
Abstract
Objective:
The purpose of this radiological study was to assess the posterior laxity of a single model of a total knee arthroplasty design (TKA) having a medially constrained (MC) or a Posterior-Stabilized (PS) polyethylene insert using a well-documented stress x-ray. To the authors knowledge, this is the first report evaluating MC TKA outcomes according to the “kneeling view.”
Materials and Methods:
Sixty patients with non-traumatic primary knee osteoarthritis undergoing TKA were first matched by age, sex, BMI and diagnosis and then divided in two groups: group A (37 knees) received a MC TKA and group B (23 knees) a PS implant made by the same manufacturer. In all cases the posterior cruciate ligament (PCL) was resected. All patients underwent the same postoperative “kneeling view” and were also clinically evaluated according to the Knee Society Score (KSS) and Oxford Knee Score (OKS). Radiographic measurements were taken by tracing a line along the posterior cortex of the tibia and then measuring the perpendicular distance to a point marked at the posterior corner of Blumensaat’s line.
Results:
At 12 months minimum FU, no statistically significant differences were found between the two groups in all the clinical scores. There was a statistically significant difference on kneeling view values between the two groups (P = 0.0002): the mean value in the MC group was −1.97 ± 3.8 mm while was −5.6 ± 3.1 mm in the PS group. In both groups, the average position of the posterior cortex of the tibia was anterior to the posterior corner of Blumensaat’s line, showing absence of instability in flexion.
Conclusion:
This study highlighted that the PCL removal, accompanied by a precise surgical technique, did not increase the instability in flexion in two groups of patients having the same TKA design but polyethylene inserts characterized by different levels of constraint.
Introduction
Despite being a very successful surgical procedure, total knee arthroplasty (TKA) is prone to major complications which may limit its survivorship. TKA instability has been highlighted as a major cause of failure, 1 especially in the chronic setting.
In the early setting, TKA instability is usually due to mismatch between the flexion and the extension gap, suboptimal coronal and rotational component alignment, and iatrogenic loss of ligamentous integrity. In the late setting, TKA instability is usually due to aseptic loosening of the components with concomitant moderate to severe bone loss. Mid-flexion instability due to flexion/extension gap mismatch, represents a well described phenomenon since the early 1990s 2 and a major cause for patient dissatisfaction 3 and implant revision. 4,5
Pure flexion instability occurs when the flexion gap is significantly larger than the extension gap: this is usually due to a technical error at the time of the original surgery or to the progressive attenuation of the PCL in the setting of a cruciate retaining implant.
Being a symptom more than a clinical finding, instability after TKA is difficult to quantify. In the normal knee, an antero-posterior (AP) laxity between 5 and 10 mm during the posterior drawer test at 90 degrees of flexion has been considered as acceptable. 6,7 Recently, a posterior translation of the tibia more than 7 mm, during KT-1000 evaluation, has been considered as pathologic in two consecutive published series of TKA. 8,9 Unfortunately, the classical clinical evaluation of posterior knee laxity after TKA is not a reliable and reproducible measurement due to inter-operator variability, intra-operator variability and patient compliance. 10 The identification of the optimal, residual laxity in the sagittal plane, which does not compromise the postoperative ROM, remains to be clarified and is one of the research topics currently most investigated in adult reconstruction. Several radiological views have been proposed to test the stability of the knee after single or multiple knee ligament injuries 11 –13 with a minor number of studies focusing on the subjects who underwent TKA. 14
The loading “kneeling view” has been already validated in previous clinical studies as an accurate diagnostic tool for the evaluation of the posterior stability of the knee: the posterior displacement forces produced during that test reproduced values comparable to the ones produced by the Telos stress device. 15 –17
The purpose of this study was to evaluate two groups of patients who underwent primary TKA, using the same knee system but two different polyethylene designs (“medial-congruent” or MC and “posterior stabilized” or PS) according to the weight bearing “kneeling view.”
The null hypothesis was that the main difference between the two groups would be given by the fact that, in PS knees, the tibia slightly translated anteriorly respect to the femur during kneeling because of the cam/post interaction while the opposite phenomenon (posterior tibial translation) was happening when MC implants were tested at 90 degrees of knee flexion under direct load application.
Materials and Methods
This study evaluated a cohort of patients prospectively included and retrospectively evaluated. Sixty patients who underwent primary TKA were included in two groups matched by age, sex (all males), BMI and preoperative diagnosis. All patients underwent primary TKA because of primary tricompartmental knee OA leading to neutral alignment or deformity less than 20° on the mechanical axis. Exclusion criteria included: preoperative diagnosis of inflammatory osteoarthritis of the knee, presence of severe bony defects or joint deformity which might require augmentation with bone graft or a constrained polyethylene insert, previous patellectomy, body mass index greater than 45, symptomatic hip pathology, previous lower extremity fractures, previous femoral or tibial osteotomy, previous knee ligament reconstruction, and neurogenic causes of knee arthritis. Patients experiencing moderate to severe pain during the kneeling test were excluded from the study. An age below 45 and over 85 years old was an additional exclusion criteria.
Twenty-three patients (Group A) received a Persona Posterior-Stabilized (PS) TKA while 37 (Group B) had a Persona Medially Congruent (MC) design (Zimmer Biomet, USA). All surgeries were performed by the senior author (PFI). Group A included 23 men with an average age of 70.9 years (range 55 to 86) and an average BMI of 30.7 (range 20.4 to 42.7). Group B included 37 men with an average age of 67.8 years (range 54 to 82) and an average BMI of 30.8 (range, 22.5 to 44.0).
The surgical technique performed by the same surgeon (PFI) was identical for both TKA designs: in all knees, the surgeon aimed to reproduce the proper mechanical axis, aligning the implants on the coronal plane and resecting both cruciate ligaments. The surgical technique, the multimodal pain control protocol and the postoperative care were previously described by the senior author. 18
All patients who reached 90 degrees of active flexion were assessed at 12 months follow-up according to Clinical and Radiological Knee Society Score (KSS) as an overall validated measurement instrument: 19 –21 all patients were questioned regarding any subjective sensation of TKA instability. Radiological evaluation of the posterior instability in all patients was performed according to the weighbearing “kneeling view” as described by Bartlett and Osti. 22
“Kneeling view” technique
A specific kneeling support has been built according to a model previously described, in order to allow a perpendicular weighbearing load with the knee flexed at 90°: the tibia was loaded directly on the tibial tubercle leaving the patella and the distal femur was not in contact with the support (Figure 1). Proper positioning of the tibia on the kneeling device and absence of any malrotation was rigorously applied in every case. Before the execution of the radiograph, each patient was asked to gradually load the knee on the support. 23

Set up for assessment of posterior drawer on 90° flexion stress X-ray (“kneeling view”).
The lateral radiograph was taken from lateral to medial, with the cassette located in a designed slot on the kneeling jug, the distance from tube to cassette was the standard 1.15 m.
All digital images obtained were measured by one of the authors (LS) according to Louisia et al. 16 using the DICOM visualization program in use at the authors’ institute [IntelliSpace Radiology, Philips, Andover, MA]. Two bony landmarks have been selected: the posterior cortex of the tibial diaphysis and the most posterior point of the Blumensaat line at 90 degrees of knee flexion; these two bone landmarks are minimally influenced by the rotations, are constant in all the knees, are not subject to bone resection during a primary TKA and are not covered by the implants. 16,24,25 Measurements on the radiographs are taken by tracing a line along the posterior cortex of the tibia and then measuring the perpendicular distance to the most posterior point of the Blumensaat line (Figure 2). If the point on the Blumensaat line is anterior to the straight line originating from the posterior cortex of the tibia the measurement assumes a positive value; on the contrary, if located posteriorly, it assumes a negative value: the distance was expressed in millimeters.
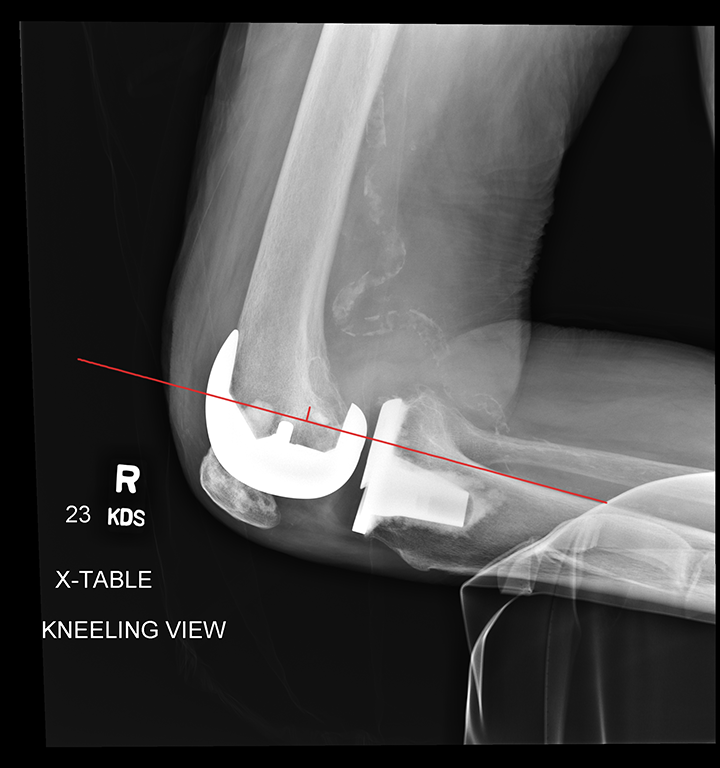
Right knee. “kneeling view” radiograph showing the measurement of the posterior draw. The measurement was taken by tracing a line along the posterior cortex of the tibia and then measuring the perpendicular distance to the most posterior point of the Blumensaat line.
Statistical analysis
All anonymized data were recorded in a secured Excel file (Microsoft Corp, Redmond, WA, USA). Statistical analysis was performed using SPSS, version 24 (IBM Corp, Armonk, NY) and differences within and between two groups were evaluated using the Student’s t test. The difference was considered significantly when P < 0.05. Spearman’s rank correlation coefficient was used to identify the relationship between kneeling values and other parameters.
Results
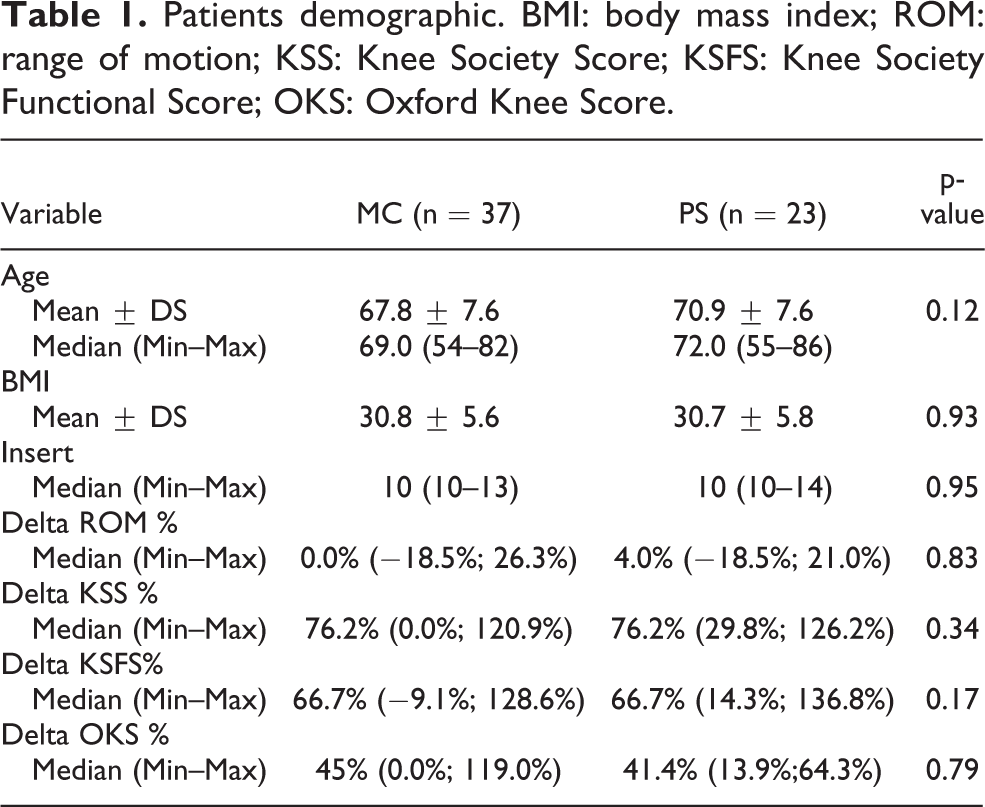
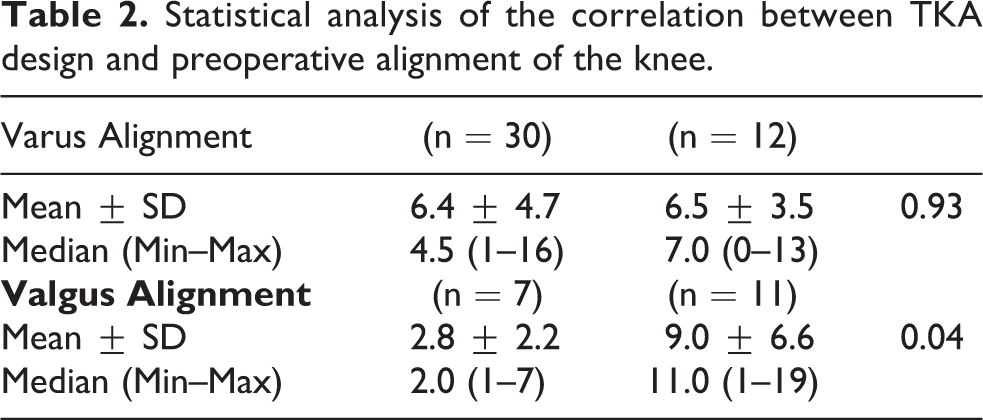
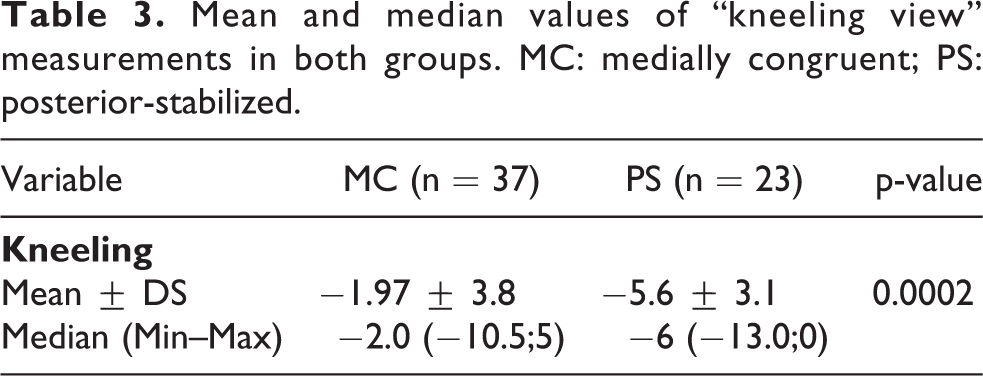
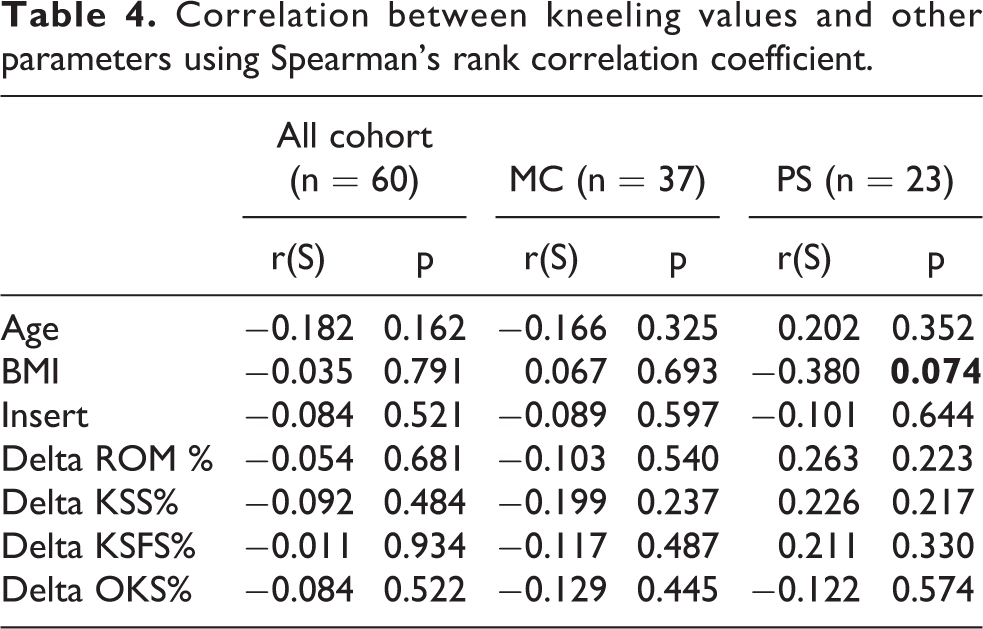
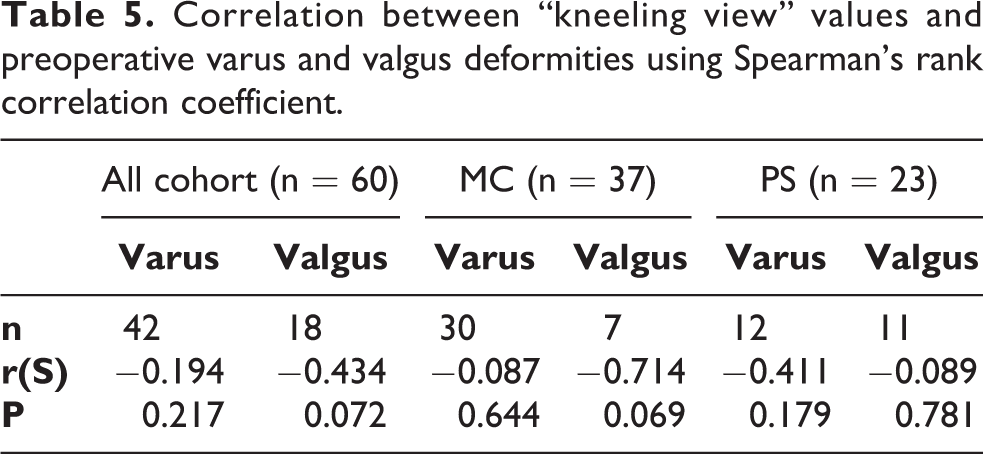
There were no significant differences in age (P = 0.12), BMI (P = 0.93), or polyethylene insert size (P = 0.95) between the two groups (Table 1). Regarding the preoperative alignment of the knee, there was a statistical difference (p = 0.04) between the two groups in their anatomical alignment: the mean value for MC group was 2.8° varus and the mean value for PS group was 9.0° varus (Table 2); there were seven patients with a preoperative valgus deformity in the MC group and 11 in PS group. Calculating the percentage variation of the parameter between post- and pre-surgical intervention compared to the pre intervention value (δParameter%), the postoperative clinical outcome for the complete cohort showed an improvement on all scores (KSS, KSFS and OKS) from preoperative values, with only the exception of median value of δROM% in MC group, which registered a variation of 0%; nevertheless, no statistically significant differences were found between study groups. The mean value of kneeling view in MC group was −1.97 ± 3.8 and in PS group was −5.6 ± 3.1: there was a statistically significant difference on kneeling view values between the two groups (P = 0.0002) (Table 3) (Figure 3). Analyzing the correlation between kneeling view value and other parameters (Table 4 and 5), there was a negative correlation between BMI values and kneeling values in PS group (Figure 4), and a negative correlation between valgus values and kneeling values in MC group (Figure 5); nevertheless, both correlations did not reach a statistically significant difference (P = 0.07 and P = 0.07). No complications were observed.
Patients demographic. BMI: body mass index; ROM: range of motion; KSS: Knee Society Score; KSFS: Knee Society Functional Score; OKS: Oxford Knee Score.
Statistical analysis of the correlation between TKA design and preoperative alignment of the knee.
Mean and median values of “kneeling view” measurements in both groups. MC: medially congruent; PS: posterior-stabilized.
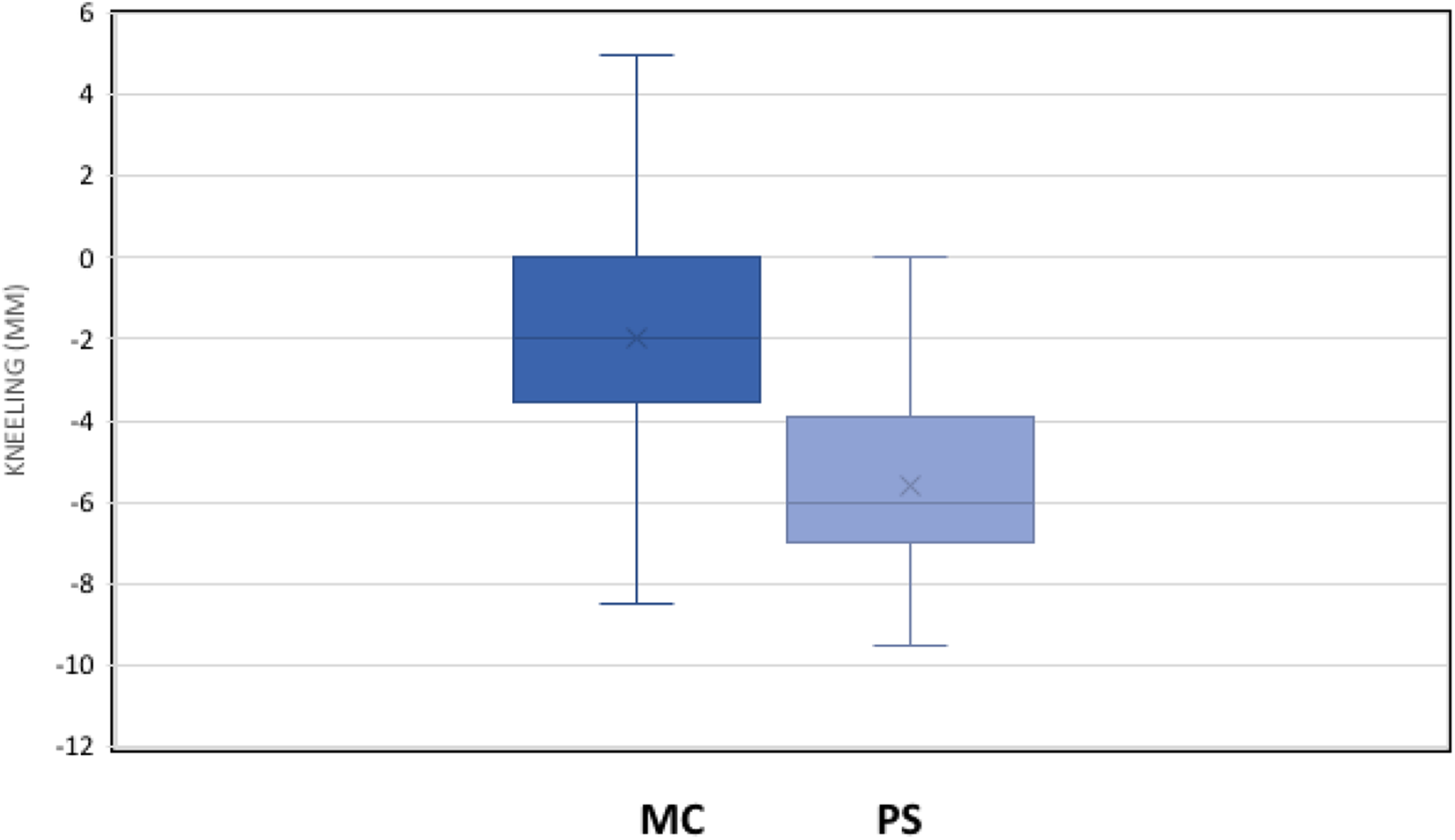
Comparative and statistical analysis of the mean value of the “kneeling view” between the two groups (P = 0.0002). MC: medially congruent; PS: posterior-stabilized.
Correlation between kneeling values and other parameters using Spearman’s rank correlation coefficient.
Correlation between “kneeling view” values and preoperative varus and valgus deformities using Spearman’s rank correlation coefficient.
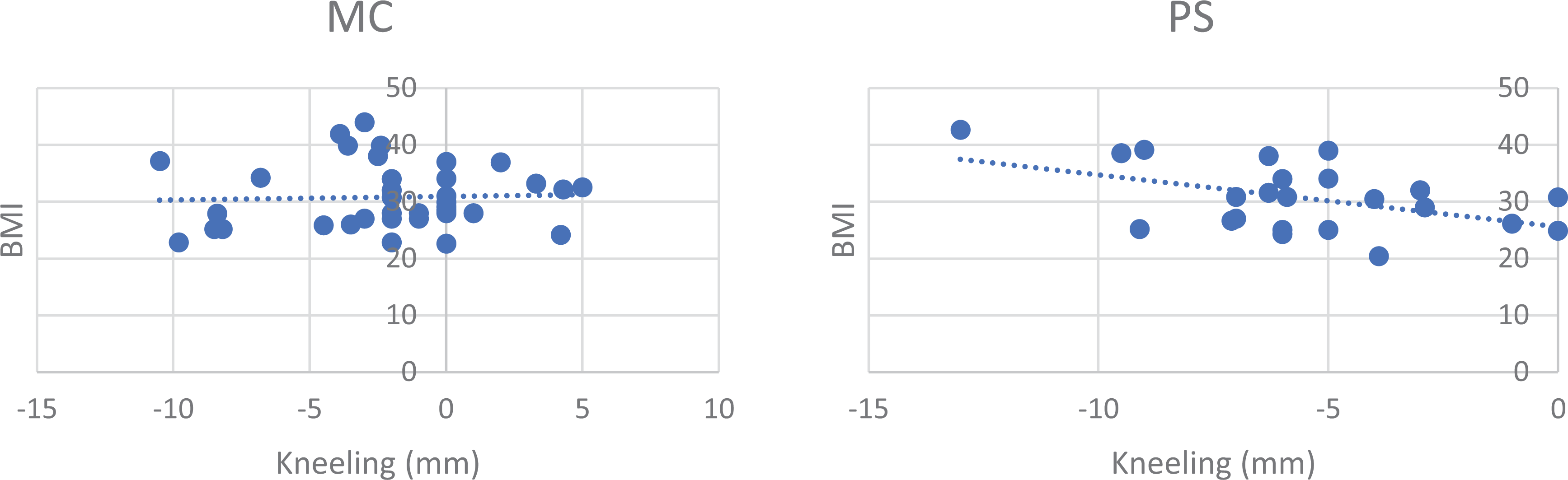
Correlation between “kneeling view” values and BMI values in MC group and PS group (P = 0.07; N.S.).
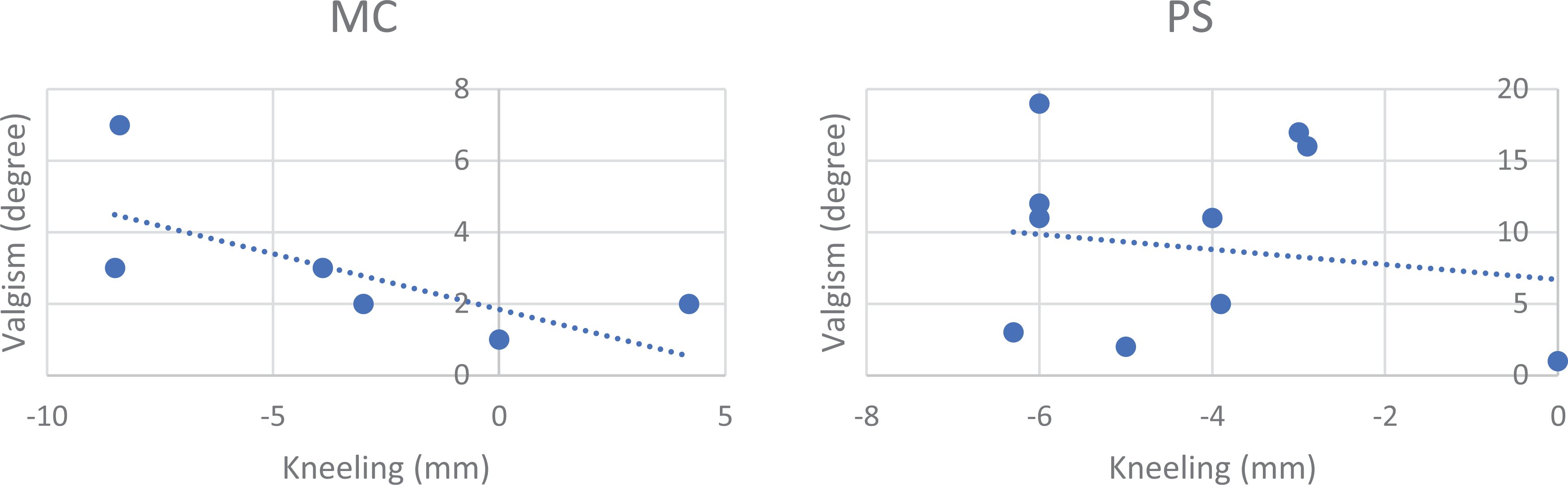
Correlation between “kneeling values” and preoperative valgus deformity value in MC and PS groups (P = 0.07; N.S.).
Discussion
This study utilized a well-established 15 –17 and reproductible 26 radiographic technique to demonstrate a statistically significant difference between the tibial posterior translation when two different polyethylene inserts, characterized by different level of constraint, are used in the same TKA design.
In our series, the PCL has always been intraoperatively removed: the reason for this surgical gesture relays on the fact that few studies confirmed that PCL retaining designs result in more technical difficulties fine tuning soft tissue balance, resulting in either stiffness or in flexion instability due to late PCL deficiency; 27,28 osteoarthritic knees, on the other side, often present a PCL characterized by a major myxoid degeneration leading to loss of its biomechanical properties. 29,30 Postero-stabilized (PS) implants have been originally designed to overcome any variable linked to the presence of the PCL; medial pivot or MC implants have the theoretical advantage to better reproduce the normal knee kinematic. 31
The current authors were not able to confirm the null hypothesis of this study. We demonstrated a statistical difference between the two particular designs in terms of tibiofemoral contact point on kneeling X-rays: on the other side, in the MC design, the high conformity on its medial compartment prevented posterior translation of the tibia respect to the femoral component posterior condyles. Our findings in the MC group differ from the previous literature showing that, after sacrifice of the PCL, many TKA designs showed significant posterior tibial translation compared to normal knees. 32 The current authors justified this finding according to the specific more posterior dwell point on the MC insert when compared to CR and PS polyethylene (PE) designs 33 : in fact, in the kneeling x-ray, we could detect that the insert stays congruent with the medial femoral condyle in a more anterior position thanks to the 1/1 ratio between the J-curve shaped condyle and the fully congruent insert. In addition to this, even though the tibia and the baseplate showed a greater posterior draw when compared to PS, the MC insert might diminish the amount of shear forces on the PE and by that count avoid conflict between the elevated posterior lip of the insert and the posterior cortex of the femur during high flexion; it has also been demonstrated that more conforming surfaces could diminish the risk of degradation of the PE. 34 –36 Our findings are similar to those one of Hoffman et al., 37 who showed that an ultracongruent insert clinically replicates the function of an efficient PCL.
The current authors agree with several other authors 17,38 suggesting that stress X-rays are more reliable and reproducible to assess the posterior stability than the clinical exam or the arthrometer. The “kneeling view” has been proposed as a method to objectively measure posterior knee laxity during weightbearing, 39 both in the sports medicine 11,39 as well as in the adult reconstruction scenario 16 where it can offer an objective, quantifiable and noninvasive tool that can be used to augment the diagnosis of TKA instability.
Historically, PS designs showed a “paradoxical motion” during active ROM when tested with fluoroscopy 40 : this undesired phenomenon has been linked to several complications, including anterior knee pain, poor ROM and patellar instability 41 The kneeling view has been described by Louisia and Bartlett 16 as a great method to quantify the amount of this anterior translation under weightbearing circumstances: patients with a PS implant showed a mean anterior movement of the tibia between 7 and 10 mm, with very few patients having a posterior translation compared to their preoperative status; their findings were similar to those of the current study, where we showed a mean anterior translation of 5.6 mm in the PS group. The anterior translation measured in the current study demonstrated that very high constraints may be applied on the PE post for this particular design of PS insert, increasing the fear for polyethylene wear even though vitamin E added polyethylene inserts were used in all patients. 42,43
The current study also confirms that when a precise surgical technique is combined with a modern polyethylene design, a satisfactory stability can be obtained without the need for an increased level of constraint as recently shown by Meneghini et al. 44
The current authors recognize that their study is a radiological more than a clinical assessment of patients who underwent primary TKA. Nevertheless, in our study, we noticed that, despite the very short follow-up, the flexion of our implants was very satisfactory (mean of 116.5 ± 10.4° degrees for in the PS group and mean of 114.9 ± 9.9° in the MC group); this finding is in line with the current literature. 45 Since instability is often a subdolous cause of TKA failure and this study has a short clinical FU, the authors were not able to predict any difference in survivorship between the two designs; on the other side, MC insert was contemplated as a mean to diminish shear forces at the bearing surface and we hypothesize that it would get less fatigue wear and thus reduce polyethylene wearing
The current study has several limitations. First, although stress radiography has been shown to provide an objective measure of posterior instability, 38,39 its accuracy can be influenced by several important components. Patient compliance and pain tolerance, radiographic technique, and exact landmark identification during measurements, all represent variables difficult to be quantified and represent a potential limitation to the use of kneeling stress radiography and must be carefully recognized. On the other side, Osti et al. 17 showed that the kneeling view can be considered, in terms of forces applied, a reliable and reproducible alternative method for the routine radiographic evaluation of the posterior knee laxity since the average amount of forces applied during the test was at least 75% of the body weight of each subject.
Another potential source of variability in the measurements is imprecise radiography: the identification of the radiographic landmarks can be influenced by rotation of the femoral condyles or by imprecise x-ray beam direction. The current authors optimized the accuracy of kneeling stress radiographs by carefully reproducing patient positioning, by overlapping of the posterior femoral condyles during the exam and by constantly reproducing the same magnification factor.
Conclusion
This study shows that stress radiography represents an excellent method to evaluate and quantify the degree of posterior tibial translation after primary TKA. When comparing different designs using this diagnostic technology, the authors showed that medially congruent TKA represents a satisfactory PCL substitution alternative without increasing the risk of implant instability during weightbearing activities at 90 degrees of flexion. Greater number of patients and long-term follow-up are warranted in order to validate the findings of the current study.
Footnotes
Authors' Note
Nicolo’ Bassi, Tommaso Amoroso, and Leonardo Osti are now Visiting Scholars at Stanford University School of Medicine, Stanford, CA, USA.
Acknowledgements
We thank Heather Maughan for her review that greatly improved the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.