
Abstract
Purpose:
We have analyzed the surgical outcomes of primary total knee arthroplasty (TKA) using computer-assisted (CA) navigation in terms of postoperative coronal alignment depending on preoperative lateral femoral bowing.
Methods:
We conducted a retrospective study of patients who have undergone navigated primary TKA from January 2016 through January 2020. Two hundred and ninety-nine cases with lateral femoral bowing of 3° or less were assigned to group 1, 95 cases of lateral femoral bowing between 3° and 5° were assigned to group 2, and 89 cases with lateral femoral bowing of more than 5° were assigned to group 3. The postoperative mechanical hip–knee–ankle (mHKA) angle was measured from scanograms, which were taken 3 months after surgery. The appropriate range of coronal alignment was set as 0 ± 3°.
Results:
The number of outliers of mHKA occurred was 31 cases (10.4%) in group 1, 17 cases (17.9%) in group 2, and 17 cases (19.1%) in group 3. There was a significant correlation between the degree of lateral femoral bowing and the occurrence rate of mHKA outliers. Multiple variables logistic regression analysis showed occurrence rate of outliers in group 3 to be 2.04 times higher than group 1. After adjusting the patient’s age, sex, body mass index, and preoperative HKA deformity, the occurrence rate of outliers in group 3 was still 1.96 times higher than group 1.
Conclusion:
The benefit of CA navigation during TKA in obtaining coronal alignment within 0 ± 3° may be lessened when the preoperative lateral femoral bowing is severely advanced.
Introduction
While performing conventional total knee arthroplasty (TKA) in patients with lateral femoral bowing, achieving the mechanical coronal alignment of 0 ± 3° 1 may be hard because bone cutting is based on the bony indices of the distal femur. 2 –6 The use of computer-assisted (CA) navigation is recommended by many surgeons as a solution for such situations. 6 –10 The CA navigation system only considers bony indices of the femoral head and the distal femur. Therefore, it can obtain the mechanical coronal alignment of 0 ± 3°, regardless of the femoral bowing at the level of the diaphysis and metaphysis. However, precise registration of the bony index is a prerequisite for so. In a previous study, we have found out that the greater degree of varus deformity resulted in higher occurrence rate of outliers of postoperative mechanical coronal alignment of 0 ± 3°, which was thought to be a result of erroneous registration of ambiguous bony markers with varus deformity. 11 We have also found out that a higher degree of varus deformity resulted in increased lateral bowing. 12
We have tried to find out if TKA using CA navigation system would enable patients with lateral femoral bowing to achieve similar surgical outcomes (mechanical coronal alignment of 0 ± 3°) with patients with no femoral bowing. We have also tried to find out the correlation between the degree of lateral femoral bowing and surgical outcomes. The study plan was based on the hypothesis that patients with lateral femoral bowing would show a higher occurrence of outliers of postoperative mechanical coronal alignment than patients without lateral femoral bowing, due to increased error during the registration of bony markers, which is similar with patients in advanced varus deformity. For the same reason, we have hypothesized that patients with more severe degree of lateral femoral bowing would show a higher occurrence rate of outliers of postoperative coronal alignment.
According to the study by Lasam et al., an average of 3° of femoral lateral bowing was present in 60 people with normal knees. 4 Based on such knowledge, we have regarded the presence of lateral bowing in patients with more than 3° of lateral femoral bowing, and severe lateral bowing was defined as more than 5° of lateral femoral bowing. 13 We have compared the occurrence rate of outliers of postoperative coronal alignment between patients with severe lateral bowing and patients with less than 5° of lateral femoral bowing. We have targeted the postoperative mechanical hip–knee–ankle (mHKA) angle to be 0° and have set the appropriate range of coronal alignment as 0 ± 3°. 14
Methods
Patients
We conducted a retrospective study of patients who have undergone primary TKA by a single surgeon in our hospital from January 2016 through January 2020. The single surgeon is an expert in CA-TKA. He had been performing CA-TKA since 2008 and have performed CA-TKA in most of the cases of primary TKA since 2015. From January 2016 to January 2020, the surgeon has performed 574 cases of primary TKR. The primary reason for surgery was knee osteoarthritis (523 cases). Exclusion criteria were valgus deformity (29 cases), intraoperative change of procedure from CA-TKA to manual TKA (3 cases), and inappropriate preoperative or postoperative scanogram (8 cases). A total of 483 cases were enrolled in this study.
According to the degree of lateral femoral bowing, 299 cases with lateral femoral bowing of 3° or less were assigned to group 1, 95 cases of lateral femoral bowing between 3° and 5° were assigned to group 2, and 89 cases with lateral femoral bowing of more than 5° were assigned to group 3 (Table 1). Analyses on the degree of difference between the target mHKA angle (0°) and postoperative mHKA angles and on the occurrence rate of outliers were performed. This trial was conducted after approval of the Daegu Catholic University Medical Center Institutional Review Board (approval number: CR-20-141).
Epidemiology of all participants.

F: female; M: male; mHKA: mechanical hip–knee–ankle.
a Group 1: Femoral lateral bowing of 3° or less.
b Group 2: 3° < femoral lateral bowing < 5°.
c Group 3: Femoral lateral bowing more than 5°.
Surgical techniques
Tourniquets were applied in all operations. Midline skin incision and the medial parapatellar approach were applied in all the cases. The Imageless Navigation System version 2.6 (BrainLAB, Feldkirchen, Germany) was used in all navigation cases. Measured gap technique was used for bone resections. Both femoral and tibial components were fixed with bone cement. Cementation of both femur and tibia was done at once using Depuy CMW 3 bone cement. Posterior cruciate-substituting type of implant was used for all TKA.
Outcome measurement
Preoperative lateral femoral bowing, preoperative mHKA, mHKA at 3 months after surgery, and mechanical lateral distal femoral angle (mLDFA) at 3 months after surgery were measured using scanograms by two orthopedic surgeons who were not involved in this study. For accurate scanogram measurement, the patient is asked to stand in the presentation ceremony indicated in advance, and the measurements are performed with both patellas facing the front. When the measured values of the two orthropedic surgeons were different, we used the values measured by the more senior surgeon. The lateral bowing of the femur was measured as the angulation between the proximal and distal quarters of the femoral diaphysis 3 (Figure 1(a)). mHKA was defined as an angle formed by the mechanical axes of the femur and tibia. The mechanical axis of the femur was defined as a line that connects the center of the femoral head to the center of the intercondylar notch. The mechanical axis of the tibia was defined as a line that connects the center of the tibial spine to the center of the tibial plafond (Figure 1(b)). The mLDFA was defined as an angle formed by the mechanical axis of the femur and the line connecting the distal ends of the medial and lateral femoral condyles of the femur (Figure 1(c)). Postoperative mHKA and mLDFA were targeted to be 0° and 90°. The appropriate range of each value was set as 0 ± 3° and 90 ± 3°.
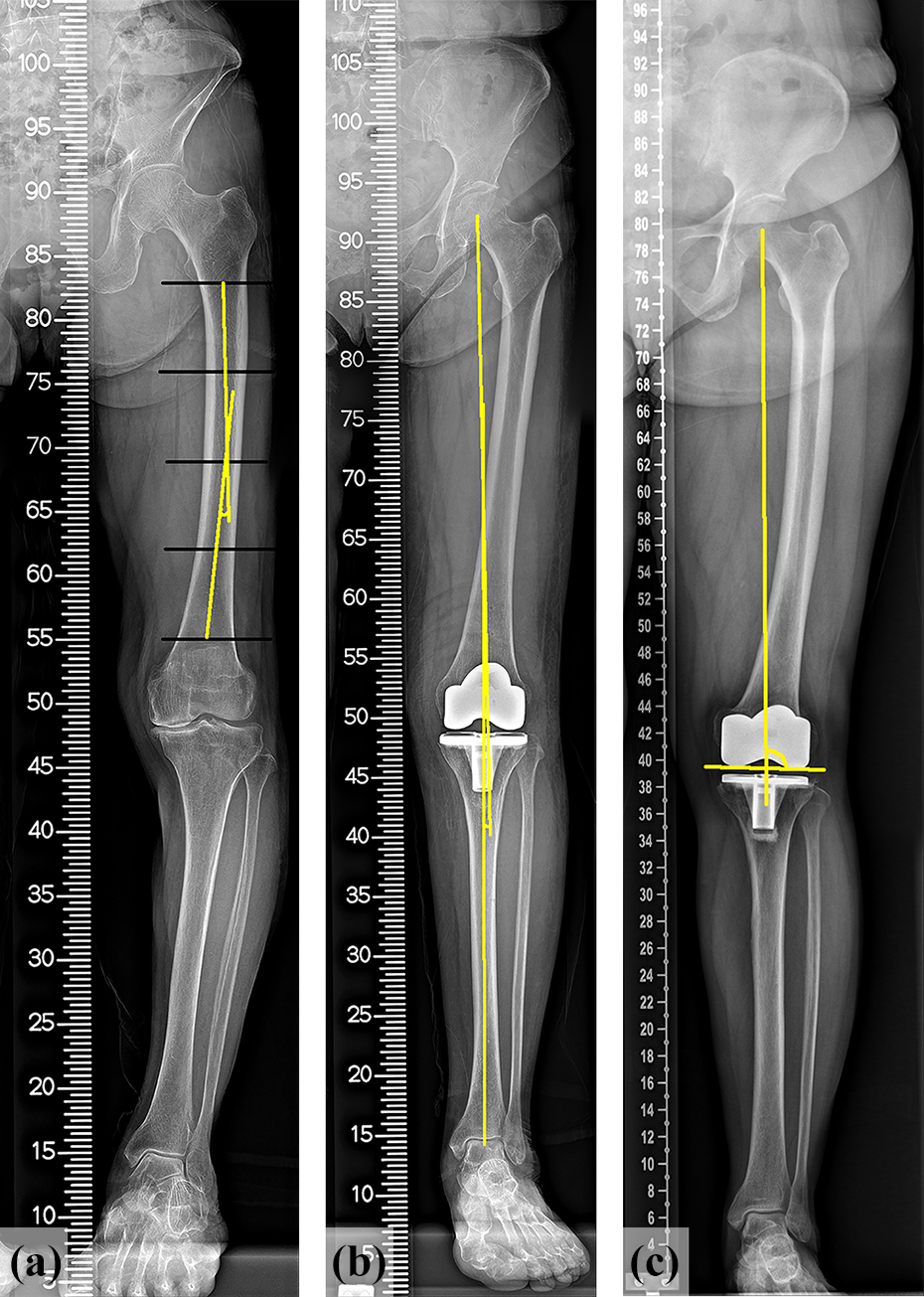
Radiographic measurements of (a) preoperative femoral lateral bowing, (b) postoperative mechanical hip–knee–ankle angle, and (c) postoperative mechanical lateral distal femoral angle.
Statistical analysis
All analyses were performed with IBM SPSS version 19.0 software (SPSS Inc., Chicago, Illinois, USA) for Windows. The χ 2 test, t-test, and one-way analysis of variance (ANOVA) test were used to identify the differences in errors and outliers of mHKA. A χ 2 test was used to identify the difference in outliers of mHKA, and t-test and one-way ANOVA test were used to determine the difference in errors of mHKA. The Pearson’s correlation coefficient was used to identify the association between the degree of preoperative lateral bowing and the absolute value of postoperative mHKA. A p-value of ≤0.05 was considered to be statistically significant.
Results
The interobserver reliability for measurement of the preoperative mHKA and lateral bowing was 0.954 (95% confidence interval (CI) 0.946–0.961) and 0.811 (95% CI 0.774–0.842), respectively. The interobserver reliability for measurement of the postoperative mHKA and mLDFA was 0.896 (95% CI 0.877–0.913) and 0.962 (95% CI 0.955–0.969), respectively (Table 2).
ICCs of radiographic measurements.

ICC: Intraclass correlation coefficient.
Absolute errors of coronal alignment (mHKA)
Among the 483 cases who met the inclusion and exclusion criteria, the absolute value of mHKA measured 3 months after surgery was 1.78 ± 1.30° on average. The mean values were 1.66 ± 1.23° in patients with lateral femoral bowing of 3° or less and 1.96 ± 1.39° in patients with lateral femoral bowing of more than 3°. The absolute error of postoperative coronal alignment was significantly higher in patients with preoperative lateral femoral bowing of more than 3° than in patients with preoperative lateral femoral bowing of 3° or less (p = 0.015).
The mean absolute value of mHKA measured 3 months after surgery was 1.66 ± 1.23° in group 1, 1.92 ± 1.42° in group 2, and 2.00 ± 1.37° in group 3. There was a statistically significant difference in the absolute error of postoperative coronal alignment between the three groups (p = 0.048), while least significance difference post hoc test only showed a statistically significant difference between groups 1 and 3 (p = 0.031).
Absolute errors of coronal alignment (mLDFA)
Among the 483 cases who met the inclusion and exclusion criteria, the absolute value of mLDFA measured 3 months after surgery was 92.08 ± 2.00° on average. The mean values were 92.10 ± 2.02° in patients with lateral femoral bowing of 3° or less and 92.04 ± 1.98° in patients with lateral femoral bowing of more than 3°. There was no significant difference in mLDFA between patients with preoperative lateral femoral bowing of more than 3° than in patients with preoperative lateral femoral bowing of 3° or less (p = 0.718).
Outliers of coronal alignment (mHKA)
Among all patients, 65 cases (13.5%) were detected as outliers (mHKA > 0± 3°) at 3 months after surgery. Thirty-one cases (10.4%) were affiliated to patients with lateral femoral bowing of 3° or less, and 34 cases (18.5%) were affiliated to groups 2 and 3. Patients with preoperative lateral femoral bowing of more than 3° showed a significantly higher occurrence of outliers than patients with preoperative lateral femoral bowing of 3° or less (p = 0.01; Table 3).
A χ 2 test to identify the difference in outliers (mHKA > 0 ± 3°).

mHKA: mechanical hip–knee–ankle, mLDFA: mechanical lateral distal femoral angle.
The number of outliers of mHKA occurred was 31 cases (10.4%) in group 1, 17 cases (17.9%) in group 2, and 17 cases (19.1%) in group 3. There was a significant correlation between the degree of lateral femoral bowing and the occurrence rate of mHKA outliers (p = 0.039; Table 4).
A χ 2 test to identify the difference in outliers (mHKA > 0 ± 3°).

mHKA: mechanical hip–knee–ankle; mLDFA: mechanical lateral distal femoral angle.
a Group 1: Femoral lateral bowing of 3° or less.
b Group 2: 3° < femoral lateral bowing < 5°.
c Group 3: Femoral lateral bowing more than 5°.
Outliers of coronal alignment (mLDFA)
When defining an appropriate range of mLDFA as 90 ± 3°, 134 cases (27.7%) were detected as mLDFA outliers at 3 months after surgery among all cases. Eighty-six cases (28.8%) were detected as mLDFA outliers in patients with lateral femoral bowing of 3° or less, and 48 cases (26.1%) were detected as mLDFA outliers in patients with lateral femoral bowing of more than 3°. There was no statistically significant difference in the occurrence rate of mLDFA outliers between the two groups (p = 0.236; Table 3).
Correlation between preoperative lateral femoral bowing and preoperative varus deformity
When the degree of lateral femoral bowing of patients with medial femoral bowing was set as 0, there was a statistically significant (p = 0.001) positive correlation (r = 0.268) between the degree of preoperative varus deformity and preoperative lateral femoral bowing.
Logistic regression analysis in difference in outliers of coronal alignment (mHKA > 0 ± 3°)
As a result of multiple variables logistic regression analysis, which analyzed the difference in outliers(mHKA > 0 ± 3°), an occurrence rate in group 3 to be 2.04 times higher than group 1 (p = 0.030) was shown. After adjusting the patient’s age, sex, body mass index (BMI), and severity of preoperative HKA deformity (whether the preoperative HKA was ≤10° or not), the occurrence rate of outliers in group 3 was still 1.96 times higher than group 1 (p = 0.050; Table 5).
Multiple variables logistic regression analysis, which analyzed the difference in outliers (mHKA > 0 ± 3°).

OR: odds ratio; CI: confidence interval; G1: group 1; G2: group 2; HKA: hip–knee–ankle.
a Group 1: Femoral lateral bowing of 3° or less.
b Group 2: 3° < femoral lateral bowing < 5°.
c Group 3: Femoral lateral bowing more than 5°.
d Adjusted by age, gender, body mass index, and preoperative HKA deformity.
Discussion
In a previous study, we have found out that obtaining the coronal alignment of 0 ± 3° may be not as effective as expected in patients with advanced varus deformity of the knee. 11 Similarly, we tried to identify whether the advantages of CA-TKA would also apply to patients with various degrees of lateral femoral bowing.
In this study, there were no statistically significant differences in postoperative mLDFA between the several degrees of preoperative femoral lateral bowing. In other words, the use of CA navigation may help to obtain the intended postoperative mLDFA of 90° regardless of the degree of lateral femoral bowing. Also, we have identified the association between the severity of lateral femoral bowing and error in postoperative coronal alignment after CA-TKA. Especially, in patients with more than 5° of lateral femoral bowing, the occurrence rate of outliers (mHKA > 0 ± 3°) was 2.04 times higher than in patients with lateral femoral bowing of 3° or less. Even after adjusting patient characteristics, such as age, sex, BMI, and preoperative HKA deformity, which may show synergistic effects with lateral femoral bowing deformity, the occurrence rate of outliers in patients with more than 5° of lateral femoral bowing was also 1.96 times higher than in patients with lateral femoral bowing of 3° or less. Thus, the advantages of CA-TKA might be canceled out in cases of severe preoperative lateral femoral bowing.
The degree of varus deformity may become worse as the extent of lateral femoral bowing deformity progresses more severely. We assume that this correlation may be the cause. In a previous study, we have found out a significant correlation between the extent of lateral femoral bowing deformity and varus deformity. We also found out a significant (p = 0.001) positive correlation (r = 0.268) between the extent of preoperative femoral lateral bowing and preoperative HKA angle. We assume that this is due to inaccurate registration of the ambiguous bony landmarks in the knees affected by lateral femoral bowing and varus deformity. According to Katz, increased varus deformity causes increased deformity of the femoral epicondyle (especially the medial epicondyle) and results in declined accuracy of the transepicondylar axis, which is one of the methods in determining femoral rotation. 15
In this study, the difference in postoperative mHKA between patients with lateral femoral bowing of 3° or less and patients with lateral femoral bowing over 3° was statistically significant, but the difference was 0.30° on average. Since the error during computer navigation may be high as up to 1°, 16 such difference may be meaningless. However, with respect to the occurrence rate of mHKA outliers (mHKA > 0 ± 3°), groups 2 and 3 showed significantly higher occurrence rates than group 1. According to this result, we have identified that preoperative advanced lateral femoral bowing may cancel out the advantage of CA-TKA.
This study has several limitations: firstly, the retrospective study design. However, since only eight cases (1.66%) were excluded due to inappropriate data settings, the selection bias may not be significant. Secondly, the accuracy in mHKA measurement. Since the measurement of mHKA angle values using long films is more accurate than using short films, we have conducted this study with only the data collected from 2016, when both preoperative and postoperative scanograms were taken using long films. Two skilled orthopedic surgeons have separately checked the measured values to obtain reliability.
Conclusion
The occurrence rate of outliers of postoperative coronal alignment (mHKA > 0 ± 3°) was higher in patients with more advanced lateral femoral bowing, and there was a positive correlation between the severity of lateral femoral bowing and the occurrence rate of mHKA outliers.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.