
Abstract
Purpose:
Aim is to investigate the changes of mediolateral soft tissue gaps in total knee arthroplasty (TKA) after suturing medial extensor.
Methods and materials:
We compared the differences of medial and lateral gap values that were shown by the computer navigation at 0°, 45°, 90°, and 120° knee flexion during patella in situ and during patella repaired by a towel clip on two constant sites. Fifty consecutive knees (43 patients) scheduled for TKA due to varus knee osteoarthritis, from February 2017 to May 2017, were enrolled in this prospective study.
Results:
The medial gaps with patella repaired were significantly lower (p < 0.05) than the medial gaps with patella in situ at 45°, 90°, and 120° knee flexion. Differences in the medial gap were largest at 90, with the difference of 0.87 mm. Twenty-four of 50 cases (48%) showed medial gap differences of 1 mm or over, and 13 of 50 cases (26%) showed medial gap differences of 2 mm or over. The variation in the medial gap at 90° following patellar repair showed significant association (correlation coefficient = 0.78, p = 0.001) with the difference between medial and lateral gaps (medial gap − lateral gap) at 90° of patella in situ. At 90° knee flexion, when the medial and lateral gap difference in patella in situ was 1 mm or less, 73.5% (25/34) of the cases showed variation in the medial gap of less than 1 mm after patellar repair.
Conclusion:
During TKA, while measuring the medial gap with patella in situ, overestimation might occur, especially in the position of knee flexion. Thus, reevaluation using towel clips should be considered when the medial and lateral gap difference is 1 mm or larger when patella in situ during evaluation of the medial and lateral gaps at 90° knee flexion.
Introduction
Obtaining precise soft tissue balance is an essential role in total knee arthroplasty (TKA) for the function and the longevity of the implant. 1 –5 However, errors in measurement of the soft tissue balance can occur by many different factors. Especially, during conventional TKA, surgical procedures are performed after patellar eversion in order to secure a clear view during surgery. Also, the patella is mostly in the everted position when checking soft tissue tension intraoperatively. However, several authors have reported that intraoperative and postoperative soft tissue tension might differ due to the position of the patella. 6 –11 Thanks to advancements in the field of minimal invasive surgery and development of the tensors which enable measuring of the tension of the soft tissue during patellar reduction, 7,12 more precise soft tissue balancing, especially in terms of mediolateral balancing, has been enabled. However, tearing the medial extensor by medial parapatellar arthrotomy might result in different values of soft tissue balancing between intraoperative and postoperative statuses. Gejo et al. 11 have reported that increased knee flexion resulted in increased tension of the knee extensors, and as a result, as the degree of knee flexion increases, the medial soft tissue tension may be underestimated due to the torn medial extensors. Medial and lateral gap values measured at patella in situ, in which the medial soft tissue is torn due to arthrotomy, might differ from the postoperative values, in which the medial soft tissue is sutured. Besides, if the variation in such values is large, such might cause a decrease in function after surgery. However, further research is lacking in such subjects. So, we compared the differences of medial and lateral gap values which were shown by the computer navigation at 0°, 45°, 90°, and 120° during patella in situ and during patella repaired by the towel clip on two constant sites to investigate changes of mediolateral soft tissue gaps in TKA after suturing medial extensor. We have assumed that knee flexion might result in increased tension of sutured medial extensors, and thus reduce the medial gap.
Materials and methods
Study design and patients
According to the power analysis based on the results from the pilot study, the sample size showing power of 0.9 (p = 0.05) with 1 mm difference in medial gaps was estimated to be 20. Since the error in gap measurement of the computer navigation system has been known to be less than 1 mm by preceding research studies, we defined the difference of 1 mm or larger as a meaningful difference. 13,14 We estimated that 50 cases would need to be enrolled to show a normal distribution. After the approval of the institutional review board (CR-17-036-L), 50 consecutive knees (43 patients) scheduled for TKA due to varus knee osteoarthritis, from February 2017 to May 2017, were enrolled in this prospective study. Inclusion criteria were pain unresponsive to medications and loss of function due to varus knee osteoarthritis. Exclusion criteria were history of knee surgeries, genu valgum deformity arthritis, infection, and revision TKA (Figure 1). A total of 43 patients (7 men and 36 women) were enrolled. The patients’ average age was 69.64 ± 6.13 years. Mean preoperative mechanical hip–knee–ankle angle value was 168.58 ± 6.54°.

Flowchart for enrollment for study.
Surgical technique and measurements
All surgeries were performed by one surgeon in the same medical center. All surgeries were performed using a posterior stabilized (PS) type of PFC (DePuy, Warsaw, Indiana, USA) with the assistance of imageless computer navigations of BrainLAB system (BrainLAB, Feldkirchen, Germany). All knees were exposed by a standard medial parapatellar approach. Cemented PS implants were inserted in all patients. None of the patients underwent patellar resurfacing. After the cut was made to the femoral side under guidance of the computer navigation, an additional tibial cut was made perpendicular to the mechanical axis using a cutting block under navigation guidance. The completion of bone cutting was followed by medial release of the superficial medial collateral ligament and removal of residual osteophytes from the medial femoral condyle and the medial tibial plateau in a step-by-step fashion, until the mechanical axis of the limb achieved in the extended position showed a mediolateral gap difference of less than 3 mm on the navigation. After insertion of the trial implant including liners was done, the coronal alignment, the medial and lateral gaps were checked in the 0° and 90° knee flexion through the navigation screen. If the coronal alignment was between 0° and 3° from the mechanical axis and the mediolateral gap difference was less than 3 mm in the 0° and 90° knee flexion through the navigation screen, real prostheses were inserted to the knees. After insertion of all the real implants including plastic liners was completed, the medial and lateral gap values were measured under navigation guidance at 0°, 45°, 90°, and 120° knee flexion with patella in situ (injured medial extensor; Figure 2). The computer navigation system displays the gap values in 0.5 mm increments. Also, after applying towel clips to the upper pole’s curved incision site and lower pole’s curved incision site of arthrotomy for medial extensor tissue repairing (repaired medial extensor; Figure 3), the gap values were also measured. Mediolateral soft tissue tensioning during TKA has been measured in various ways, such as subjective feelings of the surgeon, based on operator’s experience, by spacer bars, tensors, electric instruments, or by computer navigation. 3,15 –17 After the real implant was applied to the knee, the gap values could be measured by computer navigation. When checking the gap values using navigation, the knee was allowed to dangle freely and tourniquet was deflated. Matsumoto et al. 7 showed that during TKA, the gap values obtained by the tensors, which were able to measure soft tissue balancing in a reduced patellar position, were similar to the values measured by the computer navigation (BrainLAB) which we used in our medical center.

After insertion of all the real implants, medial and lateral gap values were checked under navigation guidance, at 0° (a), 45°, 90° (b), and 120° knee flexion.

We replaced the process of medial extensor repair with towel clip applying to constant area.
Statistical analysis
Statistical analysis was performed using IBM SPSS Statistics, version 19, software (IBM Corporation, Armonk, N.Y., USA). A paired t test was used to compare the average value of two groups in parametric values. The Mann–Whitney test was used to compare the average value of two groups in nonparametric values. p Values of 0.05 or below were considered to indicate statistical significance. Spearman’s test was used to measure the extent of association between the factors. All data are presented as means and standard deviations. G*Power 3.1 software was used for power analysis.
Results
The medial gaps with patella in situ at 0°, 45°, 90°, and 120° flexion were 12.90 ± 1.87 mm, 13.87 ± 2.20 mm, 14.04 ± 2.67 mm, and 14.21 ± 2.79 mm, respectively. The lateral gaps with patella in situ at 0°, 45°, 90°, and 120° flexion were 13.04 ± 1.96 mm, 13.21 ± 1.97 mm, 13.04 ± 2.30 mm, and 13.23 ± 2.30 mm, respectively. The medial gaps with patella repaired by the towel clip at 0°, 45°, 90°, and 120° flexion were 12.86 ± 1.91 mm, 13.59 ± 2.02 mm, 13.17 ± 2.27 mm, and 13.62 ± 2.61 mm, respectively. The lateral gaps with patella repaired by the towel clip at 0°, 45°, 90°, and 120° flexion were 13.06 ± 1.82 mm, 13.05 ± 1.89 mm, 12.82 ± 2.25 mm, and 13.26 ± 2.39 mm, respectively. The medial gaps with patella repaired by the towel clip were significantly lower (p < 0.05) than the medial gaps with patella in situ at 45°, 90°, and 120° flexion (Figure 4). We calculated that the total of 50 cases would provide 90% power to detect the variation in the medial gap. The lateral gap with patella repaired by towel clips showed significantly lower (p = 0.01) values than the lateral gap with patella in situ at 90° flexion.

The medial gaps with patella repaired by the towel clip were significantly lower (p < 0.05) than the medial gaps with patella in situ at 45°, 90°, and 120° flexion.
The medial gaps with patella repaired by the towel clip were significantly lower (p < 0.05) than the medial gaps with patella in situ at 45°, 90°, and 120° knee flexion. Differences in the medial gap were largest at 90° flexion, with the difference of 0.87 mm. Twenty-four of 50 cases (48%) showed medial gap differences of 1 mm or over, and 13 of 50 cases (26%) showed medial gap differences of 2 mm or over. The variation in the medial gap at 90° knee flexion following patellar repair showed significant association (correlation coefficient = 0.78, p = 0.001) with the difference between medial and lateral gaps (medial gap − lateral gap) at 90° knee flexion when patella in situ. At 90° knee flexion, when the medial and lateral gap difference was less than 1 mm, 73.5% of the cases (25/34) showed a variation in the medial gap of less than 1 mm after patellar repair.
Discussion
The changes in soft tissue gaps depending on the position of the patella (reduction or eversion), especially in the medial and lateral gaps, still remain controversial. In a cadaveric study, Gejo et al. 10 reported that during patellar eversion, the lateral gap was smaller than the lateral gap during patellar reduction at flexion and extension of the knees. Lateral shift and external rotation of the tibia during patellar eversion were assumed to be the cause of the result. However, a clinical trial by Matsumoto et al. and Yoshino et al. showed that the flexion gap during patellar reduction was decreased than the flexion gap during patellar eversion. 7,9 Moreover, Matsumoto et al. reported that during patellar reduction, besides the gap decrease at 90° flexion, a slight valgus ligament balance was observed. They assumed that during patellar reduction, anterolateral structures of the knee, including the iliotibial band and the extensor mechanism, showed a significant shift of tension anteriorly and laterally. So, they insisted that postoperative soft tissue imbalance due to intraoperative overestimation of the soft tissue balancing parameters might occur when the patella is everted during surgery.
In this study, we did not examine the changes in the mediolateral gaps during patellar eversion. Nowadays, with advancements in the field of minimal invasive surgery and development of tensors which enable measuring of the tension of the soft tissue, the surgeon does not need to evert patellar tissue during gap balancing in TKA. However, comparative studies for the effects of injured medial extensor by median parapatellar approach on mediolateral soft tissue tension in TKA (in situ vs. repaired) are lacking in numbers. In a cadaveric study by Gejo et al., 10 patients were assigned to three groups: patellar eversion, patellar reduction (in situ), and patellar repair with multiple sutures. Compared with the other two groups, medial and lateral gaps of the patellar eversion group differed by the strain of the quadriceps. The medial gaps of the patellar eversion group at 90° flexion of the knee were significantly lower than the other groups under the strain of the quadriceps from 25 N to 75 N. However, compared to the patellar repair group, the medial gaps of the patellar eversion group were significantly higher under the strain of 125 N. There were no significant differences in the medial and lateral gaps between the patellar reduction group and the patellar repair group at knee extension. Compared to the patellar repair group, the lateral gaps were significantly lower in the patellar reduction group at knee flexion (90°). These results were thought to be caused by strain relatively focused on the lateral extensor tissues, due to the medial tissue tear which occurred during medial arthrotomy. Senavongse et al. 18 compared the strain of the extensor tissues of the knee and reported that the lateral aspect possessed tighter strain than the medial aspect. However, in this study, the medial gap values with patella repaired by the towel clip were significantly lower than the values with patellar reduction at 45°, 90°, and 120° flexion of the knee. Medial gap difference was highest at 90° flexion, with an average value of 0.87 ± 1.31 mm (Figure 5). We assumed that the strain of repaired medial extensor made the medial gap smaller compared to patella in situ. The strain of recovered medial extensor might be largest at 90° knee flexion. Further evaluation to measure the strains of recovered medial extensor tissue by repair needs to be done later. There may be less reliability since the results are within the general error range, which is 1 mm or less. However, analysis of the distribution of the values showed that gap differences of more than 1 mm, which surpass the margin of error, occurred in 48% of the cases, and gap differences of more than 2 mm, which is a value that might cause a postoperative decrease in function, 7,11 occurred in 26% of the cases. The variation in the medial gap at 90° knee flexion following patellar repair showed significant association (correlation coefficient = 0.78, p = 0.00) with the difference between medial and lateral gaps (medial gap − lateral gap) at 90° knee flexion and patella in situ. At 90° knee flexion, when the medial and lateral gap difference was less than 1 mm, 73.5% of the cases (25/34) showed a variation in the medial gap of less than 1 mm after patellar repair. However, when the medial and lateral gap difference was 1 mm or larger, 75% of the cases (12/16) showed a variation in the medial gap of over 2 mm after patellar repair.
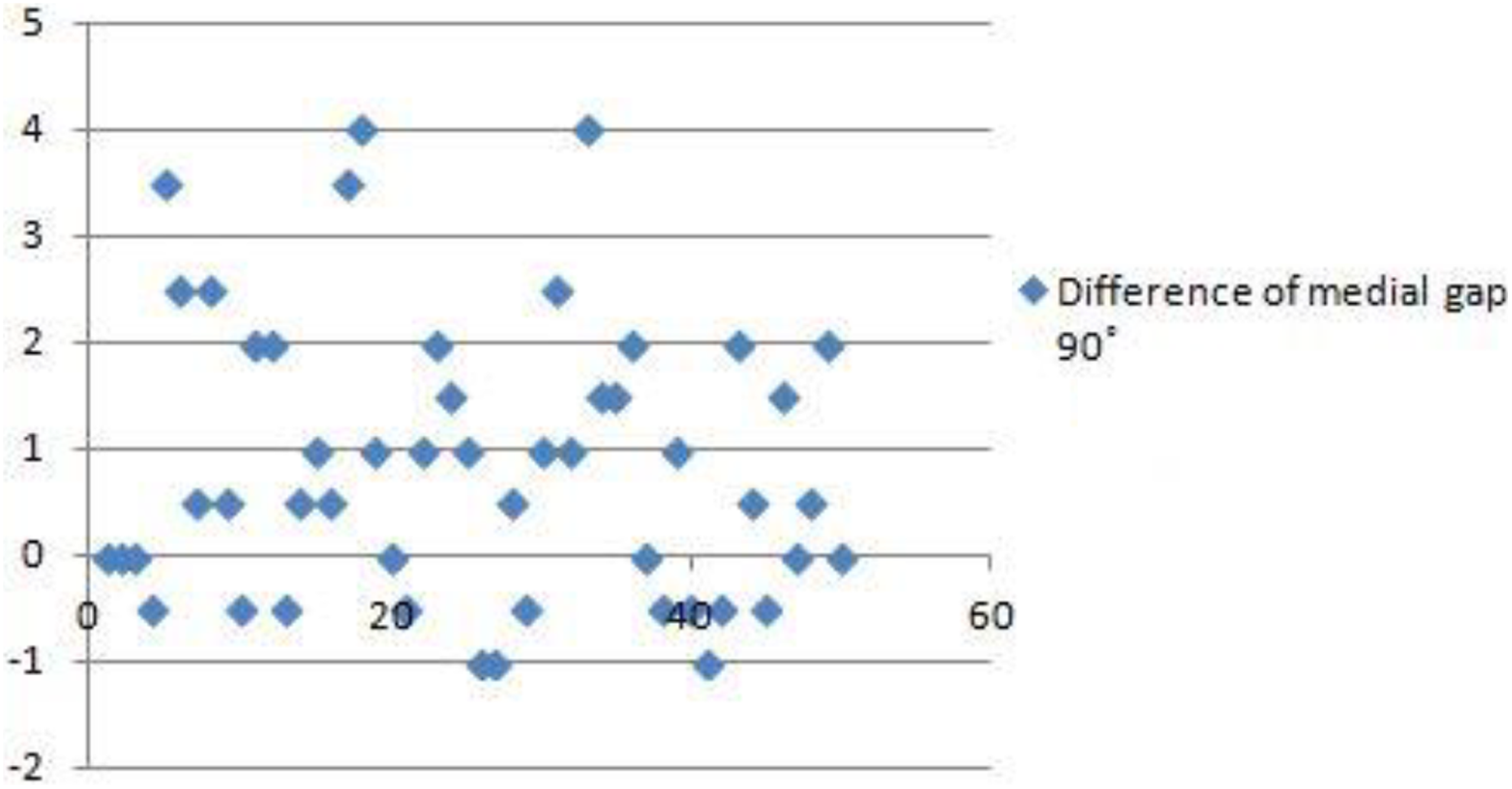
Medial gap difference was highest at 90° flexion, with an average value of 0.87 ± 1.31 mm.
In few cases, at knee flexion, differences of mediolateral gap values were 3 mm or more when measured in situ, but showed proper mediolateral gap balancing when the towel clip was applied (Figure 6). Based on this result, during evaluation of the medial and lateral gaps at 90° knee flexion, reevaluation using towel clips should be considered when the medial and lateral gap difference in patella in situ is 1 mm or larger.

In few cases, at knee flexion, differences of mediolateral gap values were 3 mm or more when measured in situ (a), but showed proper mediolateral gap balancing when the towel clip was applied (b).
Our study has several potential limitations. First, the gap values were measured by computer navigation. In order to reflect post-TKA soft tissue strain, we tried to measure the gaps after the insertion of the real prosthesis was done. Measurement after the insertion of the real prosthesis could reduce errors owing to creep elongation of the surrounding tissues and was assumed to provide more accuracy. Such means of measurement can only be done by computer navigation. According to Matsumoto et al., the gap values measured with the tensors were similar to the gap values measured by the same computer navigation that we have used in this study. Values were similar especially during patellar reduction and with flexion of the knee. Second, the difference was 0.87 ± 1.31 mm at 90° flexion. However, this can be within the margin of error of the computer navigation. Consequently, additional studies with a larger sample size are needed to determine the clinical significance of such differences. Third, we replaced the process of medial extensor repair with towel clips. When compared with tissue suture, towel clips applied to the upper and lower poles of the patella during surgery may show reduced recovery.
Conclusion
During TKA, while measuring the medial gap with patella in situ, overestimation might occur, especially in the position of knee flexion. In conclusion, during evaluation of the medial and lateral gaps at 90° knee flexion and patella in situ, reevaluation using towel clips should be considered when the medial and lateral gap difference is 1 mm or larger.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.