
Abstract
Purpose:
We have analyzed the surgical outcomes of primary total knee arthroplasty (TKA) using computer-assisted navigation that were performed by a single surgeon in terms of postoperative coronal alignment depending on preoperative varus deformity.
Methods:
We conducted a retrospective study of patients who have undergone navigated primary TKA from January 2016 through December 2019. Two hundred and fifty-six cases with varus deformity of 10° or less were assigned to group 1, and 216 cases with varus deformity of more than 10° were assigned to group 2. The postoperative mechanical hip–knee–ankle (mHKA) angle was measured from scanograms which were taken preoperatively and 3 months after surgery. The postoperative mHKA angle was targeted to be 0°, and the appropriate range of coronal alignment was set as 0 ± 3°.
Results:
The Pearson correlation showed a significant correlation with the degree of preoperative varus deformity and with the absolute error of postoperative mHKA (p = 0.01). Among all patients, 64 cases (13.6%) were detected as outliers (mHKA > 0° ± 3°) at 3 months after surgery. Of the 64 cases, 25 cases (9.8%) were affiliated to group 1 and 39 cases (18.1%) were affiliated to group 2. Group 2 showed significantly higher occurrence of outliers than group 1 (p = 0.01). Multiple variables logistic regression analysis, which analyzed the difference in the occurrence rate of outliers (mHKA > 0° ± 3°), showed that the occurrence rate of group 2 was 2.04 times higher than group 1. After adjusting for patient’s age, gender, and body mass index, the occurrence rate of outliers in group 2 was 2.01 times higher than group 1.
Conclusion:
The benefit of computer-assisted navigation during TKA in obtaining coronal alignment within 0 ± 3° may be lessened when the preoperative varus deformity is severely advanced.
Introduction
According to Fang et al., 1 postoperative coronal alignment is one of the major factors influencing total knee implant survival. Upon such understandings, computer-assisted navigation has been introduced and shown to be more effective than conventional (manual) total knee arthroplasty (TKA) in obtaining the generally accepted proper coronal alignment (0 ± 3° of mechanical hip–knee–ankle (mHKA) angle). 2 –4 One of the benefits of computer-assisted total knee arthroplasty (CA-TKA) is that it allows real-time assessment of the alignment during surgery, thus allowing precise bone cutting and adequate degree of soft tissue releasing. 5 However, the risk of registration errors, and the consequential malalignment is thought to be a great drawback of CA-TKA. 6,7 Especially registration may be inaccurate in patients with advanced osteoarthritis (OA) due to ambiguous bony markers. 8 As a result, the alignment error in the coronal plane may be higher than patients with less bony deformity. However, research on such alignment error is lacking.
We have analyzed the surgical outcomes of TKA performed by a single surgeon, which mostly used computer-assisted navigation in primary TKA cases, in terms of postoperative coronal alignment depending on preoperative varus deformity.
The study plan was based on the hypothesis that a higher degree of preoperative varus deformity in the knee joint would result in higher postoperative coronal plain alignment error, and higher occurrence rate of outliers. We have tried to target the postoperative mHKA angle to be 0° and have set the appropriate range of coronal alignment as 0° ± 3°.
Methods
Patients
We conducted a retrospective study of patients who have undergone primary TKA by a single surgeon in our hospital from January 2016 to December 2019. The single surgeon is an expert in CA-TKA. He had been performing CA-TKA since 2008 and have performed CA-TKA in most of the cases of primary TKA since 2015. From January 2016 to December 2019, the surgeon has performed 563 cases of primary TKA. The primary reason for surgery was knee OA (512 cases). Exclusion criteria were valgus deformity (29 cases), intraoperative change of procedure from CA-TKA to manual TKA (3 cases), and inappropriate preoperative or postoperative scanogram (8 cases). A total of 472 cases were enrolled to this study.
According to the degree of varus deformity, 256 cases with varus deformity of 10° or less were assigned to group 1, and 216 cases with varus deformity of more than 10° were assigned to group 2 (Table 1). Analyses on the degree of difference between the target mHKA angle (0°) and the postoperative mHKA angle and on the occurrence rate of outliers were performed. This trial was conducted after approval of the Daegu Catholic University Medical Center (DCUMC) Institutional Review Board (approval number: CR-20-070).
Epidemiology of all participants.

n: numbers; F: female; M: male; mHKA: mechanical hip–knee–ankle.
Surgical methods
Tourniquets were applied in all operations. Midline skin incision and the medial parapatellar approach were applied in all the cases. The imageless navigation system version 2.6 (BrainLAB, Feldkirchen, Germany) was used in all navigation cases. Measured gap technique was used for bone resections. Both femoral and tibial components were fixed with bone cement. Cementation of both femur and tibia was done at once using Depuy CMW 3 (DePuy International Limited T/A DePuy CMW Cornford Road Blackpool Lancashire FY4 4QQ UK) bone cement. Posterior cruciate-substituting (PS) type of implant was used for all TKA.
Outcome measurement
The mHKA angle was measured by an orthopedic surgeon who was not involved in this study, using two scanograms taken preoperatively and 3 months after surgery. Scanograms were taken with both legs under weight. The postoperative mHKA angle was targeted to be 0°, and the appropriate range of coronal alignment was set as 0 ± 3°.
Statistical analysis
All analyses were performed with IBM SPSS version 19.0 software (SPSS Inc., Chicago, Illinois, USA) for Windows. The χ 2 test and t-test were used to identify the differences in errors and outliers of mHKA. The χ 2 test was used to identify the difference in outliers of mHKA, and the t-test was used to determine the difference in errors of mHKA. The Pearson correlation coefficient was used to identify the association between the degree of preoperative varus deformity and the absolute error of postoperative mHKA. The value of p ≤ 0.05 was considered to be statistically significant.
Results
Absolute errors of coronal alignment (mHKA angle)
Among the 472 cases who met the inclusion and exclusion criteria, the absolute error of mHKA measured 3 months after surgery was 1.77 ± 1.29° in average. The mean values were 1.64 ± 1.23° in group 1 and 1.92 ± 1.34° in group 2. The absolute error of postoperative coronal alignment was significantly higher in group 2 than in group 1 (p = 0.02).
Correlation between the preoperative varus deformity and the absolute error of postoperative coronal alignment error
The Pearson correlation test showed a significant correlation between the degree of preoperative varus deformity and the absolute error of postoperative mHKA (p = 0.01).
Outliers of coronal alignment
Among all patients, 64 cases (13.6%) were detected as outliers (mHKA > 0± 3°) at 3 months after surgery. O which, 25 cases (9.8%) were affiliated to group 1 and 39 cases (18.1%) were affiliated to group 2. Group 2 showed significantly higher occurrence of outliers than group 1 (p = 0.01, Table 2).
A χ 2 test to identify the difference in outliers (mHKA > 0 ± 3°).a
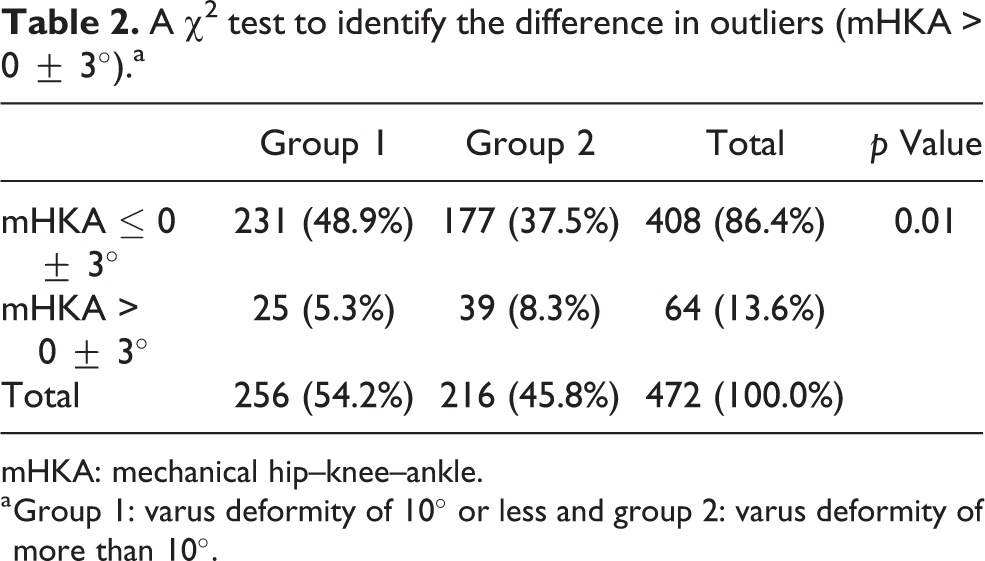
mHKA: mechanical hip–knee–ankle.
a Group 1: varus deformity of 10° or less and group 2: varus deformity of more than 10°.
Among all patients, 35 cases (7.4%) were detected as outliers (mHKA > 0 ± 4°) at 3 months after surgery. O which, 12 cases (4.7%) were affiliated to group 1 and 23 cases (10.6%) were affiliated to group 2. Group 2 showed significantly higher occurrence of outliers than group 1 (p = 0.01).
Logistic regression analysis in difference in outliers of coronal alignment (mHKA > 0 ± 3°)
Multiple variables logistic regression analysis, which analyzed the difference in the occurrence rate of outliers (mHKA > 0 ± 3°), showed occurrence rate in group 2 to be 2.04 times higher than group 1. After adjusting for patient’s age, gender, and body mass index, the occurrence rate of outliers in group 2 was 2.01 times higher than group 1 (Table 3).
Multiple variables logistic regression analysis, which analyzed the difference in outliers (mHKA > 0° ± 3°).a

OR: odds ratio; CI: confidence interval; G1: group 1; G2: group 2.
a Group 1: varus deformity of 10° or less and group 2: varus deformity of more than 10°.
b Adjusted by age, gender, and body mass index.
Discussion
TKA is currently being performed to a relatively younger population, 9 and obtaining the coronal alignment of 0 ± 3° is important for implant survival. 10,11 On such basis, the technique of computer-assisted navigation has been integrated to TKA and have been reported to be effective in obtaining the coronal alignment of 0 ± 3°. 12 –14 However, the fact that obtaining coronal alignment of 0 ± 3° in all types of cases, regardless of cases with severe varus deformity, is questionable. 14 Sorrells et al. 15 have reported that the presence of severe preoperative deformity before manual TKA may be a risk factor for shorter implant survival due to lower probability to achieve neutral alignment postoperatively. However, research on data of CA-TKA was lacking.
In this study, we have identified the association between the severity of preoperative varus deformity and the error in coronal alignment after CA-TKA. Especially the occurrence rate of outliers, which was out of the mHKA angle tolerance range of 0 ± 3°, was 2.01 times higher when patients had varus deformity of over 10°. The benefit of computer-assisted navigation may be lessened when varus deformity is severe. We assume this is due to inaccurate registration of the bony landmarks. Katz et al. 8 have reported that increased varus deformity results in increased deformity of the femoral epicondyle (especially the medial epicondyle) and may trigger decreased accuracy of the transepicondylar axis, which is one of the methods in determining femoral rotation.
In this study, difference in postoperative mHKA between group 1 and group 2 was statistically significant, but the difference is 0.28° in average. Since the error during computer-assisted navigation may be high as up to 1°, 16 such difference may be meaningless. However, with respect to the occurrence rate of mHKA outliers (mHKA > 0 ± 3°), group 2 showed significantly higher rates than group 1. Also, when the mHKA outliers were defined as 0 ± 4°, group 2 showed significantly higher rates than group 1. According to these values, we have identified that preoperative advanced varus deformity may decrease the efficacy of CA-TKA.
Limitations of this study include its retrospective study design. However, since only eight cases (1.66%) were excluded due to inappropriate data settings, the selection bias may not be significant. Secondly, since the measurement of mHKA angle values using long films are more accurate than using short films, 17 we have conducted this study with only the data collected from 2016, when both preoperative and postoperative scanograms were taken using long films.
Conclusion
The benefit of computer-assisted navigation during TKA in obtaining coronal alignment within 0 ± 3° may be lessened when the preoperative varus deformity is severely advanced.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.