
Abstract
Background:
The Zimmer iASSIST system is an accelerometer-based, portable navigation device for total knee arthroplasty (TKA) that does not require the use of a large console for alignment feedback as required in computer-assisted surgery. The purpose of this study was to determine the accuracy of the accelerometer-based system in component positioning and overall mechanical alignment.
Methods:
Two groups of 30 patients each with primary osteoarthritis underwent TKA using either conventional method or Zimmer iASSIST navigation in 2013 was retrospectively studied. Patients were matched according to body mass index (BMI), gender and age. A senior arthroplasty surgeon performed all the operation using the same surgical approach. Perioperative and post-operative regimens were the same. All patients had standardized radiographs performed post-operatively to determine the lower limb mechanical alignment and component placement.
Results:
There was no difference between the two groups for age, BMI, gender, side of operated knee and preoperative mechanical axis (p > 0.05). There was no difference in the proportion of outliers for mechanical axis (p = 0.38), coronal femoral angle (p = 0.50), coronal tibia angle (p = 0.11), sagittal femoral angle (p = 0.28) and sagittal tibia angle (p = 0.33). The duration of surgery, post-operative drop in haemoglobin level and transfusion incidence did not show statistically significant differences between the two groups (p > 0.05).
Conclusions:
Our article showed that iASSIST was safe and remains a useful tool to restore mechanical axis. However, our data demonstrated no difference in lower limb alignment and component placement between the TKA that used accelerometer-based system and those that underwent conventional method.
Keywords
Introduction
Total knee arthroplasty (TKA) is effective in relieving pain and improves function in patients affected by arthritis. The success of joint replacement depends on several factors, including patient selection, prosthesis design, soft tissue balancing, the axial alignment of the leg and the restoration of the joint line. 1 Proper alignment of the prosthesis during TKA is critical in maximizing implant survival and ensure optimal functional outcome. Malalignment of the prosthesis has been reported to lead to abnormal tibial–femoral and patellar tracking, asymmetric distribution of stresses at the weight-bearing surfaces, accelerated polyethylene wear, aseptic loosening and poor functional outcome. 2,3
The conventional method uses an intramedullary guide for the distal femoral resection and either an extramedullary or intramedullary alignment jig for the tibia resection. However, these commonly used methods have limited degree of accuracy for both lower limb mechanical alignment and individual component placement. Based on the relative stability of the osseous anatomy, computer-assisted surgery (CAS) has been developed over the last 30 years to reduce surgical errors and ensure precise component positioning. Traditional image-free computer navigation systems utilize infrared communication system and advanced software to determine the spatial positioning of patient’s anatomy and surgical equipment. They require rigid placement of the femoral and tibial navigation trackers to the respective bones using either pins or a large diameter screw. 4 Compared to conventional techniques, these navigation systems have proven to improve the accuracy of components placement and reduce the proportion of outliers for lower limb mechanical axis. 5 However, their disadvantages include a longer duration of surgery 6 as well as pin-site-related complications such as pin-site pain, periprosthetic fractures of tibia and femur 7 –9 and pin-site infection 10 including osteomyelitis. 11
An imaging-based custom patient instrumentation system reduces the intraoperative workflow to a minimum and avoids the morbidity of pin-tract-related complications. However, it requires additional costs incurred by additional imaging procedures and preoperative trial measurement of prosthesis. Other concerns with CAS techniques including increased capital costs, longer operative times, intraoperative line of sight issues and the learning curve have limited its widespread acceptance. 1,12,13
More recently, navigation systems using accelerometer-based electronic components have been developed. 14,15 These devices aim to combine the alignment accuracy of the CAS systems with the familiarity of the traditional instruments while avoiding preoperative imaging and large computer console for registration and alignment feedback.
As accelerometer-based navigation systems are a relatively new concept with a limited number of systems available, there is a paucity of literature evaluating its intraoperative accuracy and clinical effectiveness in TKA. This study aims to investigate the effectiveness of a new accelerometer-based navigation system (Zimmer® iASSIST™ Knee) in reducing the proportion of outliers for lower limb mechanical axis and components mal-placement in TKA. The authors hypothesize that iASSIST™ navigation will improve coronal and sagittal alignments when compared to conventional techniques in TKA, without a significant increase in the duration of surgery.
Materials and methods
All patients who underwent unilateral TKA by a single surgeon in 2013 at a single institution were retrospectively reviewed. All patients with primary tricompartmental osteoarthritis of the knee were evaluated for inclusion of the study. Patients with inflammatory arthritis, gouty arthritis, post-traumatic osteoarthritis, pre-existing hip pathology or previous hip arthroplasty surgery were excluded. Patients who had undergone previous knee joint surgery or who could not be treated with an unconstrained TKA with a short stem were also excluded. A single surgeon randomly assigned patients who underwent TKA to either Zimmer iASSIST navigation or conventional method. In 2013, 60 eligible consecutive patients diagnosed with primary tricompartmental osteoarthritis of the knee who underwent unilateral TKA using the iASSIST accelerometer-based navigation system or conventional method by a single surgeon were identified. The matching of patients was undertaken using preoperative data in isolation. The two groups were matched for age, body mass index (BMI), gender, side of the operated knee and preoperative mechanical alignment of the lower limb. Thirty patients (30 knees) who underwent TKA with the accelerometer-based navigation system were individually matched with the control group of 30 patients (30 knees) who underwent TKA using conventional method to achieve neutral mechanical axis.
A senior adult reconstruction surgeon, who is well versed in both surgical techniques, performed all the surgeries. In the iASSIST™ group, patients underwent TKA using the Zimmer® iASSIST™ Knee navigation system (Warsaw, Indiana, USA). The operative workflow was similar to the conventional method in which each bone is resected independently along the mechanical axis. The system consists of small disposable electronic pods containing internal accelerometer with built-in local wireless capability that is attached onto the jigs. Alignment information is captured by the accelerometer when pods are manipulated within the surgical field and this information is displayed to the surgeon on a user interface on the pods directly within the surgeon’s field of view, to guide bony resections in sagittal and coronal planes to restore the mechanical alignment orientation. 16 This system does not require additional incisions to fix the jigs. Similar to most optical navigation systems, the mechanical axis of the femur was determined by locating the anatomical centre of the distal femur and kinematically locating the femoral hip centre using multiple stop-and-go circumduction movements of the femur by the surgeon. The mechanical axis of the tibia was determined by the anatomical centre of the tibia and centre of the ankle with the aid of a custom jig. The position of the resection jigs can be adjusted in varus/valgus and flexion/extension according to the feedback information, and bones were cut perpendicular to the respective mechanical axis. Alignment can be validated after the bony resection and any adjustment can be performed.
In the conventional group, patients underwent TKA using conventional technique based on the principles of the measured resection technique. The distal femur was prepared using an intramedullary rod with the valgus resection angle guide determined from preoperative long leg films. The proximal tibia was prepared using an extramedullary cutting jig perpendicular to the mechanical axis of the tibia. After inserting the trial components, overall lower limb alignment was assessed. The distal femur and proximal tibia resections were revisited if either of these checks revealed any deviation.
All surgeries were performed using the medial parapatellar quadriceps splitting approach with patellar eversion under tourniquet control at 350 mmHg. The surgical aim was to achieve neutral coronal alignment with a 180° mechanical axis and femoral rotation aligned with the transepicondylar axis and checked using Whiteside’s line. Soft tissue releases and ligament balancing were made to achieve rectangular flexion and extension gaps. All patients had implants from Zimmer® Nexgen® LPS-Flex system (Warsaw, Indiana, USA) and closure of wounds was performed in a standard manner. All patients underwent the same post-operative rehabilitation protocol with the aim of early mobilization. On the day after surgery, patients started active range of motion exercises of the knee and began standing at the bedside or walking with a walker or crutches under the supervision of a physiotherapist.
Outcome measures
The primary outcome of this study was post-operative radiographic assessment of lower limb alignment and components placement, while the secondary outcomes include the duration of surgery, perioperative drop in serum haemoglobin (Hb) level and blood transfusion incidence. Complications of TKA including surgical site infection, significant cardiac events (i.e. myocardiac infarction and arrhythmia), deep vein thrombosis, pulmonary embolism and death during the 30 days post-operative period were recorded.
All patients had standardized post-operative long leg radiographs taken in the outpatient clinic 1 month post-operatively when the patients were able to weight-bear fully. Coronal radiographs were taken with the patient standing and the knee in full extension on a 5-cm riser to visualize the ankle joint. Both lateral malleoli were placed 20 cm apart with the toes pointing forward. The patella was placed in the direction of the radiograph source as a rotation guide, with its anterior surface perpendicular to the radiograph source. Sagittal radiographs were taken with the patient standing and operated knee flexed forward at 30°. The epicondyles were placed perpendicular to the cassette. The patella should be perpendicular to the plane of the cassette, which serves as a guide. The radiograph beam was centred 2.5 cm distal to the medial epicondyle at 6° to 7° at a distance of 100 cm. Radiographs were repeated if malrotation was detected. In this study, malrotation was defined as: (1) asymmetry of the distal medial and lateral femoral condyles; or (2) unequal medial and lateral joint spaces in the ankle joint.
Evaluation of lower limb alignment using picture archiving and communication systems (PACS) had better inter- and intra-rater reliability than using hard copy radiographs and was selected as the method of radiological evaluation for this study. 17 Two independent clinicians who were blinded to the surgical technique used performed the measurements on computer-based digital radiographs on two separate occasions. Three radiographic measurements were recorded on the coronal radiographs: (1) hip–knee–ankle angle (HKA), the angle formed by the mechanical axis of the femur (line between the centre of the femoral head and the centre of the knee) and the mechanical axis of the tibia (line between the centre of the talus and the centre of the knee; Figure 1); (2) coronal femoral component angle (CFA), the angle formed by the femoral component and the mechanical axis of the femur (Figure 2); (3) coronal tibia component angle (CTA), the angle formed by the tibia baseplate and the mechanical axis of the tibia. Two radiographic measurements were recorded on the sagittal radiographs (Figure 2); (4) sagittal femoral component angle (SFA), the angle formed by the femoral component and a line perpendicular to the sagittal femoral mechanical axis (line between the centre of the femoral head and the centre of the knee; Figure 3); and (5) sagittal tibia component angle (STA), the angle formed by the tibial baseplate and a line perpendicular to the sagittal tibia mechanical axis (line between the centre of the talus and the centre of the knee; Figure 3). In the coronal plane, a varus deformity is denoted by negative value while a valgus alignment is represented by a positive value.
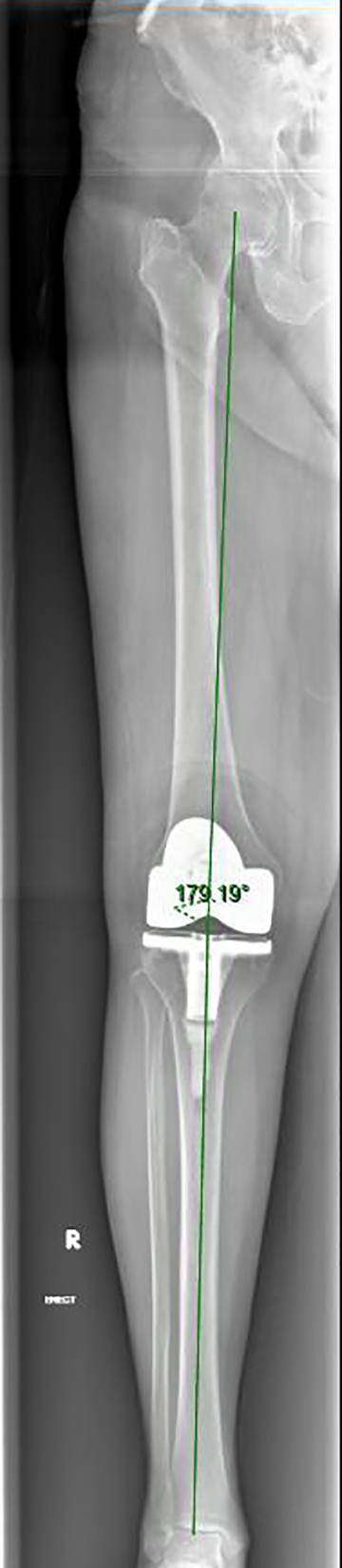
HKA measured on long leg film. HKA: hip–knee–ankle angle.
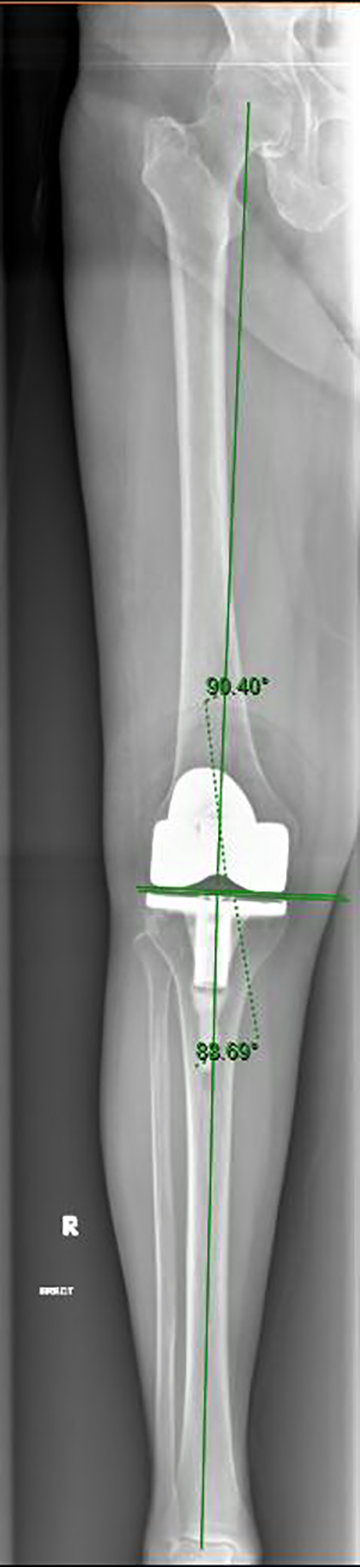
Coronal femoral component angle and coronal tibia component angle.

Lower limb sagittal view radiograph. Sagittal femoral component angle and sagittal tibia component angle.
The accepted values used in this study for normal alignment were (1) 180° ± 3° varus/valgus for HKA 18 ; (2) 90° ± 3° to the mechanical axis of the femur for CFA 18 –20 ; (3) 90° ± 3° to the mechanical axis of the tibia for CTA 18 –20 ; (4) 87° to 90° femoral flexion for SFA 20 ; 5) 83° to 90° posterior slope for STA.
Statistical analysis
Statistical analysis was carried out in consultation with the in-house biostatistician, using IBM® SPSS® 21.0 (Armonk, New York, USA). Statistical significance was defined as a p value of ≤0.05. The Mann–Whitney U test was used to compare the two groups for continuous variables while the Fisher’s Exact test was used for the analysis of categorical variables.
Results
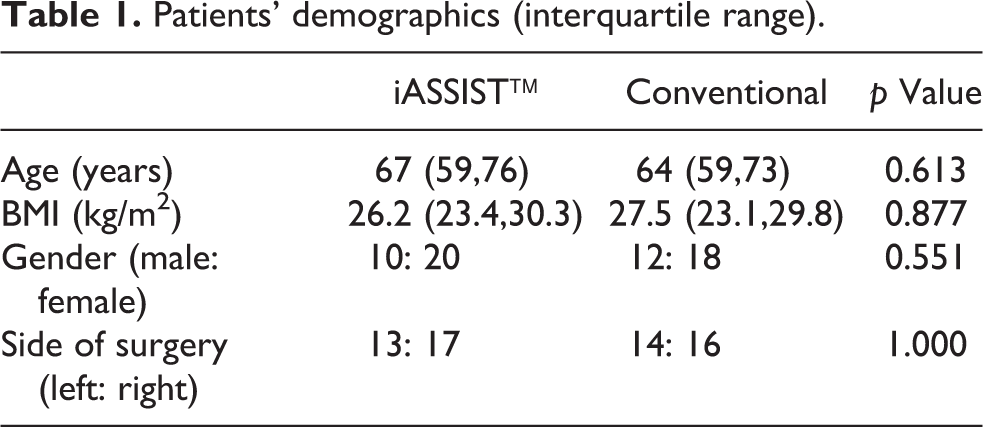
There was no difference between the two groups for age, BMI, gender and side of operated knee (p > 0.05, Table 1). Of note, there was no significant difference in preoperative mechanical axis (p = 0.471). No statistical significance was found between the control group and the navigated group pertaining to the duration of surgery, blood loss and transfusion incidence (p > 0.05). The median HKA, CFA, CTA, SFA and STA were comparable between the two groups on post-operative radiographic films (p > 0.05) (Table 2). There was no difference in the proportion of outliers for mechanical axis (p = 0.38), CFA (p = 0.50), CTA (p = 0.11), SFA (p = 0.28) and STA (p = 0.33) (Table 3). None of the patient in the iASSIST™ group developed any wound complications or major morbidity in the early post-operative period.
Patients’ demographics (interquartile range).
Perioperative outcomes (interquartile range).

Hb: haemoglobin; HKA: hip–knee–ankle angle; CFA: coronal femoral component angle; CTA: coronal tibia component angle; SFA: sagittal femoral component angle; STA: sagittal tibia component angle.
Number of outliers.

HKA: hip–knee–ankle angle; CFA: coronal femoral component angle; CTA: coronal tibia component angle; SFA: sagittal femoral component angle; STA: sagittal tibia component angle.
Discussion
Accelerometer-based navigation has been introduced as a method that is highly accurate and reproducible. The purpose of this study was to access the accuracy of lower limb alignment, femoral and tibial component placement using an accelerometer-based navigation system to perform the distal femoral and proximal tibial resections. Our study showed no improved accuracy in post-operative radiographic alignment of the implanted prosthesis and lower limb performed using iASSIST™ navigation TKA as compared with conventional TKA as judged by the number of outliers. Nonetheless, the results showed that Zimmer iASSIST navigation is as accurate as conventional method in avoiding outliers and in restoring mechanical alignment. Accelerometer-based navigation system is a useful navigation tool in TKA cases whereby the underlying patient deformity, anatomy or presence of implants precludes the use of intramedullary jigs in conventional TKA. It also eliminates additional preoperative imaging and avoids the morbidity of pin-site-related complications without significantly increasing the duration of surgery.
This result is consistent with the results of Bauwens et al.,6 Jenny et al.,13 Mielke et al.,19 and Kim et al.,20 who found no significant difference in the post-operative mechanical axis alignment of the limb between patients who underwent conventional or computer-navigated TKA. By contrast, our result was not in agreement with the findings of the many authors who have demonstrated that computer-navigated TKA is associated with more precise radiological alignment as compared to conventional TKA. 21 –23 However, computer-navigated TKA only improves limb alignment precision by a few degrees, which is within the margin of error produced by the projection-related errors in standing radiographs. 24
Recently, the long-held tenet that restoring limb alignment to within 3° from neutral mechanical axis can lead to better knee function, maximize the implant durability and decrease the risk of implant failure have been questioned. 3,25 –27 Substantial healthcare resources have been devoted to computer navigation systems and imaging-based custom patient instrumentation systems that allow surgeons to more often achieve accurate limb alignment and prosthesis placement. 6,28 The added cost of computer-assisted TKA is assumed to be subsequently balanced by a decrease in the number of revision TKA. The studies that reported post-operative malalignment predisposed to post-operative pain and poor long-term functional outcome have several limitations, including older prosthetic designs, small sample size and lack of satisfactory full-length HKA radiographs to assess overall limb alignment. 29,30 Hence, it remains controversial whether improved radiographic alignment lead to good long-term function outcome. While Huang et al. reported coronal alignment within 3° of neutral correlated with superior International Knee Society and SF-12 scores at 5 years follow-up, Spencer et al. 31 and Harvie et al. 32 concluded that there was no difference in functional outcome with computer-navigated and conventional jig-based TKR at 2 and 5 years post-operatively, respectively, despite the better alignment achieved with computer-navigated surgery. In the 15-year total knee survivorship study by Parratte et al., no difference in implant longevity was seen among patients who had neutral alignment and those with malalignment. In addition, recent research has emphasized other factors in influencing TKA outcomes and the importance of achieving coronal alignment within 3° of neutral may play at most a subordinate role. 29,30 Kim et al.20 reported no difference in clinical function or alignment and survivorship of the components between the knees that underwent computer-navigated TKA and those that underwent conventional TKA at a mean follow-up of 10.8 years in 520 patients. Authors have reported that better tribological properties, improved implant design and advancement in surgical technique have reduced negative clinical outcomes associated with prosthesis malalignment and achieving neutral coronal alignment may not necessarily reflect an ideal result for all patients. With no long-term data to support the claim that computer-navigated TKA can improves implant durability and reduces revision procedures, there is no convincing economic argument favouring computer navigation. Although the issues of desired mechanical alignment implant longevity and the inter-relationship of the two remain unknown, most authors still aim to achieve neutral mechanical axis in TKA.
The strength of our study was that the two groups had comparable demographic; surgical technique and the prosthesis used were also identical. The only difference was in the way the bone cuts were guided. Our study addressed a topic of clinical significant relevance, as there is lack of published data on the post-operative radiological outcomes of accelerator-based navigation TKR in the literature despite its widespread use in the market for the past few years. Furthermore, standardized post-operative weight-bearing long leg radiographic films are used to access the mechanical axis and implants placement. Stringent efforts were made by the authors to ensure to that films were centred and anatomic landmarks were clearly visualized to avoid measurement errors due to rotational malalignment. Positioning errors of 2° to 3° have to be acknowledged in both groups despite strict implementation of radiographic protocol.
There were several limitations to this study. Like most studies of alignment after TKA, the present study focused on the static coronal and sagittal plane alignment and did not evaluate the rotational alignment or the dynamic impact of gait on alignment. Secondly, this study did not evaluate the clinical outcomes such as the pain, range of motion, Oxford Knee Score and Short Form-36. Thirdly, due to the relatively new nature of navigation, we were limited by the small sample size and the retrospective nature of the study. This could explain the higher incidence of outlier in both the iASSIST and the conventional group. Though the use of computer-navigated TKR have been associated with steep learning curve, our study was not limited by the lack of experience to this studied iASSIST™ navigation technology. 12 The senior arthroplasty surgeon had performed more than 100 TKA with iASSIST™ navigation prior to the commencement of this study.
Conclusion
In summary, we have demonstrated that the use of Zimmer iASSIST™ navigation in TKA was safe and did not increase the duration of operation. However, our preliminary study showed that it was not better than conventional TKA in achieving satisfactory alignment and reducing outliers.
Footnotes
Authors’ note
This retrospective comparative study was studied at Changi General Hospital, Singapore.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.