
Abstract
Background
Patient satisfaction and expectations are now recognized as an outcome measure for successful total knee arthroplasty (TKA). The purpose of this study was to determine which factors including soft tissue balance during surgery affect patient satisfaction and expectations after TKA.
Methods
A total of 135 patients (157 knees) with knee osteoarthritis who underwent primary TKA with a posterior stabilized design were studied. After implantation of all components, varus/valgus laxity of the knee was measured intraoperatively with the knee at 0°, 30°, 60°, 90°, and 120° guided by an image-free navigation system. Factors that affected patient satisfaction and expectations, including lateral and medial laxities, were evaluated using the 2011 Knee Society score.
Results
The mean intraoperative lateral laxity was 1.1°, 1.6°, 0.9°, 1.3°, and 1.7° with the knee at 0°, 30°, 60°, 90°, and 120°, respectively. The mean intraoperative medial laxity was 1.1°, 1.4°, 1.1°, 1.1°, and 1.7° with the knee at 0°, 30°, 60°, 90°, and 120°, respectively. Patient satisfaction after TKA correlated positively with symptom (R = 0.61, p < 0.01) and functional activity (R = 0.47, p < 0.01) scores. Patient expectations after TKA weakly positively correlated with symptom (R = 0.29, p < 0.01) and functional activity (R = 0.20, p = 0.01) scores, and weakly negatively with medial laxity at 30° (R = −0.21, p < 0.01).
Conclusion
Midflexion medial laxity was associated with worse patient expectations after TKA. Avoiding medial laxity could be one of the important techniques during TKA.
Keywords
Introduction
Total knee arthroplasty (TKA) reduces pain, restores function, and enhances quality of life for patients with symptomatic osteoarthritis. 1 In addition, TKA is a clinically proven and cost-effective procedure. 2 However, a significant number of patients are not satisfied with the results of TKA. Patient satisfaction and expectations are now recognized as an outcome measure for successful TKA.3–6
TKA is the most commonly performed orthopedic procedure, yet the existing evidence for patient satisfaction and expectations following TKA has not been analyzed in detail. 7 There is a well-known difference between patient satisfaction based on the patients’ subjective report and clinical outcome as determined by the surgeon. 8 Many factors could affect patients’ expectations, satisfaction, and function after TKA.
Normal gap laxities have been reported using various methods. The gaps are the tibio-femoral space occurring secondary to distraction by the attached soft-tissue sleeve. The flexion and extension gaps are defined as the spaces in flexion and extension, respectively. The lateral and medial flexion gaps are measured as the distance from the distal femur to the proximal tibia in flexion at lateral side and medial side, respectively (Figure 1). Soft-tissue balance is obtained by releasing soft tissue including ligament, tendon, and capsule.
9
The flexion gap has been reported to be wider than the extension gap,10–12 and the lateral flexion gap tends to be greater than the medial flexion gap in normal knees (Figure 1).5,7,11–15 While performing varus or valgus stress, 2 mm opening of each compartment is permitted. The influence of intraoperative soft-tissue balance on knee kinematics remains unknown. Screen shots of navigation showing (a) lateral flexion gap of 16 mm and medial flexion gap of 6 mm, and (b) lateral extension gap of 9 mm and medial extension gap of 6 mm.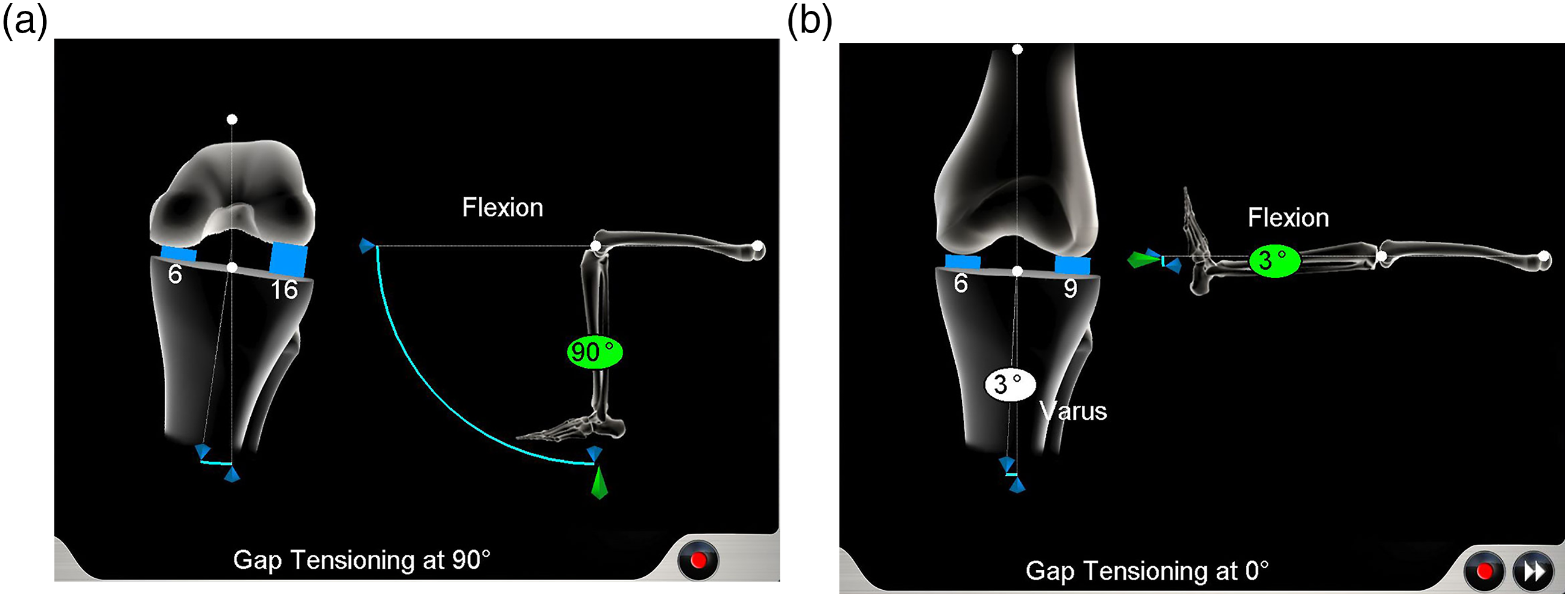
The purpose of this study was to determine which factors, including soft-tissue balance, contribute to patient expectations and satisfaction after TKA.
We hypothesized that intraoperative soft-tissue balance could contribute to patient expectations and satisfaction after TKA.
Methods
The inclusion criteria included knees underwent consecutive primary TKA with substantial pain and loss of function due to knee osteoarthritis between May 2014
The image-free navigation system (Orthopilot 4.2. B. Braun; Aesculap, Tuttlingen, Germany) was used to ensure the accuracy of implantations and measure the flexion angle of the knee during the joint component gap measurement using a tensor. The study included 17 men (21 knees) and 118 women (136 knees), with a mean age of 73 years (range, 48–88 years) and a mean body mass index of 26.1 kg/m2 (range, 17.2–44.1 kg/m2). The diagnosis was osteoarthritis in all patients. The mean preoperative flexion and extension angles were 117.2° ± 17.2° and −11.6° ± 9.0°, respectively. Full-length standing anteroposterior radiograph of the knee was carried out, and the mean preoperative hip-knee-ankle (HKA) angle with the standing condition was 9.9° ± 7.2° varus.
A balanced gap technique was used. The tibial cut was first performed perpendicular to the tibial axis in the coronal and sagittal planes using navigation. The posterior cruciate ligament was sacrificed. After the tibial osteotomy, osteophyte removal and release of the deep medial collateral ligament (MCL) were performed in varus knee. Superficial MCL was not released to obtain slight medial tightness in most cases. Rotation of the femoral component was determined according to the navigation system after soft tissue balancing; however, the surgeon checked to ensure that they were near parallel to the surgical epicondylar axis. The amounts of bony cut and varus/valgus alignment on the screen of the navigation system were determined based on the measurement of the extension and flexion gaps using the offset-type tensor. Posterior osteophytes in the femur were removed to avoid limitations associated with deep flexion. Following bony resections and soft tissue releases, a posterior stabilized (PS) design was used for all cases (Vega, Aesculap), and all components were fixed with cement. All patellae were resurfaced. After implantation of all components, the arthrotomy was temporarily repaired by applying stitches, and varus/valgus laxity of the knee was measured intraoperatively with the knee at 0°, 30°, 60°, 90°, and 120° guided by a navigation system. Intraoperative measurements were taken manually in the position of no stress, varus stress, and valgus stress up to palpable endpoints by one surgeon. Intraoperative medio-lateral laxity was defined as the difference between varus stress and valgus stress. Various changes in medio-lateral laxity were calculated, including from 0° to 30°, 30°–60°, 60°–90°, and 90°–120°. Anatomic alignment was measured on the full leg-length standing radiograph postoperatively, and flexion and extension of the knee were measured at the time of last follow-up.
All patients were evaluated using the new Knee Society Knee Scoring System (KSS 2011) after a mean follow-up of 3 years (range, 2 years–4 years). The KSS 2011 has five components, including patient demographics, objective knee score, patient expectations, patient satisfaction score, and functional knee score. Patient expectations, patient satisfaction score, and functional knee score were completed by the patient. Higher scores were associated with better outcomes. 16 Patient expectations were compared to what patients expected before his or her knee replacement. 16
Statistical analysis
Factors that affected patient satisfaction and expectations were evaluated. Correlation analyses were performed using Spearman’s rank correlation test. Dependent variables included symptom score, functional activities score, age, body mass index, preoperative and postoperative HKA, postoperative flexion and extension, lateral laxity, medial laxity, medio-lateral laxity including midflexion laxity, which was defined as medio-lateral laxity at 30° and 60°, and changes in medio-lateral laxity from 0° to 30°, 30°–60°, 60°–90°, and 90°–120°. The laxity differences between right and left knees were examined in 22 patients who underwent bilateral TKA. Correlation between laxity and patient satisfaction as well as expectations were evaluated. The Mann-Whitney U test was used for categorical data, including sex. The Wilcoxon signed-rank test was used to compare preoperative and postoperative flexion and extension. Lateral laxity, medial laxity, and medio-lateral laxity at various angles were compared using Friedman test with Bonferroni adjustment. Values are reported as means or correlation coefficients. p < 0.05 was considered significant. Data were statistically analyzed using IBM SPSS Statistics 24 (SPSS Inc, Chicago, IL, USA) and R version 3.5.1 (R Foundation for Statistical Computing, Vienna, Austria; http://www.R-project.org/).
Results
Intraoperative laxity
The mean intraoperative lateral laxity was 1.5 ± 1.1° with the knee at 0°, 1.7 ± 1.6° with the knee at 30°, 0.8 ± 0.9° with the knee at 60°, 1.2 ± 1.3° with the knee at 90°, and 1.7 ± 1.7° with the knee at 120°. The laxity decreased significantly from 30° to 60° (p < 0.01) and increased significantly from 60° to 90° (p < 0.01) and from 90° to 120° (p < 0.01, Figure 2(a)). The mean intraoperative medial laxity was 1.1 ± 0.9° with the knee at 0°, 1.4 ± 1.4° with the knee at 30°, 1.1 ± 1.4° with the knee at 60°, 1.1 ± 1.7° with the knee at 90°, and 1.7 ± 1.9° with the knee at 120°. The laxity significantly increased from 90° to 120° (p < 0.01), but significantly decreased from 30° to 60° (p = 0.04, Figure 2(b)). The mean intraoperative medio-lateral laxities with the knee at 0°, 30°, 60°, 90°, and 120° were 2.5 ± 1.3°, 3.1 ± 1.8°, 1.9 ± 1.5°, 2.3 ± 1.9°, and 3.4 ± 2.6°, respectively. The medio-lateral laxity significantly increased from 0° to 30° (p < 0.01), from 60° to 90° (p = 0.01), and from 90° to 120° (p < 0.01) but significantly decreased from 30° to 60° (p < 0.01, Figure 2(c)). The mean intraoperative lateral laxity difference between right and left knees in bilateral TKA was 0.6 ± 1.4°, 0.4 ± 2.0°, 0.4 ± 1.2°, 0.1 ± 1.8°, and 0.3 ± 2.3° with the knee at 0°, 30°, 60°, 90°, and 120°, respectively. The mean intraoperative medial laxity difference between right and left knees was 0.0 ± 1.6°, 0.3 ± 1.1°, 0.5 ± 1.4°, 0.5 ± 1.7°, and 0.6 ± 2.3° with the knee at 0°, 30°, 60°, 90°, and 120°, respectively. Intraoperative laxity at 0°, 30°, 60°, 90°, and 120°. (a) Lateral laxity, (b) Medial laxity, (c) Medio-lateral laxity. All results are expressed as means ± standard deviation. *p < 0.01, **p = 0.04, ***p = 0.01.
KSS 2011
The mean anatomical alignment was 6° valgus, and all knees had 25 points for neutral alignment (2–10° valgus). The mean postoperative HKA angle with the standing condition was 0.2° ± 1.5° valgus. The mean postoperative flexion and extension angles were 124.1 ± 19.7° and −1.1 ± 4.7°, respectively. Flexion and extension angles were significantly improved postoperatively (p < 0.01); these postoperative values showed significant positive correlations with the corresponding preoperative values (flexion: R = 0.61, p < 0.01, extension: R = 0.36, p < 0.01).
After TKA, the mean overall score for the KSS 2011 was 121 of 180 points, the mean symptoms score was 21 of 25, the mean satisfaction score was 26 of 40, the mean expectation score was 10 of 15, and the mean functional activities score was 64 of 100.
Factors that affected patient satisfaction and expectations
Patient satisfaction after TKA correlated positively with symptom (R = 0.61, p < 0.01) and functional activity (R = 0.47, p < 0.01) scores. Patient expectations after TKA Correlations between patient expectations after TKA and (a) symptoms, (b) functional activities, and (c) medial laxity at 30°.
Discussion
The important finding of this study was that the expectations after TKA evaluated using KSS 2011 correlated positively with symptoms and functional activities and negatively with medial laxity at 30°. Satisfaction after TKA correlated positively with symptoms and functional activities.
Patient satisfaction and expectations are important outcome measurements after TKA. Patient satisfaction and expectations were reported to be negatively correlated with varus postoperative alignment. 17 In the present study, no knees showed malalignment using navigation. Functional activities were reported to correlate significantly with patient satisfaction and expectations, similar to the present results. 18 Previous study showed that knees with postoperative medial joint laxity >3° in flexion resulted in inferior KSS 2011 scores, and lateral joint laxity did not affect patient satisfaction or knee function after TKA. 19 Medial stability of the knee is considered to be associated with good clinical results after TKA. 20 When measured medial-lateral component gaps at 0° knee extension and 90° flexion, excessive intraoperative medial joint laxity ≥4 mm at 90° flexion was associated with decreased patient satisfaction at 1 year 21 In that study, 21 the median KSS 2011 at 1 year postoperatively was significantly lower in medially loose knees than in medially tight knees, and medial flexion laxity resulted in lower patient satisfaction. However, that study did not evaluate midflexion laxity. Our study included this important endpoint. Assessment of gaps at midflexion is ambiguous. One study showed that 36% of TKA cases had laxity at midflexion even when a rectangular extension (0°)-flexion (90°) gap was achieved. 22 Medial laxity at 30° correlated negatively with patient expectations in the present study. In the patients with bilateral TKA, medial laxity at 90° was associated with patient dissatisfaction, and medial laxity at 30° and 60° was associated with worse expectations. Although we found no correlation between medial laxity at 30° and patient satisfaction, recent study demonstrated that medial laxity at 30° negatively correlated with patient satisfaction in bi-cruciate stabilized TKA. 23 The intraoperative predictor of patients’ satisfaction after bi-cruciate stabilized TKA was medial joint stability at 90°. 24 A modified gap balance technique was used in an attempt to achieve the same gap at 0° and 90°, but midflexion laxity could not be adjusted during surgery. In a previous study, joint gap kinematics were measured using a tensor device, and the center size of the joint gap was tight in extension and deep flexion and loose at midflexion ranges, especially at 30° of flexion. 25 In the present study, intraoperative medio-lateral laxity increased from 0° to 30°, and looseness at 30° was confirmed. The Vega femoral component has a multi-radius design, and this design has been shown to influence midflexion laxity compared with a single-radius design.26–28 Comparing single-radius and multi-radius designs, less constraint was shown in multi-radius design in the varus/valgus direction at midflexion range. 26 The tension of the collateral ligaments of the knees with multi-radius design could have been reduced. In addition, midflexion laxity has been greater after PS TKA than with cruciate-retaining procedures. 29 The design of Vega could contribute to midflexion laxity in the present study. During most activities of daily living the knee is loaded not only in full extension but also in midflexion, 30 and midflexion laxity should be considered an important outcome measure. 29
The present study clearly showed that midflexion laxity could greatly vary. Although a mean medial laxity at 30° was 1.4°, maximum medial laxity at 30° was 8°. Because some patients had excessive medial laxity at 30°, patient expectations might correlate negatively with medial laxity at 30°. Surgeons could not feel intraoperative laxity less than 2°. The error margins for the navigation system were 1°. Intraoperative laxity can be evaluated using navigation, radiographs, and tensor. However, radiographs during surgery for evaluating laxity were not indicated because of excessive radiation exposure. Patient satisfaction is a multi-factorial result for TKA, and a mean of 1.4° of medial laxity might barely cause a dissatisfaction.
This study has some limitations. First, a small number of patients was studied. Second, follow-up periods were short. Third, soft tissue balance was measured manually. The applied stress needs to be controlled and reproducible, though measurements were taken manually up to palpable endpoints by one surgeon. Fourth, there were possible bias issues because of one surgeon’s experience. Fifth, midflexion instability in anteroposterior direction could not evaluated using navigation. Sixth, after soft tissue healing, the laxity would not be the same as during surgery. We evaluated laxity including midflexion laxity using navigation. And we could not evaluate the laxity of patients at time of last follow-up using the same methods. When varus/valgus laxity was measured with the knee in extension at 6 months, 1 and 2 years after surgery, and at final follow-up examination (average, 77 months), coronal laxity did not change over time.
31
Intraoperative joint gap laxity was associated with mediolateral laxity after TKA, especially at midflexion angles.
32
Seventh, patient expectations after TKA correlated negatively with medial laxity at 30°
Conclusions
Symptoms and functional activities were correlated with patient expectations and satisfaction after TKA. Midflexion medial laxity was associated with worse expectations, which means our hypothesis was partly confirmed. Intraoperative soft-tissue balance did not contribute to patient satisfaction. Avoiding medial laxity could be one of the important techniques during TKA.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.