
Abstract
Objective
In revision total knee arthroplasty (rTKA), metaphyseal sleeves represent an effective modality for managing metaphyseal bone defects. The purpose of this study was to clearly stratify patients with different grades of metaphyseal bone defects while evaluating the mid-term clinical outcomes and survival rate of metaphyseal sleeves.
Methods
A retrospective study was conducted on 58 patients who underwent revision total knee arthroplasty (rTKA) with metaphyseal sleeves between May 2018 and September 2022. Bone defects were classified using the Anderson Orthopaedic Research Institute (AORI) classification system: patients with AORI type I and IIA defects were categorized as having mild bone defects, while those with AORI type IIB and III defects were defined as severe bone defects. Clinical outcomes, including the visual analog scale (VAS) for pain, range of motion (ROM), Hospital for Special Surgery (HSS) score, Knee Society Score (KSS), Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), and Short Form-12 (SF-12) health survey, were recorded preoperatively and during the entire follow-up period. Linear mixed-effects models were employed to analyze repeated-measure outcomes, and Kaplan–Meier analysis was utilized to estimate the survivorship of metaphyseal sleeves.
Results
The mean duration of follow-up was 66.6 months, with a range of 30 to 85 months. All clinical outcome metrics exhibited a statistically significant improvement compared with preoperative values (p < 0.001), and both the mild and severe defect groups demonstrated analogous postoperative recovery trajectories. No sleeve-related complications or failures were observed, including aseptic loosening, periprosthetic fracture, or deep periprosthetic infection. Kaplan–Meier analysis yielded an estimated 5-years metaphyseal sleeve survivorship of 100%.
Conclusion
These findings demonstrate that metaphyseal sleeves provide reliable midterm fixation and significant functional improvements in patients undergoing revision total knee arthroplasty (rTKA), irrespective of the severity of metaphyseal bone defects.
Introduction
Total knee arthroplasty (TKA) is a well-established and effective treatment for end-stage symptomatic knee osteoarthritis, yielding significant improvements in joint pain and functional capacity.1,2 The widespread global adoption of TKA, combined with expanding indications for younger and more active patients, has contributed to an increasing number of revision TKA (rTKA) procedures anticipated in the coming decades. 3 Revision knee arthroplasty is inherently more technically demanding than primary TKA, and is associated with relatively higher complication rates and reduced implant survivorship. 4 Common causes of failure necessitating revision include aseptic loosening, osteolysis, periprosthetic joint infection (PJI), instability, postoperative stiffness, and periprosthetic fracture. 5 These conditions often result in varying degrees of metaphyseal bone defects, posing additional challenges to achieving durable implant fixation and restoring appropriate joint mechanics. 6
Bone defect classification is most commonly guided by the Anderson Orthopaedic Research Institute (AORI) system, 7 which stratifies defects into type I, type II (with subtypes IIA and IIB), and type III based on the extent and location of metaphyseal destruction. 8 Type I defects involve intact metaphyseal bone and minimal bone loss; type IIA defects involve contained defects with partial metaphyseal involvement; type IIB defects involve uncontained or bicondylar defects; and type III defects represent extensive loss of supportive metaphyseal bone with compromised cortical structure and ligamentous attachments.9,10 In cases of moderate to severe metaphyseal bone loss, durable fixation depends not only on diaphyseal stem stability but increasingly on achieving reliable metaphyseal fixation, as emphasized by the Morgan-Jones zonal fixation concept. 11
Metaphyseal sleeves are porous-coated, press-fit fixation devices designed to enhance metaphyseal engagement, promote osseointegration, and provide stable load transfer, thereby reducing stress shielding and minimizing the risk of implant migration or loosening. 10 Prior short- and midterm studies have reported encouraging osseointegration rates and favorable survivorship using metaphyseal sleeves 12 ; however, there remains a relative scarcity of medium-to long-term cohort studies, particularly those comparing outcomes among varying severities of metaphyseal defects. 13 Given the increasing utilization of metaphyseal fixation strategies in rTKA, a clearer understanding of midterm clinical performance is needed.
The present study was designed to address this gap by evaluating the midterm survivorship and functional outcomes of metaphyseal sleeves in patients undergoing rTKA, with additional emphasis on comparing the clinical performance of sleeves in mild versus severe metaphyseal bone defects as defined by the AORI classification. By analyzing a consecutive cohort with standardized surgical technique and comprehensive follow-up, this study provides important insights into the reliability, durability, and clinical utility of metaphyseal sleeves in revision knee reconstruction.
Methods
Patients
The inclusion criteria for this study were as follows: patients who underwent revision total knee arthroplasty (rTKA) combined with metaphyseal sleeve implantation between May 2018 and September 2022; patients with complete clinical and imaging data; and patients with a follow-up duration of more than 12 months and regular continuous follow-up visits. The exclusion criteria were as follows: presence of periprosthetic fractures secondary to trauma after primary total knee arthroplasty (TKA); active tuberculosis infection; hemorrhagic disorders/coagulopathy; lower extremity muscle paralysis; knee joint–surrounding muscle weakness of any etiology; and general inability to tolerate anesthesia or surgical procedures.
Surgical procedures
All revision total knee arthroplasties (rTKA) with metaphyseal sleeve implantation were performed by the same consistent team of senior orthopedic surgeons. A standardized metaphyseal sleeve system and uniform cementless fixation technique were applied to all patients.
1. Preoperative preparation
Preoperative evaluation included assessment of general medical status, knee anteroposterior/lateral radiographs, standing weight-bearing full-length lower extremity radiographs (for alignment), and 3D CT with metal artifact reduction (MAR) (for metaphyseal bone stock). Perioperative management included correction of anemia and hypoalbuminemia, optimization of osteoporosis, and adjustment of blood pressure and glucose to meet perioperative safety standards.
2. Surgical procedures: Incision and exposure
Under general anesthesia with the patient in the supine position, a pneumatic tourniquet was maintained at 240 mmHg. Via the original surgical approach, partial resection of the infrapatellar fat pad, excision of hyperplastic synovium, removal of femoral and tibial osteophytes, soft tissue release, patellar eversion, and joint exposure were performed sequentially. The existing spacer and primary prosthesis were removed, followed by thorough debridement of scar tissue and bone cement inside/outside the medullary cavity (with care to prevent iatrogenic fractures and excessive bone loss). Subsequent steps included tibial medullary cavity preparation, proximal tibial osteotomy, distal femoral osteotomy, establishment of tibial rotational alignment, management of tibial defects, trial reduction, selection of appropriately sized prostheses, component assembly and fixation, incision irrigation, and layered suturing. Intraoperative findings are illustrated in Figure 1. Intraoperative photograph showing bone surfaces prepared for the insertion of metaphyseal sleeves.
3. Postoperative management
A closed suction drainage tube was clamped for 2 h and then loosened for 10 min in a cyclic manner. Subcutaneous anticoagulation with low-molecular-weight heparin was initiated 12 h postoperatively. After emergence from anesthesia, patients were instructed to perform active quadriceps and hamstring contraction-relaxation exercises of both lower limbs. Following drainage tube removal, patients were guided to conduct active knee flexion-extension exercises and intensify lower limb muscle contraction-relaxation training.
Survival analysis
The primary endpoint was metaphyseal sleeve survival, defined as the time from index surgery to the first revision surgery for any cause (including aseptic loosening, infection, dislocation, or periprosthetic fracture). Patients who died without revision were censored at death. Those lost to follow-up were censored at their last clinical visit.
Outcome measurement
Patients were followed up at 3, 6, and 12 months postoperatively, followed by annual visits thereafter. Outcome measures for comparative analysis included the American Knee Society Score (KSS), Hospital for Special Surgery (HSS) Knee Score, visual analog scale (VAS) for pain, Short Form-12 (SF-12) Health Survey, and Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC). Knee range of motion (ROM) was additionally compared with preoperative measurements. Patient satisfaction was assessed using a 10-point linear visual analog scale (VAS). Patients with AORI type I/IIA defects were assigned to the mild defect group (Group A), and those with AORI type IIB/III defects to the severe defect group (Group B). The mean difference between preoperative and last follow-up VAS scores was estimated via a linear mixed-effects model with random intercepts and slopes, adjusting for individual follow-up durations.
Statistical analysis
Continuous data with a normal distribution (confirmed via Shapiro-Wilk test) were presented as mean ± standard deviation. Intergroup comparisons of baseline demographic and clinical data were conducted using independent samples t-tests. Repeated-measures data (e.g., VAS pain scores) were analyzed with linear mixed-effects models to account for intra-subject temporal correlations. The models included fixed effects of time, group, and time-group interaction, with a random intercept for each participant; residuals were assumed to follow an autoregressive [AR(1)] covariance structure. Kaplan–Meier survival curves were generated to estimate implant survivorship, and the log-rank (Mantel–Cox) test was used for intergroup comparisons of survival distributions. A two-sided p < 0.05 was considered statistically significant. All statistical analyses were performed using SPSS 27.0 (IBM Corp., Chicago, IL, USA), and Kaplan–Meier curves were plotted with GraphPad Prism 10.1 (GraphPad Software, San Diego, CA, USA).
Results
General information
Causes for revision TKA.

Bone loss according to the AORI classification.

No intraoperative injuries to the medial and lateral collateral ligaments or periarticular tendons were observed. Additionally, no cases of neurovascular injury, extensor mechanism rupture, or periprosthetic fracture occurred. The mean operative time was 2.3 ± 0.44 h, and the mean intraoperative blood loss was 286 ± 52.0 ml.
Comparison of basic patient information between the two groups.

Clinical efficacy
The mean follow-up duration was 66.6 months (maximum, 85 months). No symptomatic lower extremity deep vein thrombosis occurred during follow-up. At final follow-up, no patients developed complications including infection, periprosthetic loosening, or periprosthetic fracture. One patient sustained an isolated tibiofibular fracture at the 3-months postoperative follow-up, which was managed with open reduction and internal fixation using a cortical bone plate; the patient had uneventful postoperative recovery, with no metaphyseal sleeve loosening observed during subsequent follow-up.
Comparison of outcome indicators and clinical scores in Group A (n = 25).

Note. Data are presented as mean ± SD. Mean Difference = last follow-up minus preoperative value. “Estimate per month” represents the fixed effect of continuous time (in months since surgery: 0, 3, 12, individual last follow-up [mean = 66.6]) from a linear mixed-effects model with random intercepts and slopes for subjects. All p values <0.001. The quadratic term for time was significant for all outcomes (p < 0.001), indicating decelerating improvement over time.
Comparison of outcome indicators and clinical scores in Group B (n = 33).
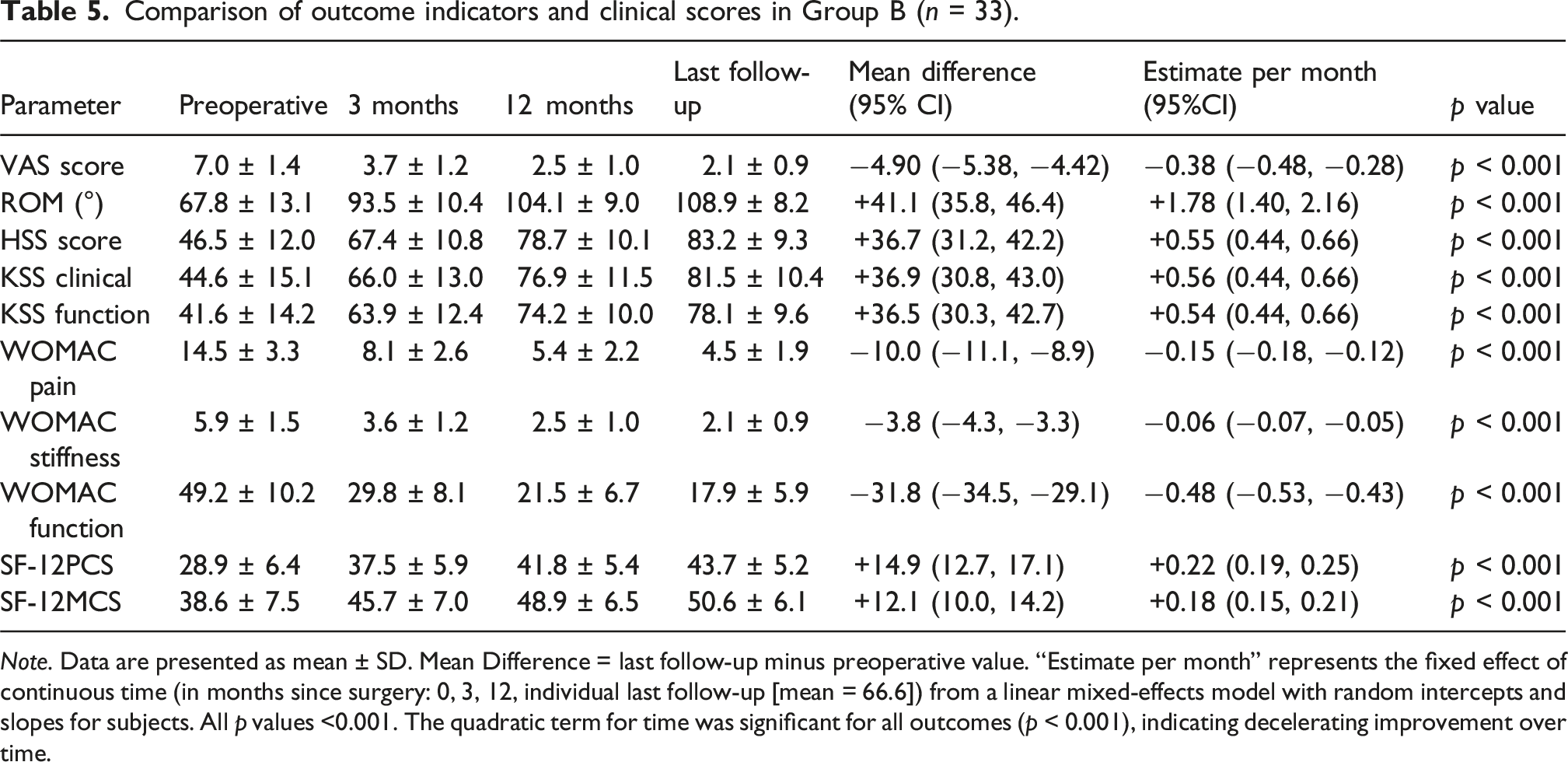
Note. Data are presented as mean ± SD. Mean Difference = last follow-up minus preoperative value. “Estimate per month” represents the fixed effect of continuous time (in months since surgery: 0, 3, 12, individual last follow-up [mean = 66.6]) from a linear mixed-effects model with random intercepts and slopes for subjects. All p values <0.001. The quadratic term for time was significant for all outcomes (p < 0.001), indicating decelerating improvement over time.
In Group A, the mean VAS pain score decreased from 7.1 ± 1.3 preoperatively to 1.7 ± 0.8 at final follow-up (mean reduction: 5.40 points; 95% CI: −5.91 to −4.89). Knee range of motion (ROM) improved from 68.4° ± 12.5° to 110.3° ± 7.7°, and the HSS score increased by 37.3 points to 84.6 ± 8.9. Similarly, Group B exhibited comparable substantial improvements: VAS score declined from 7.0 ± 1.4 to 2.1 ± 0.9 (mean difference: −4.90; 95% CI: −5.38 to −4.42), ROM increased by 41.1° to 108.9° ± 8.2, and HSS score improved by 36.7 points to 83.2 ± 9.3. Both groups also showed significant improvements in all WOMAC subscales (total, pain, stiffness, function), KSS clinical/functional scores, and SF-12 Physical Component Summary (PCS)/Mental Component Summary (MCS) scores (all p < 0.001).
Linear mixed-effects modeling demonstrated a highly significant fixed effect of time on all outcomes (p < 0.001); the quadratic term for time was also significant (p < 0.001) in both groups, consistent with a nonlinear recovery trajectory: rapid improvement in the early postoperative period, followed by gradual deceleration toward a plateau. All patients achieved independent ambulation without external support, with 3 patients reporting mild intermittent claudication.
Imaging evaluation
Postoperative radiological evaluations (plain radiographs) showed that host bone was well-integrated with the metaphyseal sleeve in all 58 patients during follow-up. No radiolucent lines >1 mm were identified at the interfaces of the femoral prosthesis, tibial prosthesis, or bone cement.
Regarding implant survival, no metal sleeve–related failures (defined as aseptic loosening, periprosthetic joint infection, or reoperation for sleeve-related complications) occurred in either group throughout follow-up. As shown in Figure 2, Kaplan–Meier analysis estimated a 5-years metaphyseal sleeve survival rate of 100% for both Group A (95% CI: 86.3%–100%) and Group B (95% CI: 89.3%–100%). Owing to the absence of failure events, formal intergroup statistical comparison was not possible; however, these results indicate excellent mid-term stability of metaphyseal sleeves in both mild and severe defect cases. All prostheses remained radiographically and clinically stable, with no complications (e.g., infection, dislocation, periprosthetic fracture) observed. Typical cases are shown in Figures 3 and 4. Kaplan-Meier survival curves for metaphyseal sleeves survival. A 61-year-old female underwent revision total knee arthroplasty due to aseptic loosening of the temporary prosthesis after temporary implant placement for TKA. These are preoperative (a, b), postoperative (c, d) and 4-years post-operative (e, f) radiographs obtained via the metaphyseal sleeve. A 67-year-old female patient underwent knee revision surgery due to prosthesis loosening and T2a-type bone defects after total knee arthroplasty (TKA). (a, b) Preoperative radiograph. (c, d) Postoperative X-ray. Three months after revision surgery, the patient experienced an accidental tibiofibular fracture. The patient underwent cortical plate fixation. (e, f) are preoperative radiographs. (g, h) are postoperative radiographs. X-ray images at the last follow-up (i, j) revealed that the prosthesis was still stable.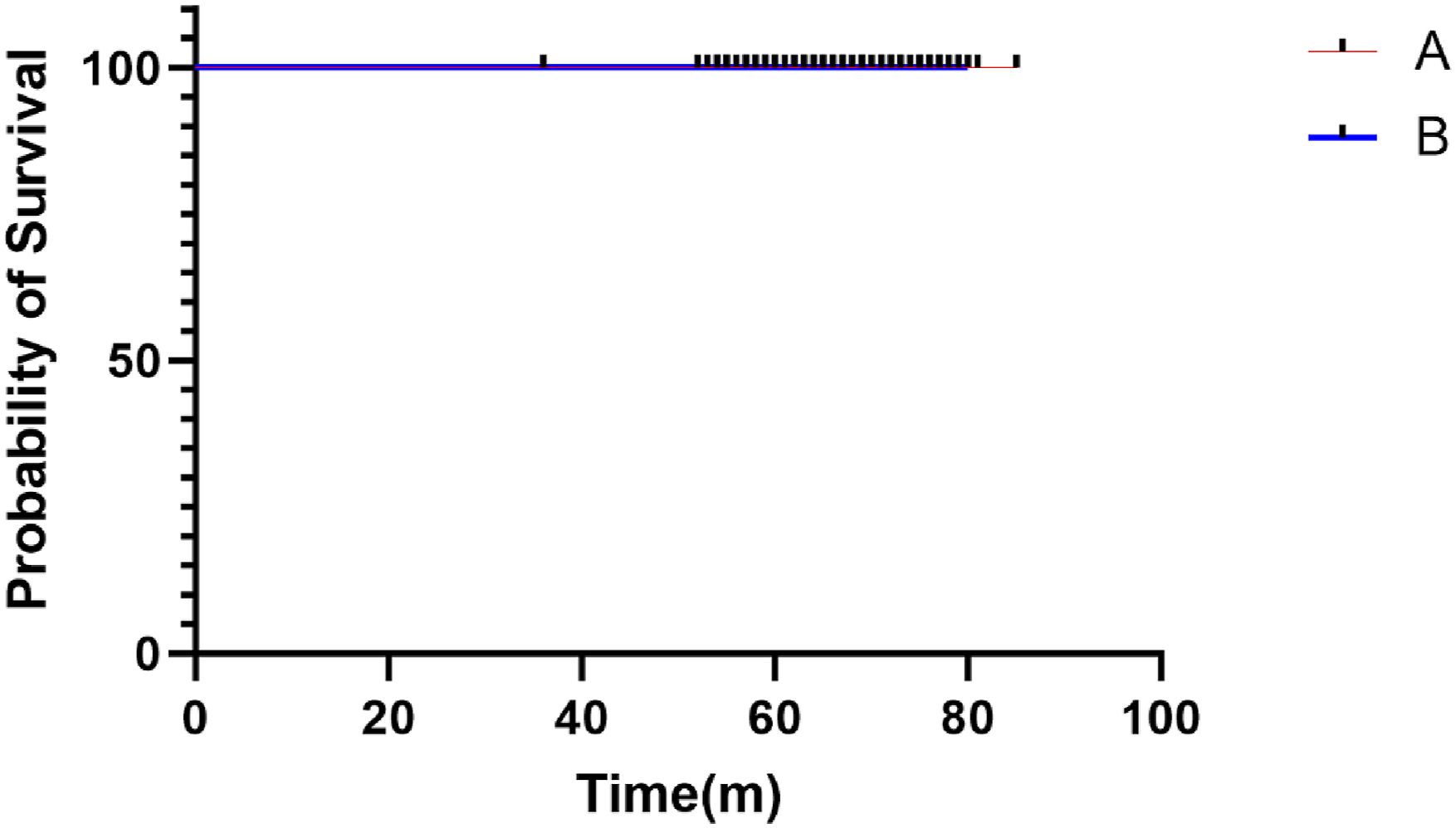


Complications
No wound complications, superficial infections, neurovascular injuries, extensor mechanism ruptures, or periprosthetic fractures occurred in any patient. Two patients developed delayed wound healing postoperatively, which resolved with serial dressing changes; complete wound healing was achieved by 4 weeks postoperatively.
Patient satisfaction
Of the total patients, 82.8% reported a postoperative satisfaction score of ≥8 points (Figure 5). Only 4 patients had a satisfaction score below 6 points. Patient satisfaction rating after surgery (score ranging from 1–10).
Discussion
Main findings of this study
This study evaluated the mid-term clinical efficacy and implant survivorship of metaphyseal sleeves in 58 patients undergoing revision total knee arthroplasty for varying degrees of metaphyseal bone loss, with a mean follow-up of 66.6 months (5.5 years). Both cohorts demonstrated significant and sustained improvements in pain (VAS), range of motion (ROM), knee-specific scores (HSS, KSS), WOMAC domains, and quality of life (SF-12) from baseline to final follow-up (p < 0.001). Postoperative recovery followed a nonlinear trajectory: rapid early functional gains, then a plateau, which aligns with previously reported revision arthroplasty recovery patterns.
The key finding was the excellent mid-term survivorship of metaphyseal sleeves: no sleeve-related failures (e.g., aseptic loosening, periprosthetic joint infection, mechanical failure, or sleeve-associated reoperation) were observed during follow-up. Kaplan–Meier analysis estimated a 100% 5-years survival rate in both groups, which is consistent with prior midterm studies reporting 95%–100% survivorship for such sleeves.14–16 Radiographically, no interfacial radiolucent lines >1 mm were detected, and all cases showed stable osseointegration, confirming the biological and mechanical stability of metaphyseal sleeves.
Review of the literature concerning the application of artificial prostheses in revision total knee arthroplasty.

Notes: “a” indicates missing data.
Advantages of metaphyseal metal sleeves in revision total knee arthroplasty.
The favorable fixation performance of metaphyseal sleeves likely stems from their unique biomechanical and biological properties. 20 Their porous-coated press-fit construct enables immediate mechanical stability while facilitating bone ingrowth, thereby enhancing long-term biological fixation. 23 Compared with traditional diaphyseal stem-dependent designs, metaphyseal fixation mitigates stress shielding via more physiological load distribution within the metaphysis. 24
Restoring stable metaphyseal support helps preserve joint-line position, optimize limb alignment, and lower the risk of mechanical failure. 25 Moreover, sleeve fixation preserves the option for future revision procedures by minimizing additional bone loss, which is particularly valuable in younger revision candidates. 26
Analysis of the clinical results and treatment of bone defects
The results of this study align with and expand upon previous findings. Short- and midterm analyses by Bugler et al., Martin-Hernandez et al., Bloch et al., and others have consistently demonstrated high osseointegration rates and low reoperation rates with metaphyseal sleeves.10,14,17,20 Studies that included more severe AORI type IIB and III defects similarly reported durable metaphyseal fixation and acceptable functional outcomes.21,27 However, many of these earlier reports included heterogeneous surgical techniques, varied implant systems, or smaller sample sizes.12,23 The current study strengthens existing evidence by incorporating a uniform surgical approach, standardized postoperative follow-up, and subgroup comparisons across clearly defined defect categories.
Strengths and limitations
Existing literature similarly reports high osseointegration rates (>95%) and low aseptic loosening rates with metaphyseal sleeves. 28 The current findings extend these observations by demonstrating consistent midterm outcomes even in severe defects (AORI IIB–III). The uniform surgical technique and consistent construct selection further strengthen the interpretability of the results.
Nonetheless, this study is limited by its retrospective design, modest sample size, heterogeneous revision indications, and lack of long-term (>10 years) follow-up. The absence of sleeve failures, while encouraging, limits the ability to identify risk factors for failure. Future research should include multicenter prospective cohorts and biomechanical analyses comparing sleeves with metaphyseal cones.
Conclusion
In summary, this study provides strong evidence that metaphyseal sleeves offer excellent midterm fixation, substantial improvements in pain and function, and exceptional implant survivorship in rTKA. Their ability to provide stable, durable fixation across the full spectrum of metaphyseal bone defects underscores their value in contemporary revision knee reconstruction. These findings contribute to the growing body of literature that supports metaphyseal sleeves as a reliable and effective solution in the management of metaphyseal deficiency in revision total knee arthroplasty.
Footnotes
Ethical considerations
This study was approved by the Institutional Review Board (IRB) of West China Hospital, Sichuan University (No.159 in 2022). This is a retrospective observational study. Data collection was conducted from 2018 to 2022, and retrospective registration was completed on Chinese Clinical Trial Registry in 2025 (Registration Number: ChiCTR2500109427) due to the initial positioning of the study as an internal clinical outcome summary. All procedures were performed in accordance with the ethical standards of the 1964 Declaration of Helsinki and its later amendments.
Consent to participate
For retrospective studies, the requirement for informed consent was waived by the IRB due to the anonymous and non-interventional nature of the data analysis.
Author contributions
P.K. and D.L. contributed to the conception and design of the study. Material preparation and data collection were performed by S.S and G.H.. Q.W. and Y.C. performed the analysis. The first draft of the manuscript was written by Q.W., and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China [No. 82372392].
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data of this study were stored at West China Hospital, Sichuan University. If you have any questions, please contact the corresponding author of this article.