% (4/446) had screws directly invaded the facet joint (grade 2). The open technique had the highest cranial facet violation of 10.4% (21/202) (grade 1 = 8.9%, grade 2 = 1.5%) among the three groups. Percutaneous technique had FJV of 4.5% (8/176) (all grade 1) and CTB technique had FJV of 3.4% (3/88) (grade 1 = 2.2%, grade 2 = 1.2%) (Figure 4). There was no statistical significance among the three screw fixation techniques (p = 0.075) (Table 2).
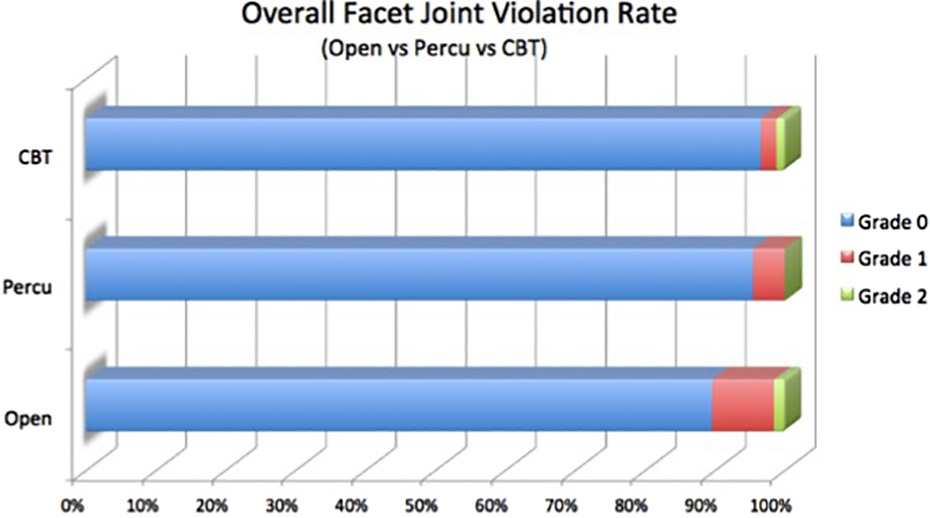
Graph showing the overall FJV rate using open, percutaneous, and CBT techniques. FJV: facet joint violation; CBT: cortical bone trajectory.
Facet joint violation.
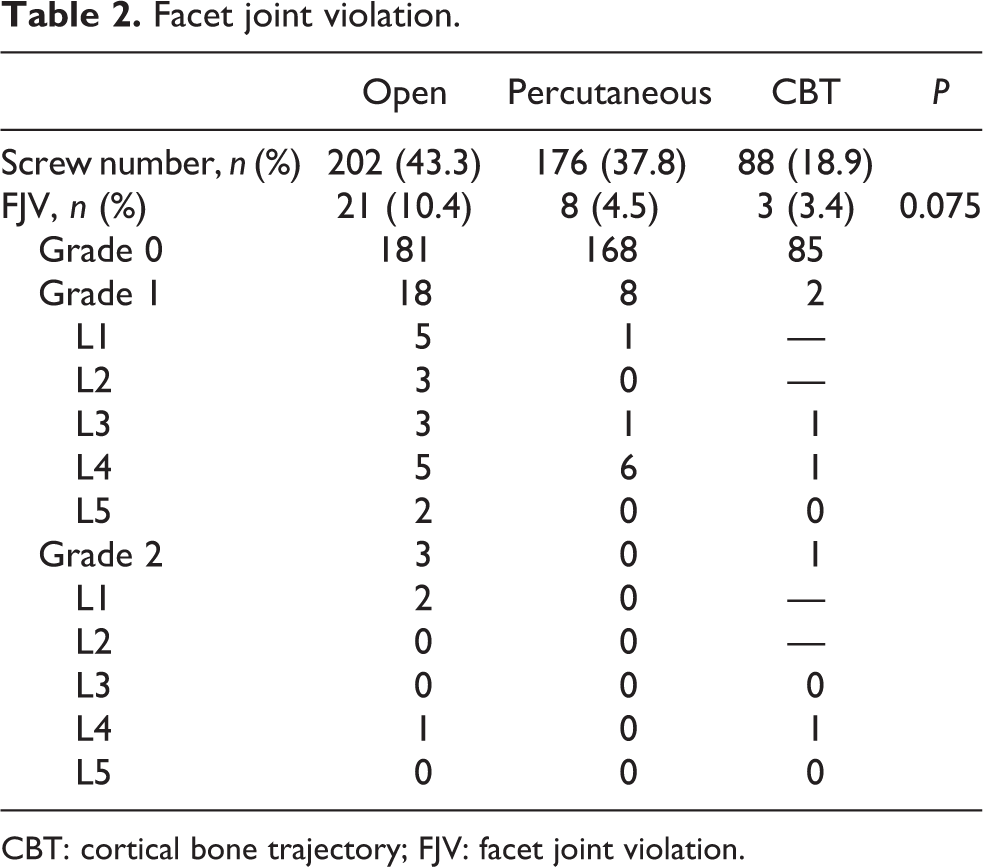
CBT: cortical bone trajectory; FJV: facet joint violation.
Discussion
Currently, most studies on pedicle screw insertion in lumbar spinal instrumentation emphases on fixation strength and accuracy of screw placement within the pedicle. 19,20 However, screw fixation with screw placing within a pedicle can cause impingement on cranial facet joint which leads to adjacent segmental degeneration after spinal fusion. In a biomechanical cadaveric study, Kim et al. 21 report increase in facet contact force and intradiscal pressure in the finite element model after FJV by screw insertion. Cardoso et al. 22 also showed an increase in the cranial facet joint motion due to the additional insult by the screw. Literature review had shown that symptomatic adjacent segment disease ranged from 5.2% to 18.5% in postoperative follow-up of 44–164 months. 2 The rate was higher in patients with transpedicular instrumentation and the potential risk factors included fusion length, sagittal malalignment, facet injury, instrumentation, and pre-existing degenerative changes. Therefore, it is important to identify strategies to minimize cranial FJV.
The previous studies report a widely varying incidence of FJV in open, percutaneous, and CBT techniques (Table 3). Our results showed the incidence of FJV by open and percutaneous technique was 10.4% and 4.5%, respectively. These violation rates were relatively low compared with those reported in the literature that was 15% to 100% using traditional open technique and 4% to 58% using the percutaneous technique. In theory, the further the entry point away from the facet joint, the lower the risk of FJV is. In the open technique, in order to obtain a lateral enough entry point, adequate soft tissue dissection is necessary and it is highly limited by muscle retraction. This is not problematic in the percutaneous technique as muscle dissection is not required. Therefore, an open technique generally has a higher incidence of FJV and it is reflected in most studies and also our result. Yson et al. 12 reported even a lower rate of 4% incidence of FJV with the percutaneous technique using intraoperative computed tomography (CT) imaging (O-arm) and a navigation system.
Summary of Studies on FJV.
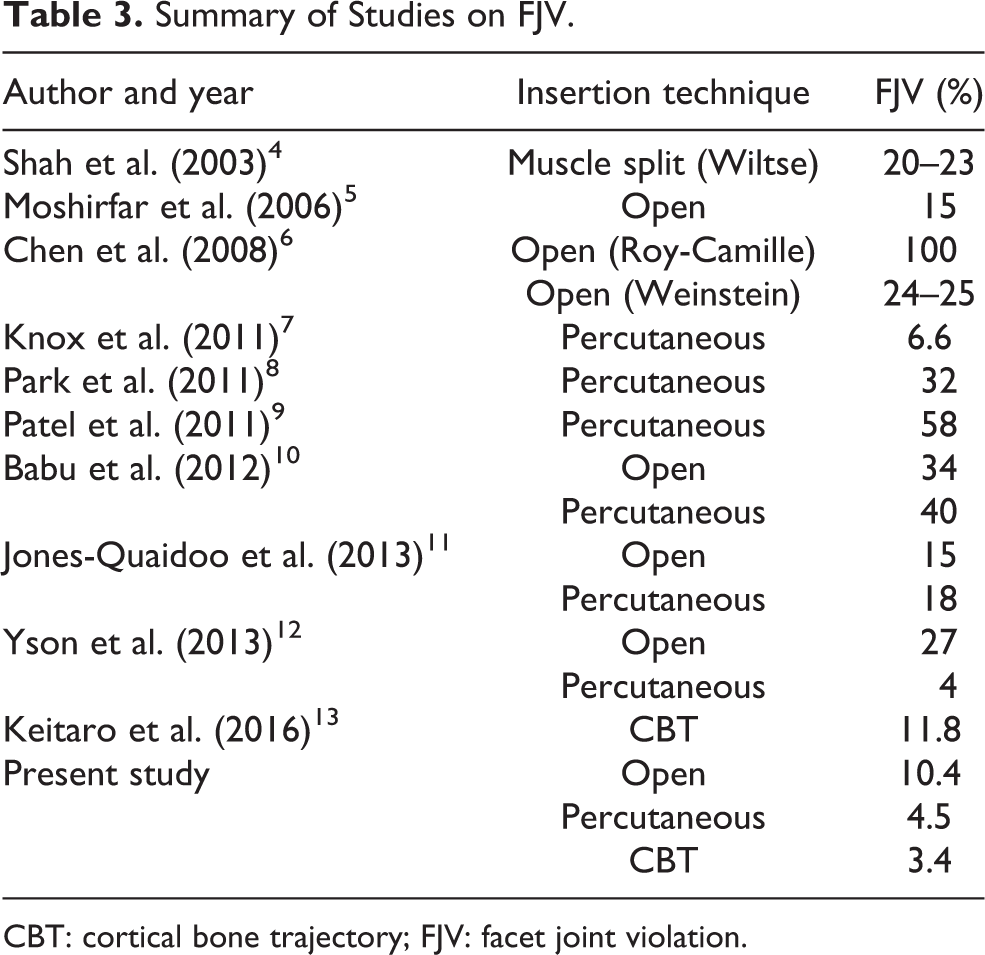
CBT: cortical bone trajectory; FJV: facet joint violation.
Our study showed CBT technique had a remarkably low incidence of FJV of 3.4% including one case of direct FJV. Comparing to the study of Keitaro et al. 13 which was the first one evaluating FJV using CBT, they reported FJV of 11.8% with no occurrence of intra-articular violation after reviewing 202 consecutive patients. They also performed CT measurement on screw position and revealed the importance of selecting sufficiently caudal entry point after exposing the pars interarticularis, and placing the screw head away from the dorsal lamina to maintain a safe distance from the cranial facet joint with extra 5 mm adding to the measure screw length. These are essential points taking into account during screw insertion as well in order to reduce the risk of FJV.
It is believed that CBT technique has a reasonably low risk of cranial FJV due to its unique entry starting at the lateral aspect of pars interarticular and following a caudomedial to a craniolateral pathway, staying away from the facet joint. Our study showed CBT technique has the lowest incidence of FJV compared to open and percutaneous techniques (p = 0.075). Although the study did not give statistical significance on FJV, CBT technique for pedicle screw fixation has been proven more advantageous than traditional approaches. 15 CBT screw insertion had been shown to have good clinical outcomes. It is less invasive and requires less muscle dissection and retraction particularly leading to a reduction in blood loss, postoperative pain and duration of hospitalization, and an enhancement of postoperative recovery. In 2017, Brahim et al. demonstrated statistically significant reductions in back pain and leg pain visual analog scores, and Oswestry Disability Index in series of 18 patients undergoing L4/5 posterior lumbar interbody fusion with 3D-navigation guided CBT at a minimum of 12 months postoperatively. 8
Also, CBT may reduce injury to neurovascular structures close to the pedicle including nerve roots, dural sac, and anterior blood vessels due to the laterally directed trajectory in the transverse plane, meaning it is a safer profile for screw insertion. Mizuno et al. reported no cases of surgery-related spinal nerve injury or neurological deficits from a retrospective analysis of 12 patients with single-level lumbar spondylolisthesis who underwent posterior or transforaminal lumbar interbody fusion surgery using CBT screws. 23 In addition, CBT screws are proven to have better biomechanical fixation in osteoporotic lumbar spine compared with standard pedicle screws. 24
There are few relative contraindications about CBT screw insertion. 25 It is not recommended for long construct greater than three levels. Orientation CBT screw is unique at each level and it is difficult to align rods to connect multiple levels together for spinal fusion. Also, CBT is usually not used in narrow or medialized pars, and congenitally small pedicles since it is technically demanding for put the screws accurately.
In our study, there was one case of screw direct invasion to cranial facet joint using CBT technique and this was out of expectation in view of the superior cortical trajectory. Interestingly, the FJV was not due to the screw insertion itself but due to bone morphogenetic protein-induced bone osteolysis after the operation. Osteolysis caused instability of adjacent spinal level, therefore, migration of screw causing intra-articular violation of facet joint (Figure 5).
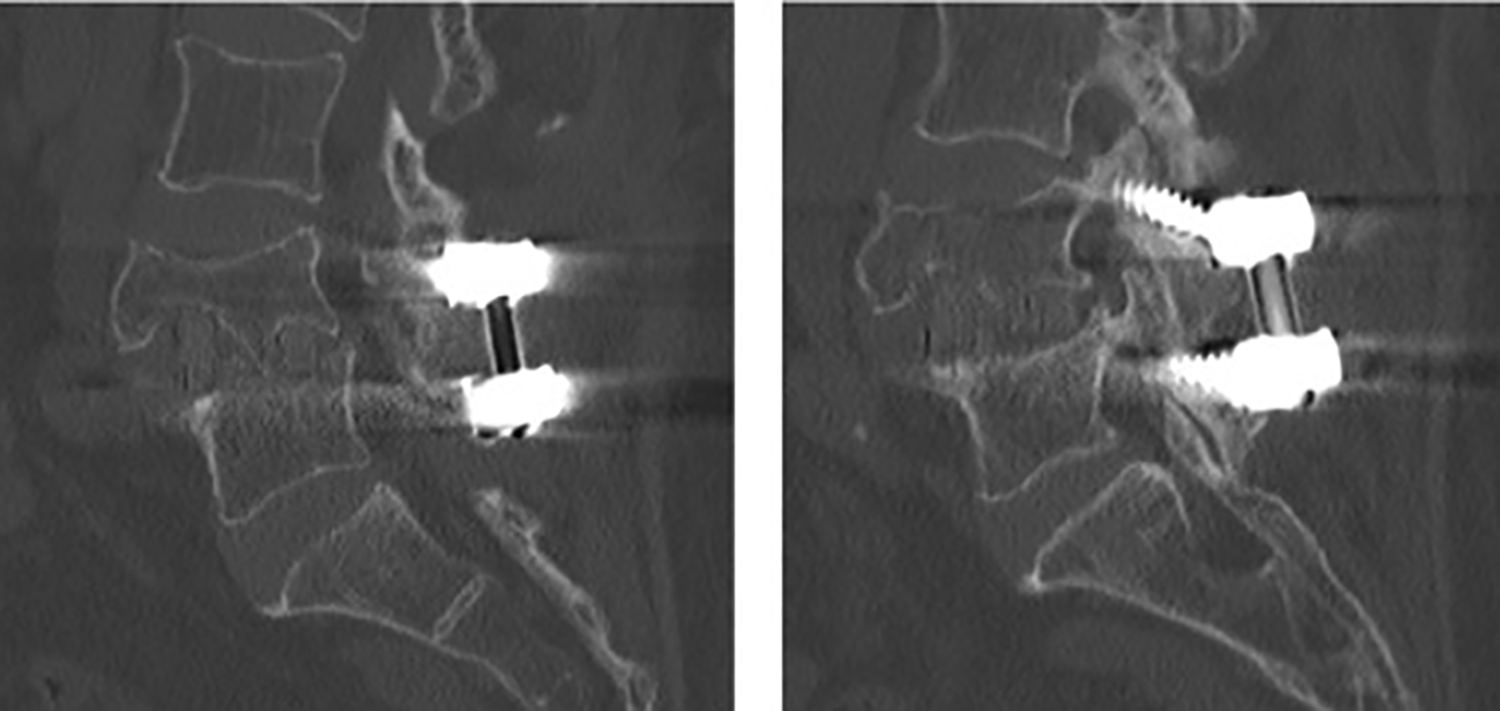
Sagittal images showing osteolysis of L4 vertebral body and direct invasion of cranial facet joint by the screw shaft.
There were several limitations to our study. First, it is the nonrandomized study design which may cause potential selection bias. CBT technique was only used in L3–S1 lumbar instrumentation due to the anatomical variance among lumbar vertebrae for ease of screw insertion. This may give a falsely lower risk of FJV. Second, the influence of FJV on the clinical outcome due to adjacent segmental degeneration is unknown. Clinical parameters should be measured to evaluate the impact of different degree and magnitude of FJV between open, percutaneous, and CBT techniques.
Conclusion
CBT technique has a potential advantage in reducing FJV. It has a unique entry site at the lateral aspect of pars interarticular with a caudomedial to a craniolateral pathway. It is also a safe approach with minimal muscle dissection and retraction with a small chance of iatrogenic damage to neurovascular structures or dura. Therefore, it is a reasonable alternative to open or percutaneous techniques in lumbar posterior spinal instrumentation.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.