
Abstract
Achieving a well-balanced total knee arthroplasty (TKA) is a difficult task, but the use of real-time sensing technology could provide intraoperative dynamic feedback regarding stability and load. This study compared intraoperative data and clinical outcomes between two cohorts, where one cohort had a sensor-guided medial pivot TKA performed.
Methods:
Two cohorts of 50 patients each were preoperatively matched to receive the same TKA, having a J-curve femoral design with an adapted “medially congruent” polyethylene insert; the second cohort (group B) underwent the intraoperative sensor-check. Intraoperative sensor data were recorded as tibiofemoral load at 10°, 45°, and 90°. We considered stable knees those with a pressure <50 lbs on the medial compartment, <35 lbs on the lateral, and a mediolateral inter-compartmental difference <15 lbs. Clinical outcomes were evaluated according to the Oxford Knee Score (OKS) and Knee Society Score (KSS).
Results:
All patients (group A: no sensor; group B: sensor) were available at 2-year minimum follow-up (FU; min. 24 months, max. 34 months); no preoperative statistical differences existed between groups in the average range of motion (ROM), OKS, KSS, and body mass index. There were no statistical differences at final FU between groups in the average OKS (group A: 41.1; group B: 41.5), in the average KSS (group A: 165.7; group B: 166.3), or in final ROM (group A: 123°; group B: 124°). One patient in each group required a manipulation under anesthesia. In the sensor group, an accessory soft tissue release/bone recut was necessary after sensor testing with trial components in 24% to obtain the desired loads; in the same group, the level of constraint in the final components was increased to posterior-stabilized in 12% because of an inter-compartmental difference >40 lbs. Surgical time was 8 min longer in the sensor group.
Conclusion:
The use of this sensing technology did not improve the clinical outcome but supported multiple intraoperative decisions aimed to better reproduce the medial pivot kinematic of the normal knee.
Introduction
Total knee arthroplasty (TKA) has proven to be effective in significantly reducing osteoarthritic knee pain and more cost effective than prolongation with nonsurgical treatments. 1 Despite the use of third-generation implants, results still show almost 20% of patients are unsatisfied. 2 –6 Several biomechanical and anatomical studies confirmed a medial pivot pattern in the human knee, showing different anatomical geometries between the knee compartments, with a concave shape on the medial plateau and a convex shape for the lateral side 7,8 ; a difference between the two compartments in terms of loads during normal walking has been shown too. Similar reports showed that 60% of the body weight is transferred through the medial side of the knee during normal gait and that the medial stability of the knee is dynamically guaranteed by the soft tissue structures. 9
A few modern TKA implants have been designed in order to reproduce the normal kinematics of the knee by mimicking the physiological medial pivoting pattern, with a greater conformity on the medial compartment between tibial insert and femoral condyle and an inferior congruency on the lateral side. 10,11 Despite these advancements in TKA design, which aimed to reproduce a more anatomical kinematic, there is evidence that implant design plays a minor role in the final outcome as opposed to a precise surgical technique. 12 Therefore, proper balancing of soft tissue has become of primary importance as it is estimated that improper balancing causes up to 35% of TKA revisions in the United States. 13 –15 To address this problem and to make ligament balancing less operator dependent, several advances in technology have been proposed over the past decades. Among the most used are computer-assisted surgery, patient-specific instrumentation, and intraoperative pressure sensors, which represent very appealing instruments. 16 The “load-sensing” solution is a relatively recent one, consisting of two microelectronic sensors embedded into the tibial tray that allow for dynamic, in vivo evaluation of joint loading and peak center of load location; using this technology, the surgeon receives a real-time feedback of the loading in the knee and is able to adjust any imbalance with additional bony resections or soft tissue corrections. 17,18 The authors of the current study hypothesized that the use of sensor technology would help reproduce the normal medial pivot knee kinematics without improving clinical outcome. In fact, it is our opinion that this technology can help to balance any TKA in a slightly asymmetric way, obtaining a medial compartment slightly tighter than the lateral compartment, both in extension and in flexion. The authors also hypothesized that this technology would help to intraoperatively replicate the physiological medial pivoting biomechanics of the natural knee and reduce the risk of a mid-flexion instability. 19
Materials and methods
This was a prospective, matched-pair case–control study of patients who underwent primary TKA using the same medially congruent (MC) design (Persona MC; Zimmer-Biomet, Warsaw, Indiana, USA) with a minimum of 2-year follow-up (FU). This study has been performed in line with ethical guidelines set by The Declaration of Helsinki and its later adaptions. This study received approval from the authors Institution (Stanford University IRB 4947). All participants in this study were fully informed and provided their informed consent for participation.
The main inclusion criteria were age between 45 years and 85 years and primary degenerative knee osteoarthritis (OA) graded 3 or 4 according to the Kellegren–Lawrence classification, 20 not responsive to conservative treatment, leading to neutral alignment, or varus deformity less than 20° on the mechanical axis. Exclusion criteria included any preoperative diagnosis of inflammatory or post-traumatic OA of the knee, body mass index (BMI) greater than 45, or symptomatic hip or back pathologies. The matching criteria were set as age, BMI, preoperative range of motion (ROM), gender, and the Knee Society Score (KSS) 21 and Oxford Knee Score (OKS). 22
After 1:1 matching, 50 patients underwent TKA using standard instrumentation (group A) and 50 cases (group B) underwent TKA utilizing a modern pressure-sensing technology (OrthoSensor, VERASENSE, Dania Beach, Florida, USA) as a real-time instrument to allow an intraoperative evaluation of inter-compartmental load pressures. The first group (group A: no sensor) included 50 patients (50 knees): It had 94% males with a median age of 67.3 years (range 53–77) and a BMI of 34.7 (range 23.7–42.5); the second group (group B: sensor) included 50 patients (50 knees): It had 98% males with a median age of 67.7 years (range 48–75) and a BMI of 34 (range 22–41.5).
Operative technique
The implant used in this study was the Persona Total Knee System (Zimmer-Biomet), which is characterized by an anatomical tibial baseplate, two femoral designs (posterior-stabilized (PS) and cruciate-retaining (CR)), and five polyethylene inserts (CR, MC, PS, UC, and CPS), all of which are compatible with the same tibial baseplate.
The surgical technique adopted in this series was a mix between “gap-balancing” and “measured resection” as previously described. 23 The first surgical step consisted of making a rectangular extension gap (after proximal tibial and distal femur resections according to the mechanical axis of the knee) checked by spacer blocks accepting a slightly tighter medial compartment; at this point, attention was focused on the femur where the surgical trans-epicondylar axis was drawn and recognized as the main landmark for rotational alignment of the femoral component in order to avoid an excessive femoral external rotation that might contribute to postoperative mid-flexion instability. After all bone cuts were completed, the PCL was resected in all cases and both gaps were checked one more time using a 10-mm spacer block in extension and calibrated laminar spreaders in flexion (aiming for a rectangular flexion gap between 30 mm and 35 mm); an accessory soft tissue release was performed at this point to achieve symmetry or slightly more tightness (1–2 mm less opening during varus/valgus stress) in the medial compartment. After trial component positioning, the MC poly insert was used in the no sensor group (group A) if the surgeon felt that both gaps were well balanced.
In group B (sensor group), the OrthoSensor (VERASENSE) CR sensor was inserted instead of the conventional trial polyethylene and its use was guided following multiple recommendations given by the manufacturer and the current literature. 18 The patella was then relocated in the femoral groove to obtain close-to-real-time data. 24 At this point, the axial load on the sensor was measured at 10°, 45°, and 90° of flexion according to a standardized protocol. 19 The tibiofemoral load on both compartments was displayed and recorded on the screen that was wirelessly connected to the sensor (Figure 1). In the authors’ hands, these data were used to target the creation of a medial pivot kinematic as in the native knee, establishing an average mediolateral intra-compartment pressure difference <15 lbs in favor of the medial compartment. The knee was defined as stable when the authors achieved a medial compartment load <50 lbs, a lateral compartment load <35 lbs, and a mediolateral inter-compartmental difference within 15 lbs. 17,25 Previous studies showed that any value over 70 lbs should not be accepted because of the risk of postoperative stiffness and early polyethylene wear, suggesting further soft tissue releases or bony cuts should be performed. 26,27 The current authors, in the scenario of an inter-compartmental difference between 20 lbs and 40 lbs, always performed a soft tissue release in order to reproduce a slightly tighter medial compartment as previously described; in a scenario of an inter-compartmental difference >40 lbs, the authors preferred to increase the level of constraint in the polyethylene insert, shifting to a PS design in an attempt to address any residual instability. In both groups (group A: no sensor; group B: sensor), a careful clinical examination was performed under anesthesia with the trial component in place before cementation and wound closure performed in a standard fashion. Length of surgery was recorded in all cases.

Intraoperative images of a sensor-guided left knee TKA. (a) Persona CR (Persona; Zimmer-Biomet, Warsaw, USA and OrthoSensor, VERASENSE, FL, USA) articular surface shim and sensor card (not visible) ready to be inserted on the tibial baseplate (right), (b) shim and sensor card in place, (c) intraoperative testing during assisted ROM; (d) Persona Verasense intraoperative software application: loads on the medial and tibial compartments are recorded together with tracking of the tibiofemoral contact point during ROM; in this case a medial pivot kinematic has been reproduced, (e) postoperative AP X-ray; (f) articular surface shims modularity (10, 11, 12, 13, 14, 16 mm). ROM: range of motion; TKA: total knee arthroplasty.
Primary outcome measurements
The clinical outcome was measured using the OKS and the KSS, which were collected at the preoperative visit and at the most recent FU visit (minimum 24 months, range 24–36). 28 Preoperative radiographic evaluation was undertaken on full-length lower limb anteroposterior (AP) X-ray, a standard WB AP and lateral knee X-ray. At the 2-year FU visit, knee AP and lateral view films were performed. The senior author was involved only in performing the procedures, not in data collecting and elaboration; this section of the study was performed by a single coauthor (AC) blinded to the allocated cohort at the time of examination.
Secondary outcome measurements
Complications, defined as “any deviation from the normal intraoperative and postoperative course,” were recorded, along with time of procedure and length of stay. 29
Statistical analysis was conducted in R (R Core Team) 30 and figures were produced using the package ggplot2 31 . The authors tested the difference between the two populations using the standard Student’s t test, and a p value <0.05 was employed as a threshold for significance. The independent t test was used to assess the female:male ratio between the two populations. The data have been reported as a mean value and the standard deviation (SD) has been calculated and reported when appropriate. The load value was reported in lbs unit in accordance with the software utilized by the pressure-sensing technology system; the load value has been reported as a mean value in both compartments at 10°, 45°, and 90° of flexion; and the load differences before and after bone recuts or soft tissue releases were also recorded and statistically compared.
Results
The demographic data of the two populations and a description of the allocation of the patients are summarized in Table 1 and Figure 2. All patients (group A: no sensor; group B: sensor) were available at a minimum FU of 2 years: no differences in FU time were demonstrated between the two groups (no sensor group average FU: 26.9 months, SD 3.9; sensor group average FU: 26.6 months, SD 3.4). Preoperatively (Table 1), there were no statistical differences between the groups in the average ROM (group A: 108°; group B: 112°), average OKS (group A: 19; group B: 19.6), average KSS (group A: 64.4; group B: 65), and average BMI (group A: 34.70; group B: 34.40). At final FU, there were no statistical differences between the groups in the average OKS (group A: 41.1; group B: 41.5) and in the average KSS (group A: 165.7; group B: 166.3). We found no statistically significant difference in the final maximum active flexion: 123° in group A and 124° in group B (Table 1). Because of these findings, the authors accepted the null hypothesis and concluded that the rate of clinical improvement was similar in both cohorts, as captured by surgeon evaluation (KSS) and patient-reported outcome scores (OKS).

Flowchart of population selection. MC TKA: medially congruent total knee arthroplasty; group A: no sensor group; group B: sensor group.
Preoperative versus final FU data.a
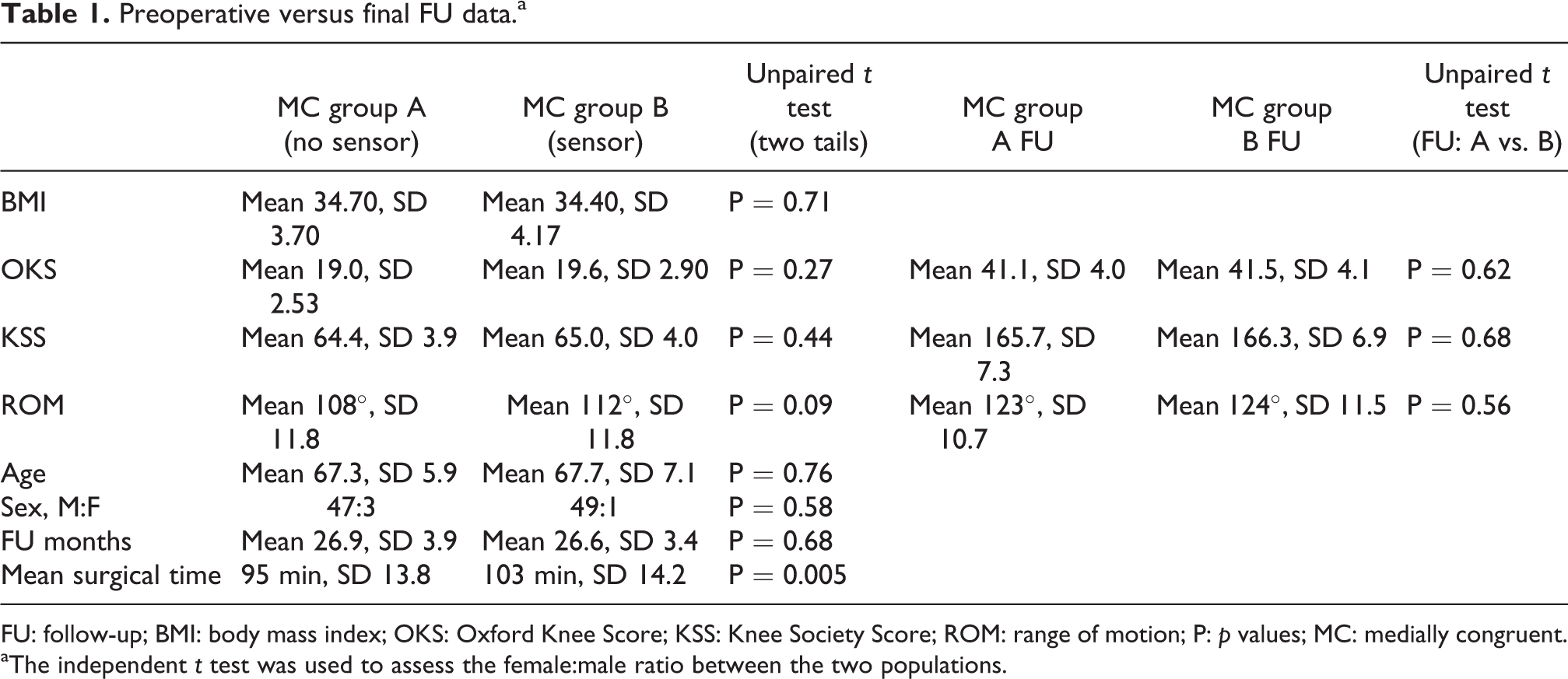
FU: follow-up; BMI: body mass index; OKS: Oxford Knee Score; KSS: Knee Society Score; ROM: range of motion; P: p values; MC: medially congruent.
aThe independent t test was used to assess the female:male ratio between the two populations.
In the sensor group, an accessory soft tissue release or bone recut was necessary after sensor testing with trial components in 12 patients (24%) in order to obtain the desired intra-articular loads (Table 2). In this group of patients, the level of constraint in the final components was increased to PS in six cases (12%) because of an inter-compartmental difference >40 lbs. Average surgical time was 8 min longer in the “sensor” group (p < 0.05).
One patient in each group required a manipulation under anesthesia because of poor ROM: one patient in the no sensor MC group (2.1%) at 11 weeks from surgery and one patient in the sensor MC group (2.1%) at 10 weeks from surgery.
Medial compartment loads
At the time of the initial trial (before soft tissue release or bone recut), the medial compartment loads were the highest when the knee was held at 90° of flexion; on the other hand, at the time of final trialing, the loads were the highest when the knee was held at 45° of flexion. Interestingly, there was a substantial reduction of medial compartment loads at relaxed extension (10° of flexion; Figures 3 and 4) both during initial and final trialing. The average load at all the degrees of knee flexion decreased after readdressing the soft tissues and bone surfaces to obtain the desired loads in the medial compartment but the difference was not statistically significant (n.s.).

Average load value in the med and lat compartments during initial trial testing (10°, 45°, and 90° of knee flexion) before soft tissue and/or bone recuts. The red dots represent the average load value. 10 lbs = 4.5 kg; 20 lbs = 9 kg; and 30 lbs = 13.6 kg. The error bars represent the SD. SD: standard deviation; med: medial; lat: lateral.

Average load value in the med and lat compartments during trial testing (10°, 45°, and 90°) after soft tissue and/or bone recuts. The red dots represent the average load value. 10 lbs = 4.5 kg; 20 lbs = 9 kg; and 30 lbs = 13.6 kg. The error bars represent the SD. SD: standard deviation; med: medial; lat: lateral.
Lateral compartment loads
The lateral compartment showed a similar bimodal loading pattern throughout ROM as seen in the medial compartment: Higher loads were seen with the knee held at mid-flexion (45°) compared to relaxed extension and flexion at 90°. There was a reduction of loads when the knee was taken from mid-flexion to relaxed extension and a similar decrease in loads when the knee was taken from mid-flexion to 90° (Figures 3 and 4). This bimodal loading pattern was similar pre- and post-readdressing the soft tissues and bone surfaces to obtain the desired loads in the lateral compartment. Similarly to the medial compartment, the average lateral compartment loads at all the degrees of knee flexion decreased after readdressing the soft tissues and bone surfaces to obtain the desired loads (Table 2).
Load differential between compartments
The loads throughout ROM remained higher in the medial compartment than the lateral compartment during the entire ROM (Figure 3 and 4); however, this finding was n.s.. On the other hand, the absolute load differential between the medial and lateral compartments increased with the degrees of knee flexion. The lowest load value during final sensor testing was found on the lateral compartment with the knee at 90° (18.6 lbs, min. 0–max. 69), demonstrating that the lateral femoral condyle was able to reproduce the posterolateral rollback during knee flexion and simultaneous internal rotation of the tibia, a pattern typical of the natural knee (Figure 4). The subpopulation of patients who underwent soft tissue releases or bone recuts (12 patients in group B) was thoroughly analyzed: In this subgroup, the adjunctive surgical gesture appeared to influence the load more during testing at relaxed extension (10°) and at 90° of flexion than during mid-flexion (45°) (Table 2 and Figure 5).
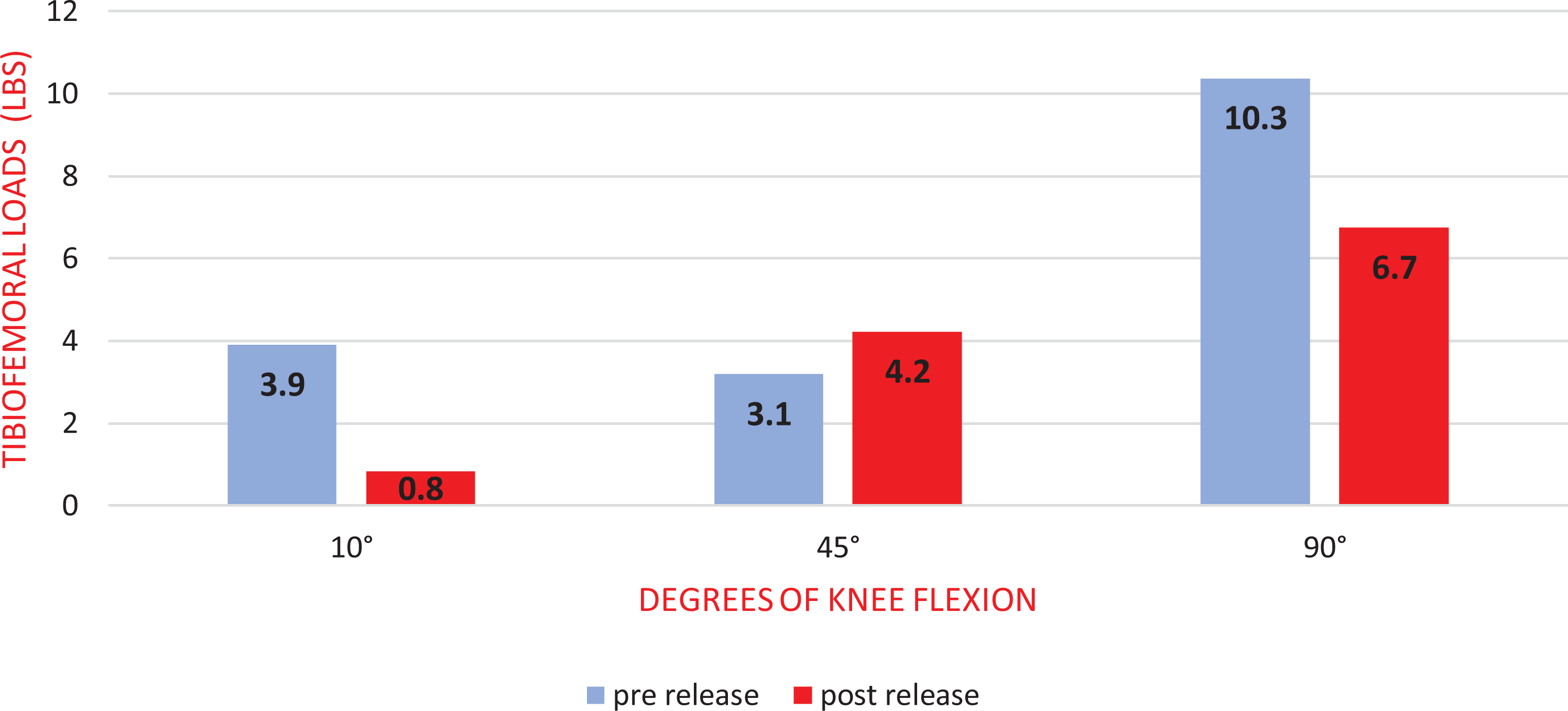
Load variation (average) before and after soft tissue release or bone recuts in the subpopulation of patients (group B: 12 patients) who underwent adjunctive surgical steps to obtain the desired intra-articular loads. The final load was influenced more at relaxed extension (10°) and at 90° than during mid-flexion (45°) (n.s.). 4 lbs = 1.8 kg; 6 lbs = 2.7 kg; and 10 lbs = 4.5 kg. n.s.: not statistically significant.
Load differences before and after soft tissue release/bone recuts in 23 of 50 patients in the sensor group (MC group B).a

SD: standard deviation; Med: medial; Lat: lateral.
a10 lbs = 4.5 kg; 20 lbs = 9 kg; 30 lbs = 13.6 kg; 35 lbs = 15.8 kg.
Discussion
This study showed that the use of an intraoperative sensing technology during primary, medial pivot TKA was not related to a statistically significant improvement in the clinical outcome at 2-year FU. Nevertheless, the most relevant finding was that use of the sensor required a high number of accessory surgical gestures (soft tissue releases or bone recuts) in order to reproduce the medial pivot kinematics during primary TKA. In fact, in 24% of the patients, the sensor detected the need to modify balancing, and in 12% of patients, led to an increase in the level of constraint because it detected mild instability. The potential benefits of those intraoperative steps have not been proved by the authors.
As the demand for TKA is constantly increasing, the industry is responding with multiple technological advancements. 16,32,33 The goal of the use of these new technologies is not only to improve implant alignment but also to guarantee an accurate knee balancing. As previous studies have proven, a proper TKA balancing is fundamental for the success and longevity of the implants 15,34,35 but there is no actual standardization of this procedure and balancing the knee remains an art with no definitive protocol on how to optimize tissue tension in TKA. Intraoperative sensing technology (OrthoSensor, VERASENSE) gives a more quantitative, and therefore a more standardized, method of detection of global soft tissue balancing and proper component alignment. It gives a dynamic, real-time feedback regarding tibiofemoral position and quantitative pressure at peak contact points in the medial and lateral compartments during both TKA trials and final implant positioning. 18 Furthermore, the possibility of intraoperative knee testing during assisted ROM, with trials or final implants in place, represents a great tool to avoid future mid-flexion instability in comparison with standard techniques, which utilize classical spacer blocks or laminar spreaders only in full extension or locked flexion. 17,36 MacDessi et al. showed, on 322 mechanically aligned TKA, that the expert surgeon, in comparison with the sensor, could accurately determine knee balance in 63% of cases at 10° of flexion, 57.5% at 45°, and 63.7% at 90°, concluding that standard assessment of knee balance is a poor predictor of the true soft tissue balance when compared to sensor data. 37 Cho et al., in a recent study, showed that only 35.7% of TKA that experienced surgeons considered well balanced using standard techniques achieved good stability when tested with the sensor, pointing out the poor reliability of an operator-dependent hands-only feeling. 38 Meere et al. conducted a cadaveric study showing that the use of a pressure sensor guided the surgeon to balance the TKA with greater medial compartment forces and greater lateral laxity in comparison with normal tools; these patterns better reproduced the normal kinematic of the knee. 39 To date, there is no clear consensus in the literature regarding whether a classic, truly balanced knee has better results in terms of durability and stability when compared to a TKA with a subtle lateral laxity and a more thigh medial compartment that mimics a more physiologic kinematic. A few recent reports highlighted that better reproduction of the normal anatomy of the knee, with mild to moderate mediolateral laxity during a varus stress test, is linked to a better clinical score. 40 Edwards et al. 41 and Liebs et al. 42 reported better WOMAC (Western Ontario and McMaster Universities Osteoarthritis Index) pain scores in a group of patients showing a larger lateral than medial gap during knee stability testing. Based on those findings, Risitano et al. proposed a modified surgical technique using a wireless load-sensor that may allow reproduction of physiologic knee kinematic providing objective and reproducible data. 19
The current study showed that the intraoperative use of load sensors improved the use of a medial pivot implant (characterized by a lower level of constraint when compared to PS), intraoperatively reproducing a normal kinematic without increasing the risk of postoperative patient-detected instability. The current results differ from those of previous studies. Schnaser et al., 43 in a retrieval study on PS TKA designs, demonstrated that loads throughout ROM shifted from the medial to the lateral compartment regardless of the patella position, whereas the current authors reported opposite findings. Our findings could be due to the use of a different surgical technique (aimed on obtaining a slightly tighter medial compartment during gap-balancing) and a polyethylene insert having a fully congruent (1/1 radius) medial compartment. Meneghini et al. 25 also demonstrated that knees showing a dual pivoting kinematic with a late medial pivoting performed clinically better when compared to different kinematic patterns.
The current authors also demonstrated that, in contrast to other technologies, 11 the use of this sensor testing did not require a change in the surgical workflow, as also shown by Lakra et al. 44 and that the average operative time was prolonged only by 8 minutes. The current authors recognize that, as with many new novel technologies, the use of the sensor in the hands of a surgeon unfamiliar with the system may increase operative time: This can lead to a longer duration of anesthesia and potentially increased operative costs and complications. Laktra et al. 44 also demonstrated that it takes approximately 41 cases of sensor-assisted TKA cases to achieve an operative time similar to manually balanced TKA cases.
This study has several major limitations. The sample size was relatively small. The authors intended to review their early experience using this sensor technology after developing a novel surgical technique dedicated to medial pivot TKA. 19 In addition, all patients underwent primary TKA because of primary OA with mild deformities; given this and the small size of our cohorts, we were not be able perform sub-analyses. Another major limitation of this study is represented by the fact that the load registration was not made in a weight-bearing scenario, different from the normal gait circumstances; however, Wasielewski et al. 45 showed that this passive intraoperative load registration correlates with postoperative knee kinematics. Most importantly, our results do not demonstrate that the use of this computer-assisted technology correlates to superior clinical outcomes compared to manual gap-balancing techniques; we only demonstrated that the intraoperative feedback given by the sensor helped to reproduce a medial pivoting kinematic, which, in the authors’ hands, reflects the one of the native knee.
Conclusion
Despite the improvement in TKA implant design and advances in technology, proper balancing in TKA is still a challenging step. The wireless load-sensing tibial device object of the current study was introduced to help adult reconstruction surgeons in this effort. Even though the use of this technology was not related to an improvement in the clinical outcome, this study showed that it facilitates the reproduction of a natural stability in the joint lowering the level of constraint in the replaced knee. A greater number of patients and long-term FUs are warranted in order to validate the findings of the current study.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.