
Abstract
Background:
A device that can measure posture alignment repeatedly is important for the prevention of hyperkyphosis.
Objective:
We devised a markerless measurement method for hyperkyphosis using digital photography and investigated the correlation with other noninvasive measurements and the validity and accuracy of this method.
Methods:
The study included 27 participants. The craniovertebral angle in supine (CVAS) and craniohorizontal angle in supine (CHAS) were calculated from digital photographs of the head and neck areas of the studied subjects with ImageJ. The correlations of CVAS and CHAS with the kyphosis index (KI) and block method (BM) were investigated. Intrarater correlation coefficient and Bland–Altman analyses were used to verify the reliability and accuracy of the measured results.
Results:
CHAS exhibited an excellent correlation with the KI and the BM. The intra- and interrater reliabilities of CHAS were almost perfect. Bland–Altman analysis revealed that CHAS was associated with minor addition errors.
Conclusion:
CHAS founded an excellent correlation and reliability with the conventional spinal postural alignment measurements. The addition error suggested that the manual was needed to confirm the landmark. The CHAS is a method used to measure the spinal postural alignment in a supine position without markers and without exposing the skin surface.
Keywords
Introduction
Age-related postural hyperkyphosis is an exaggerated anterior curvature of the midthoracic spine. It is often referred to as the Dowager’s hump or strange deformity, has a prevalence of 20–40%, and is more common in the geriatric population. 1,2 Hyperkyphosis leads to worsened gait patterns and balance, lowers Activity of Daily Living (ADL), and causes a decline in lung function. 3 –6
Given that age-related spinal postural alignment abnormalities, including hyperkyphosis, progress temporally, it is important to measure the posture repeatedly and provide preventive and appropriate intervention guidance. In Japan, the aging population is increasing rapidly, and extending healthy life expectancy is important. Therefore, devices for repeated measuring of the posture of elderly people are required. It is desirable to implement a simple device with a high service capacity for the effective identification of patients at risk, including intervention and frequent follow-up, thus reducing the healthcare burden.
To date, the devices that can measure posture regularly for the prevention of hyperkyphosis include the Cobb angle of kyphosis that is based on X-ray imaging, Spinal Mouse, kyphosis index (KI), and the block method (BM). The Cobb angle is the most objective measurement method that captures the curvature based on the difference between the inclinations of the two terminal vertebrae. 7 However, Cobb angle measurements cannot be performed regularly because (a) the patients are exposed to radiation and (b) the cost of examination is relatively high. Noninvasive measurement methods, such as the Spinal Mouse and KI, are alternatives to the Cobb angle, and many published reports have documented the existence of increased correlations of their outcomes with those of the Cobb angle. 8 –11 However, the Spinal Mouse requires expensive equipment and the exposure of the skin of the upper body for measurements. Moreover, given that KI also requires exposure of the skin surface at the time of measurement, currently, no tool is easy to use for local residents. The BM is a noninvasive measurement method that is inexpensive and does not require skin exposure. However, it is not possible to identify slight changes in the subject’s posture because of the number of 1.7 cm blocks. 4,12
Therefore, we have devised a method to measure the spinal postural alignment using image processing software with ImageJ (version 1.52, National Institutes of Health, Bethesda, Maryland, USA). A posture measurement method using digital images has already been reported, but it is unsuitable for use in the community because it requires exposure of the skin to expose the landmarks. 13 –15 Our proposed method can be used in the supine position, it does not require the removal of clothing, and it is thus applicable and useful for frail elderly people whose standing is unstable. Therefore, it is assumed that our method can be easily used.
The purposes of this study are (1) to devise a measurement method for sagittal spinal postural alignment using markerless digital images, (2) to verify the correlation with other noninvasive measurement methods and quantify the reliability of this measurement method, and (3) to verify the accuracy of this measurement method using Bland–Altman analyses.
Materials and methods
Participants
The subjects were 27 elderly patients (5 males, 22 females, average age 85.3 ± 7.0 years) who were enrolled in a healthcare facility for the elderly. Those who could not measure KI due to standing difficulties and those with severe dementia were excluded. Examiners were two physiotherapists with multiple years of experience (Examiner A: 17 years and Examiner B: 2 years) who worked in the hospital. All participants provided informed consent, and the study was approved by our institutional ethics review board (approval number: OKRU19-A011). This study conforms to the Declaration of Helsinki.
Measurement methods
Spinal postural alignment measurement using digital photography
The subjects were asked to assume a supine position with the occipital region in contact with the surface of the bed. We instructed the subjects the following: “do not move the chin or the neck,” “keep your eyes on the ceiling in the room,” and “relax and keep your eyes on the ceiling.” A digital camera (PowerShot SX740 HS, Canon Co. Ltd) was placed 1 m away from the edge of the bed and was adjusted to a height that was parallel to the bed surface. The resolution of the camera was 1824 × 1824 pixels. The center of the lens of the digital camera was aligned with the right shoulder joint of the subject (Figure 1). The operator confirmed that the ears were exposed at the time of photography. Therefore, if the ears were covered with hair, the operator moved them so that the ears were exposed.

(a and b) Layout of the digital imaging acquisition setup.
The digital images were loaded into a personal computer, and the orientation of the spine was calculated with the angle measurement tool of ImageJ (PowerShot SX740HS,Canon Co. Ltd, Tokyo, Japan). According to previous studies, ImageJ has been measured for posture assessment, wheelchair sitting posture, and brow position measurements. 16 –18
To measure the degree of sagittal spinal postural alignment, the craniovertebral angle in supine (CVAS) and craniohorizontal angle in supine (CHAS) biomarkers were calculated from the images acquired in ImageJ. Previous studies have reported that standing CVA is an index of the anterior tilt of the head, and standing CHA reflects the position and visual field of the upper cervical spine that are associated with good intra- and interrater reliability in standing measurements (Figure 2). 14 We decided to apply these parameters to supine position measurements. The CVAS was formed at the intersection of the horizontal line, which passed through the back and the line, which joined the tragus of the ear and the back. CHAS was formed at the intersection of the horizontal line, which passed through the tragus of the ear and the line, which joined the tragus of the ear and the external canthus of the eye (Figure 3).
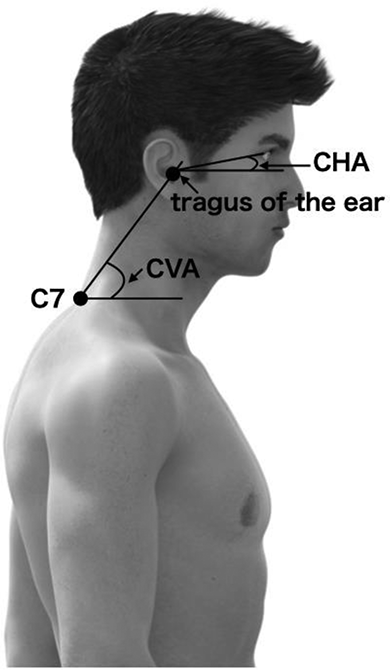
Conventional measurements of CVA and CHA. CVA: craniovertebral angle; CHA: craniohorizontal angle.
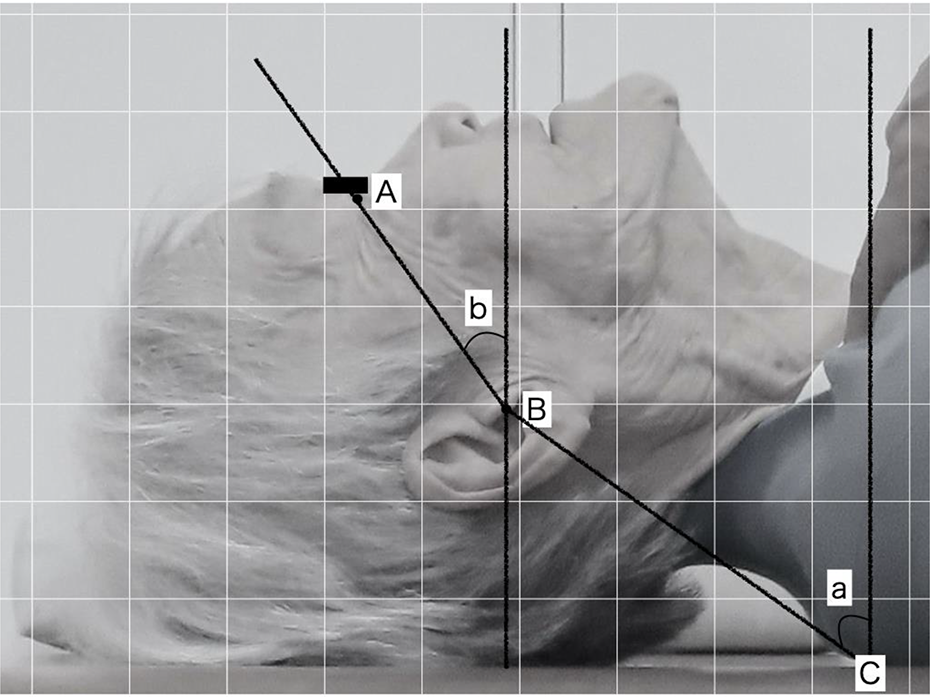
Methodology used to measure CVAS and CHAS (A: lateral canthus, B: tragus, C: contact between back and back; a: CVAS, b: CHAS). CVAS: craniovertebral angle in supine; CHAS: craniohorizontal angle in supine.
Conventional noninvasive spinal postural alignment
For comparison, the spinal postural alignment was measured with the conventional method. KI was measured with a flexible curve ruler (60cm curve ruler, Shinwa Rules Co., Ltd. Niigata) based on the method of Milne and Lauder. 9 The location on the ruler that was level with the lumbosacral joint was marked, and the curve was traced onto a graph paper. A straight line was then drawn from the level of C7 to L4. The KI was represented as multiplication by 100 of the ratio of the height of the thoracic curve and the spinal length. Higher KI values indicated greater kyphosis. Spinal postural alignment with BM was measured according to the method of Kado et al. 12 The subject laid in a supine position, and 1.7 cm wooden blocks were stacked until the head and neck were parallel. The number of blocks was used as the final outcome. 4
Statistical analysis
The correlations with CVAS, CHAS, and KI were investigated using the Pearson product-moment correlation coefficient. The relationship between CVAS, CHAS, and BM was investigated using the Spearman’s rank correlation coefficient. Subsequently, for the parameters that significantly correlated with CVAS and CHAS, the standard error and 95% confidence intervals (CIs) were determined, and the Intraclass correlation coefficient were calculated to assess interrrater (ICC 1.1) and intrarater reliability (ICC 2.1).
Bland–Altman plots were used to confirm the agreement between intra- and interrater measurements. 19 In the Bland–Altman analyses, we investigated the systematic errors of fixed bias and percentage error. The fixed bias calculates the 95% CI of the average of the differences between the measured values. If this interval does not include zero values, it is considered to be a fixed error. For the percentage error, we calculated the Pearson product-moment correlation coefficient by the Bland–Altman plot and judged that there was a proportional error when a significant correlation was found. To examine whether the measurement error was within the clinically applicable range, we determined the “limit of agreement (LOA),” which is the permissible range of errors between the two measurement values. In this study, [(d− − 1.96 s) + tSELOA] – [(d− + 1.96 s) − tSELOA] were used as LOA CIs. SPSS (version 26.0, IBM, New York City, New York, USA) was used for statistical analyses, and the significance level was set to 5%.
Results
Table 1 lists the measurement results of demographic data and the kyphosis values of the subjects. Table 2 lists the correlations among all the measurements. The correlation coefficient between the first and second measurements of KI and CVAS did not significantly correlate (either in the case of examiner A or in the case of examiner B). The correlation coefficients between the first and second measurements of BM and CVAS did not significantly correlate in the cases of examiners A and B. The correlation coefficients between the first and second measurements of KI and CHAS were 0.81 and 0.81 for examiner A and 0.85 and 0.84 for examiner B. The correlation coefficients between the first and second measurements of the BM and CHAS were 0.81 and 0.81 for examiner A and 0.80 and 0.79 for examiner B. Therefore, reliability was verified using only CHAS.
Characteristics of subjects.

KI: kyphosis index; BM: block method; CVAS: cranio-vertebral angle in supine; CHAS: cranio-horizontal angle in supine.
Relationship between CVAS, CHAS, and KI and BM.
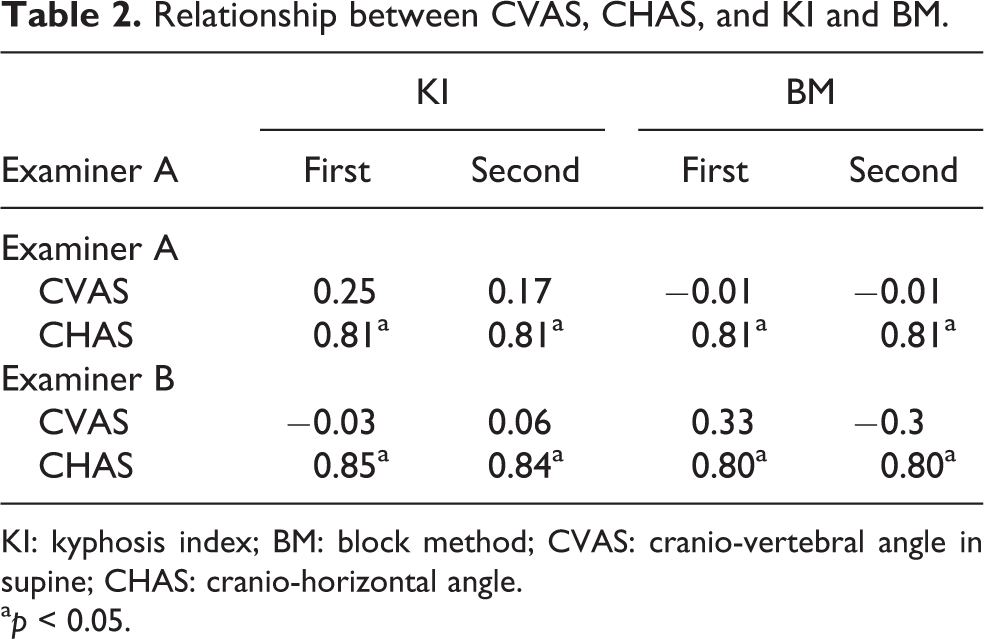
KI: kyphosis index; BM: block method; CVAS: cranio-vertebral angle in supine; CHAS: cranio-horizontal angle.
a p < 0.05.
CHAS values equaled 28.6 ± 11.3° and 28.7 ± 11.1° in the cases of the first measurements conducted by examiners A and B, respectively, and 29.1 ± 11.3° and 28.9 ± 11.3° in the second measurements. Regarding the intrarater reliability of CHAS, the ICC (1, 1) values were 0.99 and 0.99 for examiners A and B, respectively (Table 3). Bland–Altman analyses for CHAS showed that both examiners A and B yielded good reliabilities, but there was a fixed bias in the case of examiner A. Examiner B did not yield any errors (Table 4 and Figure 4). The LOA ranged from −2.3° to 1.3° in the case of examiner A, and from −2.2° to 1.7° in the case of examiner B (Table 4).
Intraclass correlation coefficient (ICC) of CHAS.

CHAS: craniohorizontal angle in supine; CI: confidence interval.
a p < 0.05.
Bland–Altman analysis of measurement error.

LOA: limits of agreement; CI: confidence interval.
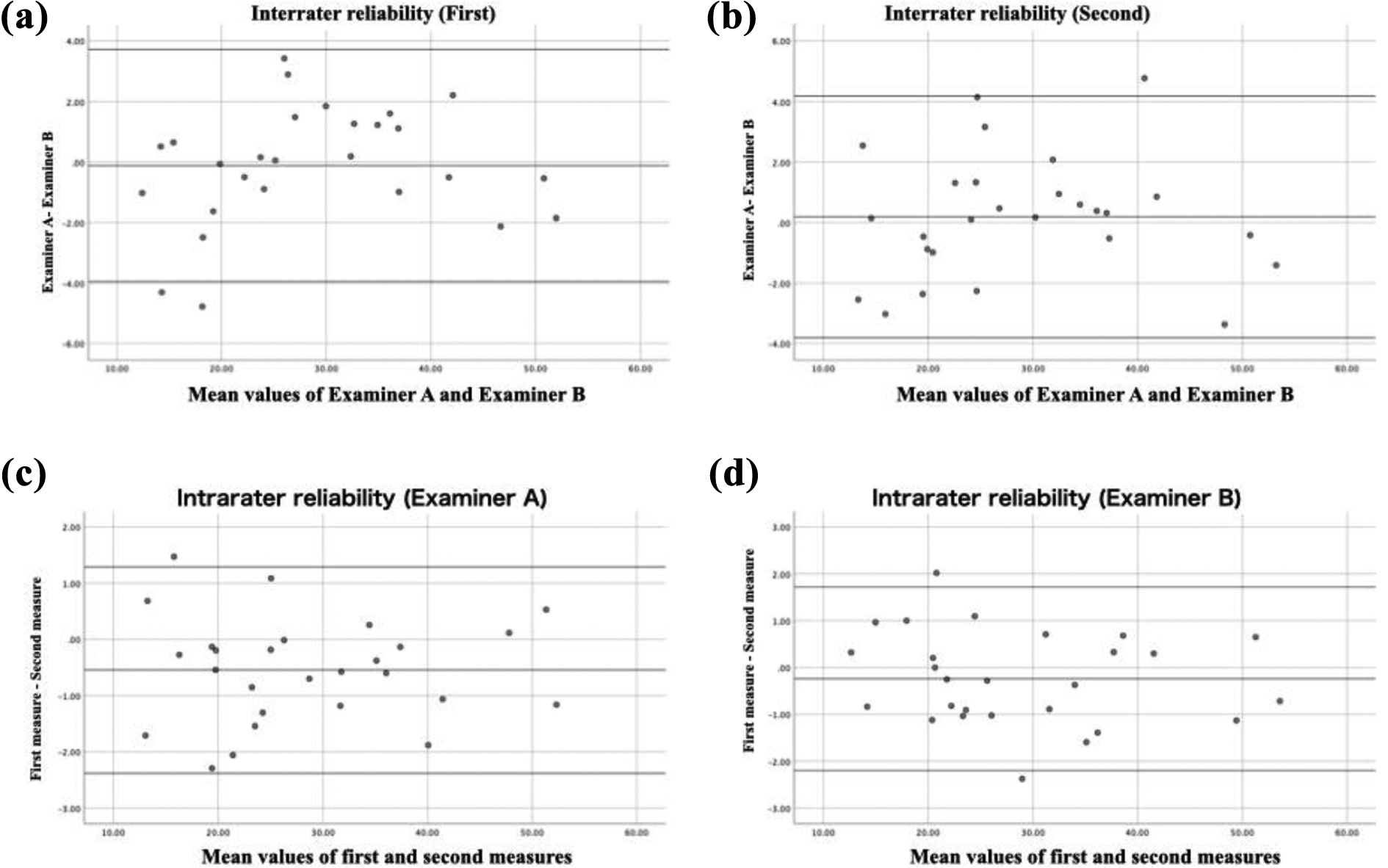
Bland–Altman plot of CHAS. (a) Bland–Altman plot of differences comparing examiners A and B with a mean difference of −0.11° and 95% LOA with the first measurement. (b) Bland–Altman plot of differences comparing examiners A and B with a mean difference of 0.19° and 95% LOA with the second measurement. (c) Bland–Altman plot of differences comparing first and second measurements with a mean difference of −0.54° and 95% LOA of examiner A. (D) Bland–Altman plot of differences comparing first and second measurements with a mean difference of −0.24° and 95% LOA of examiner B. CHAS: craniohorizontal angle in supine; LOA: limits of agreement.
For CHAS, the ICC (2, 1) of the interrater reliability of the first measurement was 0.98 (Table 3). Bland–Altman analysis yielded good reliability in both the first and second measurements without errors (Table 4, Figure 3). The LOA ranged from −4.0° to 3.7° in the first measurement and from −3.8° to 4.2° in the second measurement (Table 4).
Discussion
In this study, we investigated the reliability and accuracy of sagittal spinal postural alignment with the use of digital images based on previous studies.
Among the parameter of CVAS and CHAS used by the proposed method of this study, CHAS exhibited an excellent correlation with the conventional spinal postural alignment measurement method; however, CVAS exhibited no such correlation. In previous studies, CVA was used to evaluate posture in patients with cervical pain and school children, and its excellent reliability was reported. 20 –22 However, this study revealed that there was no correlation between CVAS and KI or BM. The reason for this is the difference in the measured position. It is considered that the measured limb position in this study is the supine position, and the part of the spinal column that was in contact with the bed surface (back and bed surface) differed depending on the subject. In other words, the lower spinal column is in contact with the bed in subjects with a high degree of hyperkyphosis, while subjects with normal spinal postural alignment have the upper spine in contact with the bed. The results of this study suggest that CVAS is an evaluation index for inaccurate spinal postural alignment.
Conversely, CHAS exhibited a strong correlation with the conventional measurement method of spinal postural alignment. CHA can estimate the position of the head from the position of the upper cervical spine and the angle of the cervical spine. 23,24
The excellent correlation between CHAS and the conventional methods for the measurement of spinal postural alignment revealed that the head position in the supine posture changed with changes of the spinal postural alignment. Liu et al. reported that the cervical tilt angle in the supine position was 53.0 ± 9.5° in people over 40 years of age and tended to increase with age. 25 Changes in spinal column alignment with aging affect both the cervical spine and the entire spinal column. The strong correlation between CHAS and KI or BM indicates that changes in the alignment of the entire spinal column lead to head position changes.
The calculation of the CHAS angle by ImageJ yielded excellent intrarater and interrater reliabilities. Landis and Koch mentioned that ICC >0.8 is considered almost perfect, and it was found that the measurements of hyperkyphosis with this method are highly reliable. 26 This is attributed to the fact that CHAS measurements simplify the confirmation of landmarks such as the tragus and external canthus on the image.
Fixed bias, which is a systematic error, was observed in the first and second measurements of Examiner A. To prevent this error, it is necessary to prepare a manual to ensure accurate placement of the landmarks. However, the LOA of examiner A ranged from −2.3° to 1.3°. Porto and Okazaki argued that the study of postural alignment with digital images yielded only ICC values. Therefore, there is a limit to clinical interpretation. 27 Therefore, the LOA of this study cannot be compared with other studies, but the LOA seems to be very small, and it is speculated that CHAS has increased accuracy. 28 Whether the LOA of this study is clinically acceptable will be clarified based on future data analyses.
Given that the CHAS calculated by our method is a method used to measure spinal postural alignment in the supine position without markers and without the necessity to expose the skin surface, it can compensate for the shortcomings of conventional spinal postural alignment measurement methods. CHAS can be measured repeatedly and can be used as a tool to promote behavioral changes in the subject. Furthermore, CHAS is considered as a method that can be easily incorporated in the posture and motor function tests that are necessary for the implementation of health promotion and long-term care prevention activities in the community.
The limitation of this study was attributed to the fact that the measurement was conducted on the right side of the subject. The subjects were elderly, and their postures may have been asymmetric owing to aging. 29 Analyses of images acquired from both sides might be necessary. In addition, this study cannot be generalized because it represents collective outcomes from measurements on elderly people only. Nevertheless, we believe that the CHAS method is likely to be available in the local communities. To allow community-dwelling elderly people to be evaluated within the community, it is necessary to make arrangements so that nonspecialized individuals can also conduct these measurements.
In the future, we plan to conduct a large-scale, cross-sectional survey to investigate the relationship between the results of this method and the physical and walking functions of the elderly.
Conclusion
We have proposed a method to measure spinal postural alignment that can compensate for the shortcomings of conventional measurement methods based on the application of the method of previous research studies on the measurement of sagittal spinal postural alignment. The CHAS method proposed herein is inexpensive, does not require skin exposure, and can be measured without markers. Furthermore, the CHAS can be measured even in frail elderly people whose standing is unstable because the measurement is performed in the supine position. The correlation of the spinal postural alignment between CHAS and the conventional measurement method was extremely good. CHAS also exhibited excellent reliability and accuracy. In the future, we will conduct a cross-sectional survey to clarify the relationship between spinal postural alignment data obtained with this method and the physical functions of local residents.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.