
Abstract
Study Design
Retrospective review of prospective database.
Objectives
Vertebral pelvic angles (VPAs) account for complexity in spine shape by assessing the relative position of each vertebra with regard to the pelvis. This study uses VPAs to investigate the shape of the fused spine after T10-pelvis fusion, in patients with adult spinal deformity (ASD), and then explores its association with proximal junctional kyphosis (PJK).
Methods
Included patients had radiographic evidence of ASD and underwent T10-pelvis realignment. VPAs were used to construct a virtual shape of the post-operative spine. VPA-predicted and actual shapes were then compared between patients with and without PJK. Logistic regression was used to identify components of the VPA-based model that were independent predictors of PJK occurrence and post-operative shape.
Results
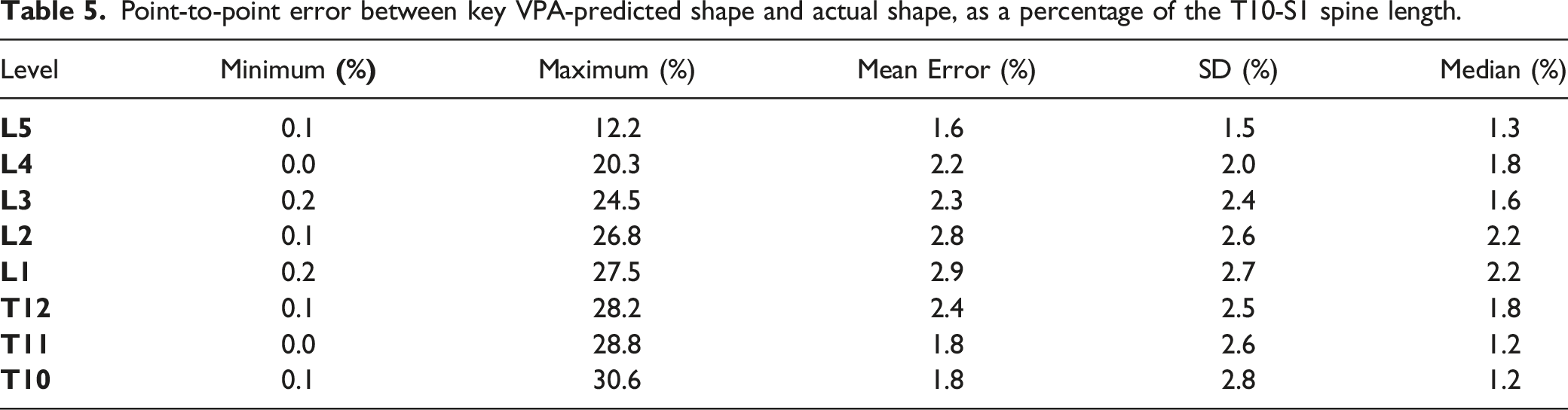
287 patients were included. VPA-predicted shape was representative of the true post-operative contour, with a mean point-to-point error of 1.6-2.9% of the T10-S1 spine length. At 6-weeks follow-up, 102 patients (35.5%) developed PJK. Comparison of the true post-operative shapes demonstrated that PJK patients had more posteriorly translated vertebrae from L3 to T7 (P < .001). Logistic regression demonstrated that L3PA (P = .047) and T11PA (P < .001) were the best independent predictors of PJK and were, in conjunction with pelvic incidence, sufficient to reproduce the actual spinal contour (error <3%).
Conclusions
VPAs are reliable in reproducing the true, post-operative spine shape in patients undergoing T10-pelvis fusion for ASD. Because VPAs are independent of patient position, L3PA, T11PA, and PI measurements can be used for both pre- and intra-operative planning to ensure optimal alignment.
Introduction
In recent decades, significant advances have been made in spinal deformity surgery, with an emphasis on the clinical relevance of the sagittal plane. Spinal alignment in healthy subjects was first described in the late 1980s.1,2 Soon after, the importance of pelvic incidence (PI) and its relationship with spinal curvatures, such as the lumbar lordosis (LL), 3 became apparent, and studies examining the correlations between malalignment and clinical outcomes started to emerge.4-6 The Scoliosis Research Society (SRS)-Schwab classification marked an important progression, introducing simple objectives of correction based on correlations with health-related quality of life (HRQOL) instruments, while providing 3 basic parameters to guide realignment procedures 7 : a pelvic tilt (PT) less than 20°, a mismatch between pelvic incidence and lumbar lordosis (PI-LL) less than 10°, and a sagittal vertical axis (SVA) less than 40 mm. While this classification has the advantage of being simple and easy to apply, permitting widespread adoption by adult spinal deformity (ASD) surgeons, it was not designed to address the issue of mechanical complications such as proximal junctional kyphosis (PJK) and related adjacent segment concerns. Such radiographic changes occur in 30-50% of patients following ASD surgery and are not without consequences, with an associated rate of revision surgery ranging from 13% to 55%.8,9
Recent literature supports a probable multifactorial etiology for PJK, with re-alignment components appearing to play a critical role.
10
However, the literature remains unsettled with regard to specific associations between alignment and the occurrence of PJK. Some studies have reported an association with a lower post-operative PI-LL mismatch, while others found no difference in post-operative PI-LL mismatch between patients with and without PJK.11-13 We hypothesize that these inconsistent results could be explained by the inability of the classic Cobb angle, between the superior endplates of L1 and S1, to accurately depict the shape of the lumbar spine. In fact, one of the weaknesses of the Cobb angle method is its failure to account for the relative spatial position of each vertebra. For instance, the classic lumbar Cobb angle is unable to capture differences in the lumbar shape resulting from disc degeneration at differing levels.
14
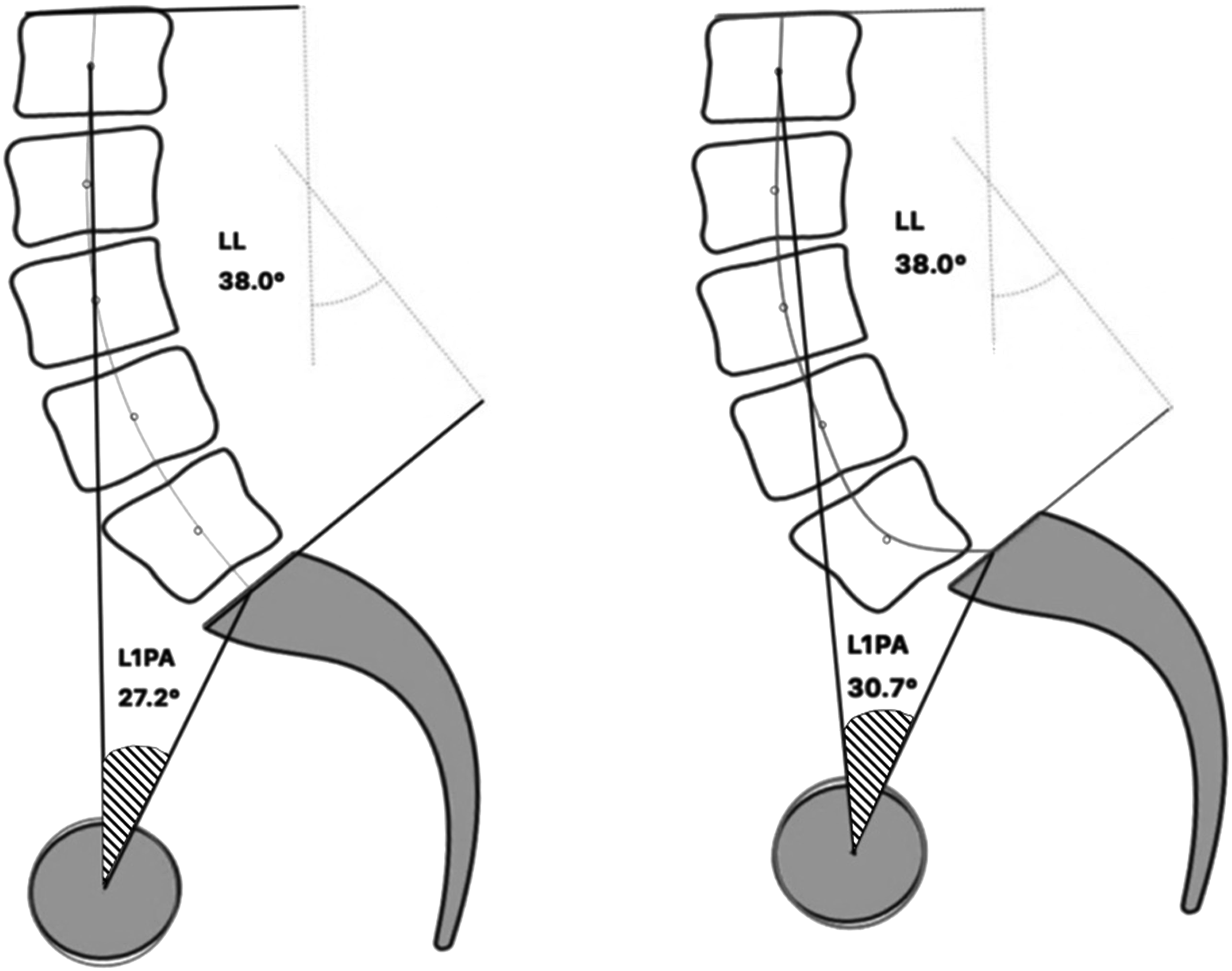
Distinguishing between these shapes is important because, for the same LL, a loss of height and lordosis within caudal discs typically leads to a more forward spine (increased SVA) than does a comparable loss within cranial discs (Figure 1). Additionally, Cobb angles are not able to capture translational motion (Figure 2). For the same lumbar lordosis, measured with the Cobb angle spanning L1-S1, patients with degeneration of the lumbar spine may present with variability in shape. A distal loss of lordosis produces a more forward displacement of the spine, ie increased SVA, than does a proximal loss of lordosis. Difference in measurement between the Cobb angle and vertebral pelvic angle in the setting of a translation.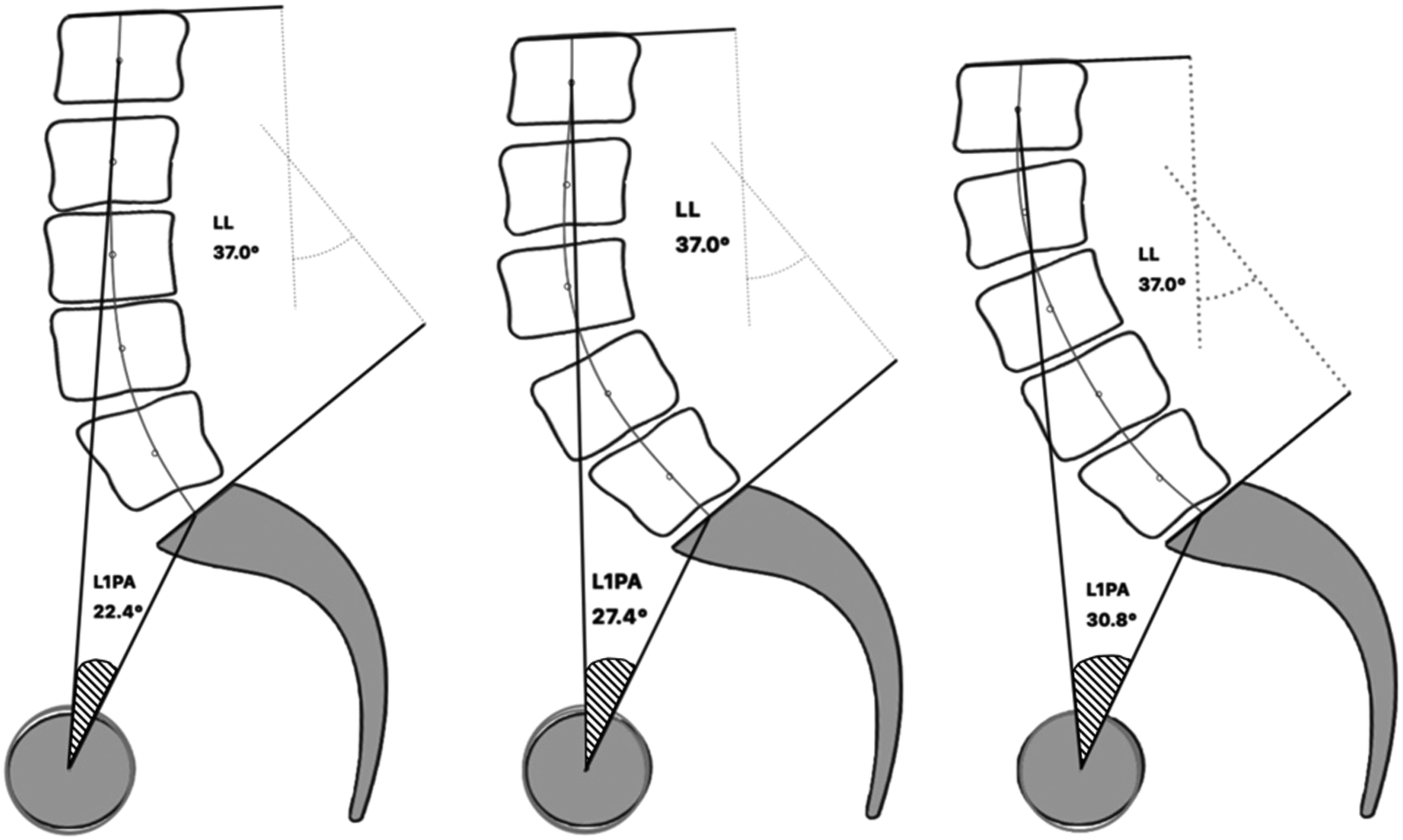
In contrast to Cobb angles, vertebral pelvic angles (VPAs) account for the relative position of each vertebra with regard to a fixed reference, the pelvis. These parameters are independent of patient position, so they can be used for both pre-operative planning and intra-operative assessment. VPAs are well known by ASD surgeons and are currently assessed through measures of thoracic pelvic angle (TPA) and lumbar pelvic angle (LPA).15,16 This study aims to investigate the shape of the fused spine in the setting of a commonly utilized “T10-pelvis” fusion, using a more detailed and comprehensive approach, and then to explore its potential association with proximal junctional kyphosis. We hypothesize that certain shapes of the fused spine will correlate more closely with the development of PJK and that by measuring VPAs, we will be able to predict this post-operative spine contour and, therefore, the occurrence of PJK.
Methods
Patient Sample
This was a retrospective review of a prospective, multicenter database of surgical ASD patients, collected through the International Spine Study Group. Institutional Review Board (IRB) approval at each of the 22 participating sites was obtained prior to conducting the study (IRB No. 2014-357). Informed consent was obtained from all participating patients. Inclusion criteria for database entry were age greater than 18 years and radiographic evidence of ASD, defined by the presence of at least one of the following: coronal Cobb angle greater than 20°, SVA greater than 5 cm, PT greater than 25°, and/or thoracic kyphosis (TK) greater than 60°. Database exclusion criteria were spinal deformities due to neuromuscular, post-traumatic, neoplastic, rheumatologic, and/or infectious processes. In addition to the database inclusion criteria, the present study required that included subjects have undergone operative treatment of ASD with instrumented fusion from T10 to the pelvis and have at least 6 weeks of follow-up data available.
Data Collection
Collected data included sex, age at surgery, body mass index (BMI), and various radiographic information. Full-length, freestanding lateral and anteroposterior spine radiographs were obtained at baseline and at 6 weeks following surgery. Radiographic parameters were measured using dedicated, validated software (SpineView, ENSAM ParisTech, Paris, France)
17
and Matlab (Matlab 2015b, MathWorks). Radiographic parameters of interest included: PI, PT, LL, PI-LL mismatch, T10-L2 thoraco-lumbar angle, TK (T4-T12), focal alignment parameters based on segmental sagittal Cobb angles (L5-S1, L4-L5, L4-L3, L3-L2, L1-L2), location of the lumbar apex, maximum lordosis value, number of vertebrae within the maximum lordosis, vertebral pelvic angles (VPAs) at each level from L5 to T1, intervertebral distances, and total length of the spine between T10 and S1 (Figure 3). Radiographic PJK was defined based on the criteria reported by Glattes et al
18
as a kyphotic angle >10° between the upper-most instrumented vertebra (UIV) and the vertebra 2 levels above, along with a kyphotic change >10° from the pre-operative baseline. A: Classic sagittal alignment parameters. B: Segmental alignment parameters with examples of Cobb angles for L1-L2 and L4-L5. C: Examples of vertebral pelvic angle measurements, which are measured between the line from the femoral head axis to the centroid of the vertebra and the line from the femoral head axis to the middle of the S1 superior end plate.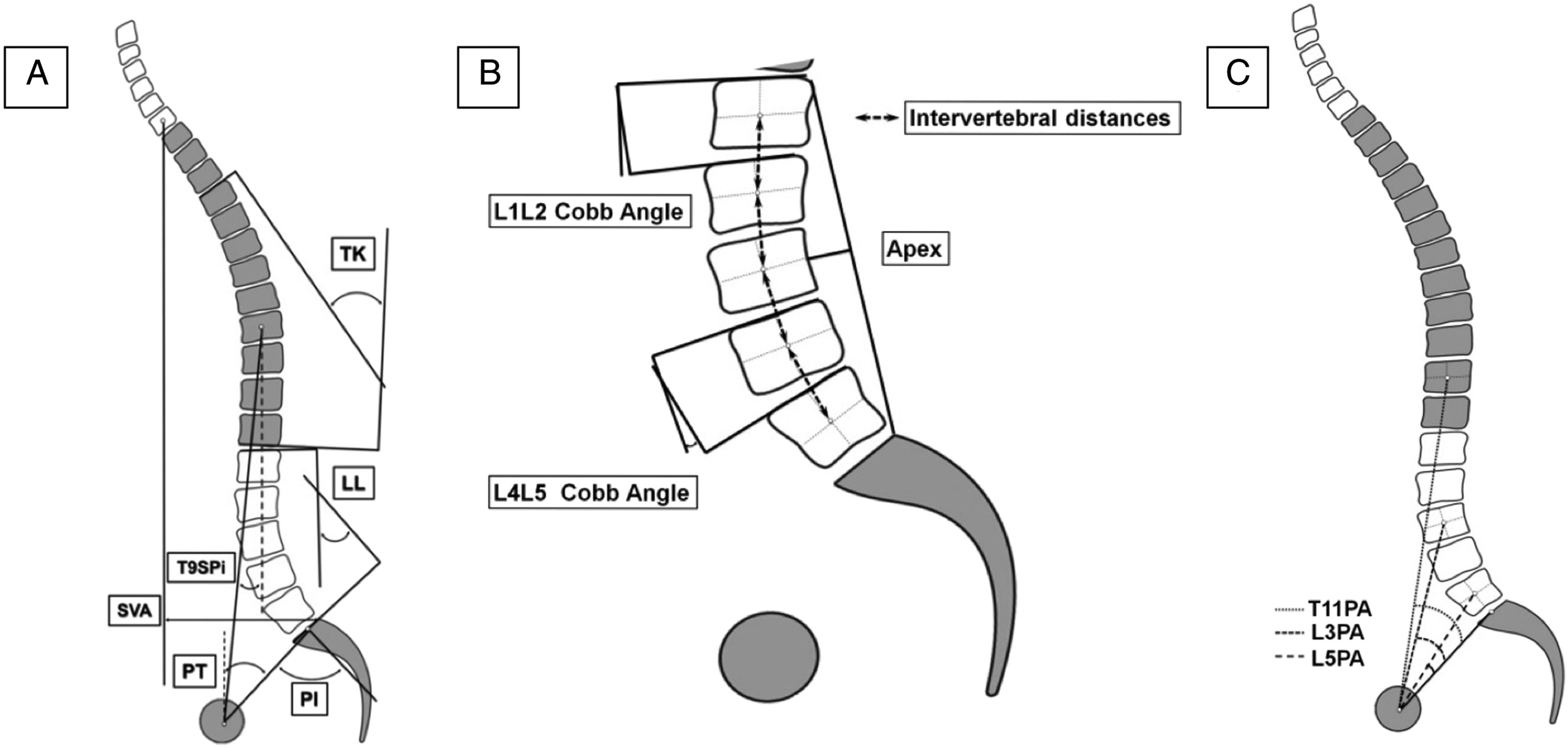
Statistical Analysis
The collected demographic and radiographic data were described and analyzed at baseline and at 6 weeks post-operatively. Changes in radiographic alignment were also investigated, including pre-to post-operative analysis of sagittal alignment and the presence of radiographic PJK.
Validation of the VPA-Based Shape
The VPA-based post-operative shape of the fused spine was determined using a combination of the measured and predicted post-operative VPAs for all vertebrae from L5 to T10, along with the pre-operative intervertebral distances from S1 to T10 (Figure 4). This was then compared to the actual spine shape directly drawn on x-ray film, by measuring the point-to-point distance between the 2 shapes at each level. The results were expressed as a percentage of the length of the spine from T10 to S1, in order to compare patients independently of their morphology. Workflow to construct the VPA-predicted spine shape: A combination of pre-operative intervertebral distances and post-operative, measured and calculated VPAs were utilized. The spine shape generated using this method was then compared to the actual post-operative shape for validation.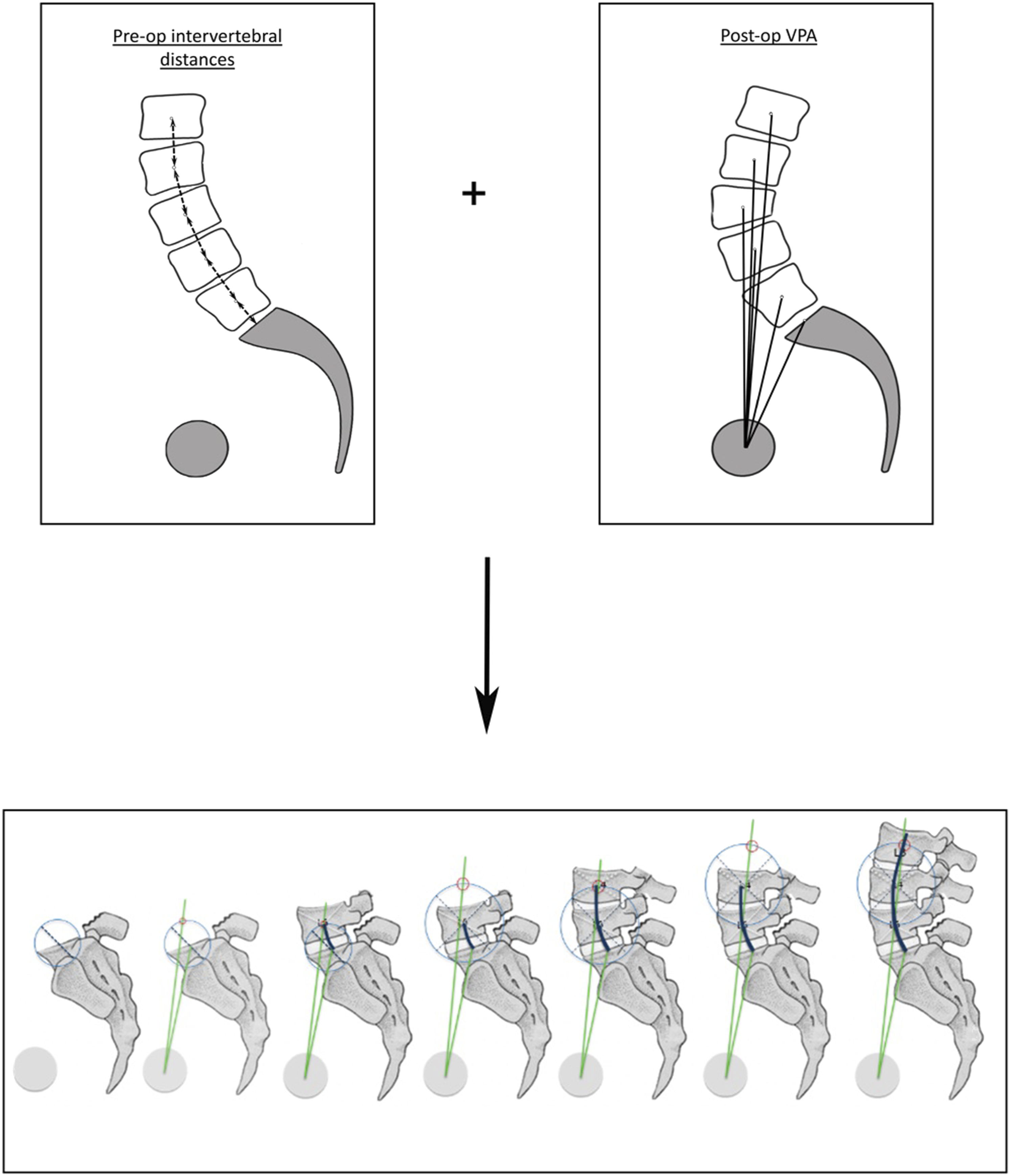
VPA-Predicted Shape in the Setting of PJK
Patients were stratified into 2 groups: those with PJK and those without PJK (NPJK) at 6 weeks following surgery. A comparison of demographic and radiographic parameters, including the VPAs, was performed using Student’s t-tests or Chi-Squared tests, as appropriate. To describe differences in progression of the spine shape between PJK and NPJK patients, a derivative analysis of the mean VPA-predicted curve was performed. A negative derivative value demonstrated a posterior progression of the shape relative to the pelvis, while a positive value demonstrated an anterior progression. These derivative values were then compared between the 2 groups. A positive difference demonstrated a more posterior (or less anterior) progression of the shape for PJK patients, while a negative difference demonstrated a more anterior (or less posterior) progression.
Prediction of Post-operative T10-S1 Shape Using Only a Minimum Number of Key VPAs
Using a logistic regression, with a stepwise forward method controlling for age and PI, we identified the minimum subset of VPAs (coined “key VPAs”) that would enable prediction of PJK occurrence. Then, key VPAs and PI were entered into a set of polynomial regressions to predict all other VPAs from L5 to T10. This method allowed us to reconstruct a predicted, post-operative T10-S1 shape by measuring only the key VPAs.
Results
Cohort Description
Our sample included 287 patients, with a mean age of 64.7 ± 8.6 years and a female predominance (76.2%). These patients, all of whom were treated with a T10-pelvis fusion by inclusion criteria, presented with typical baseline malalignment reflective of the ASD population, with mean PT of 26°, mean PI-LL of 23.9°, and mean SVA of 81.2 mm. Significant improvement after surgery was observed across the sample, with a pre-to post-operative decrease of 5° for PT, 22.2° for PI-LL, and 50.7 mm for SVA; all P < .05.
Regarding the surgical procedures performed, 100% of our patients underwent posterior fusion, with only 6.3% of cases using minimally invasive surgery techniques. 76.9% of patients underwent direct decompression, 78.1% received some sort of osteotomy, and 18.8% had a major osteotomy (either pedicle subtraction osteotomy or vertebral column resection). 67.1% had an interbody fusion procedure, with 26.1% undergoing anterior lumbar interbody fusion, 36.9% undergoing posterior lumbar interbody fusion, and 14.3% having lateral lumbar interbody fusion. Median estimated blood loss was 1500 mL (IQR 800 to 24,500 mL), median operative time was 427min (IQR 336 to 561min), and median length of stay was 7 days (IQR 6 to 9 days).
VPA-Based Shape Comparison Between PJK Patients and NPJK Patients
Comparison of demographic and alignment parameters between PJK and NPJK patients.
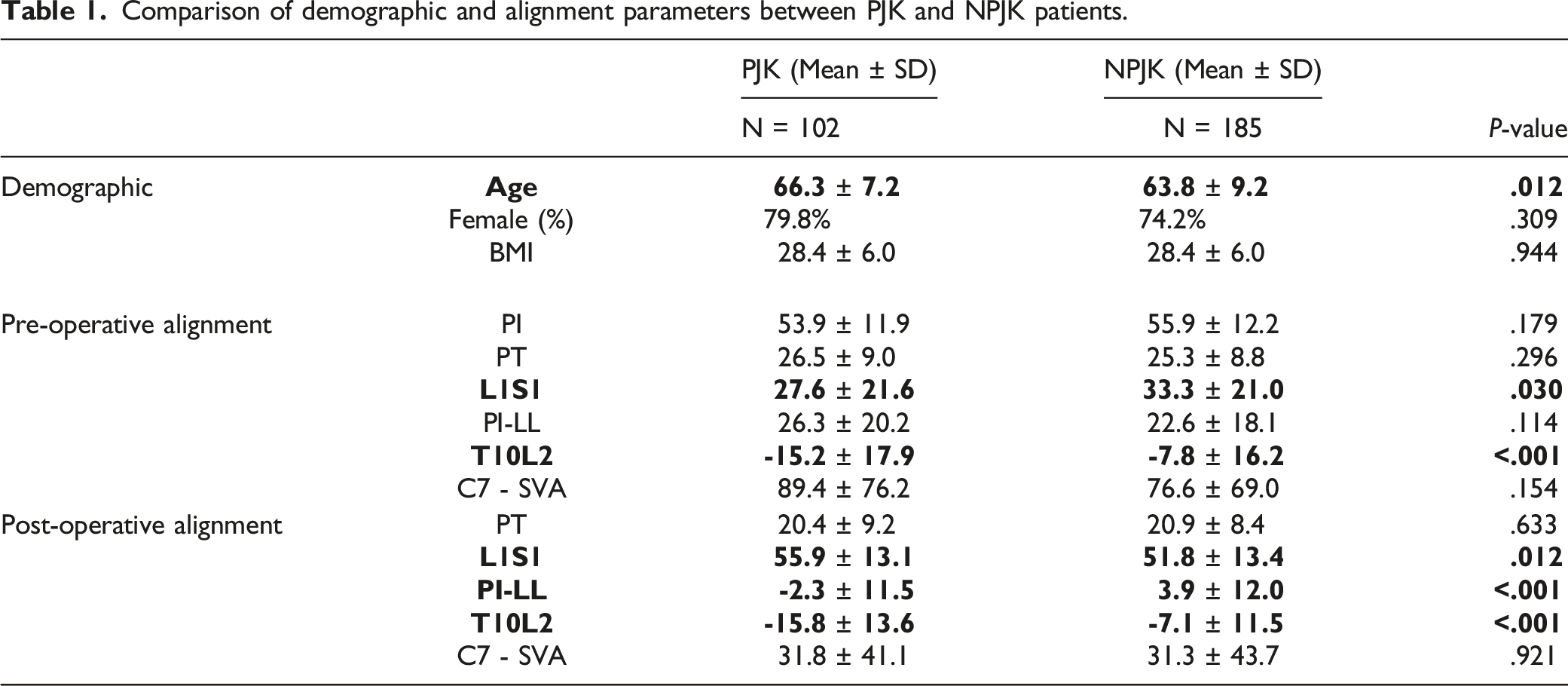
Comparison of segmental parameters between PJK and NPJK patients.
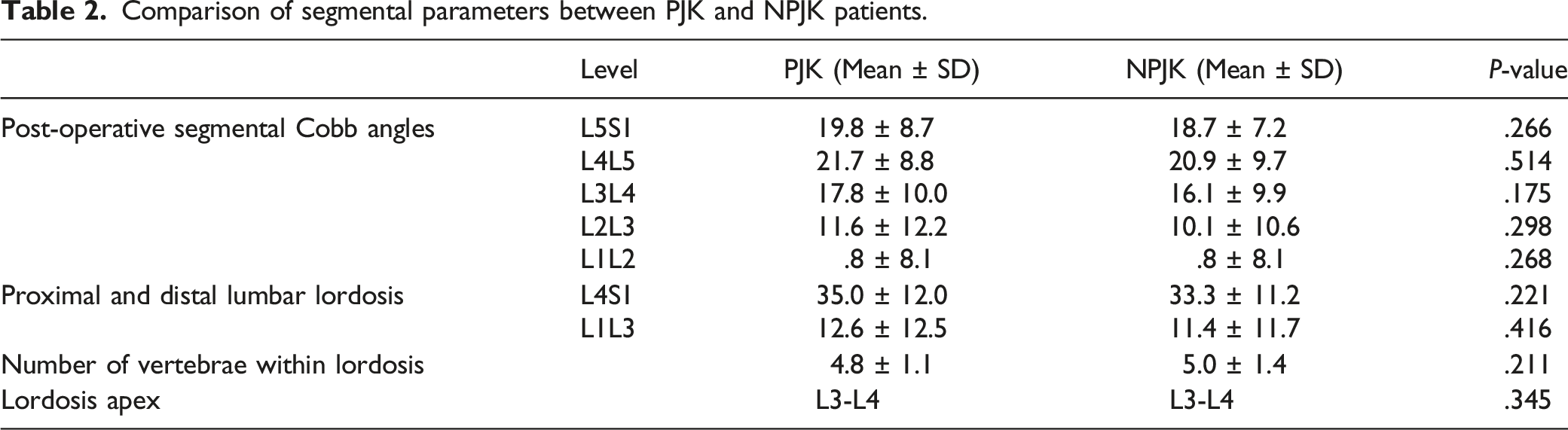
Comparison of post-operative VPAs between PJK and NPJK patients.
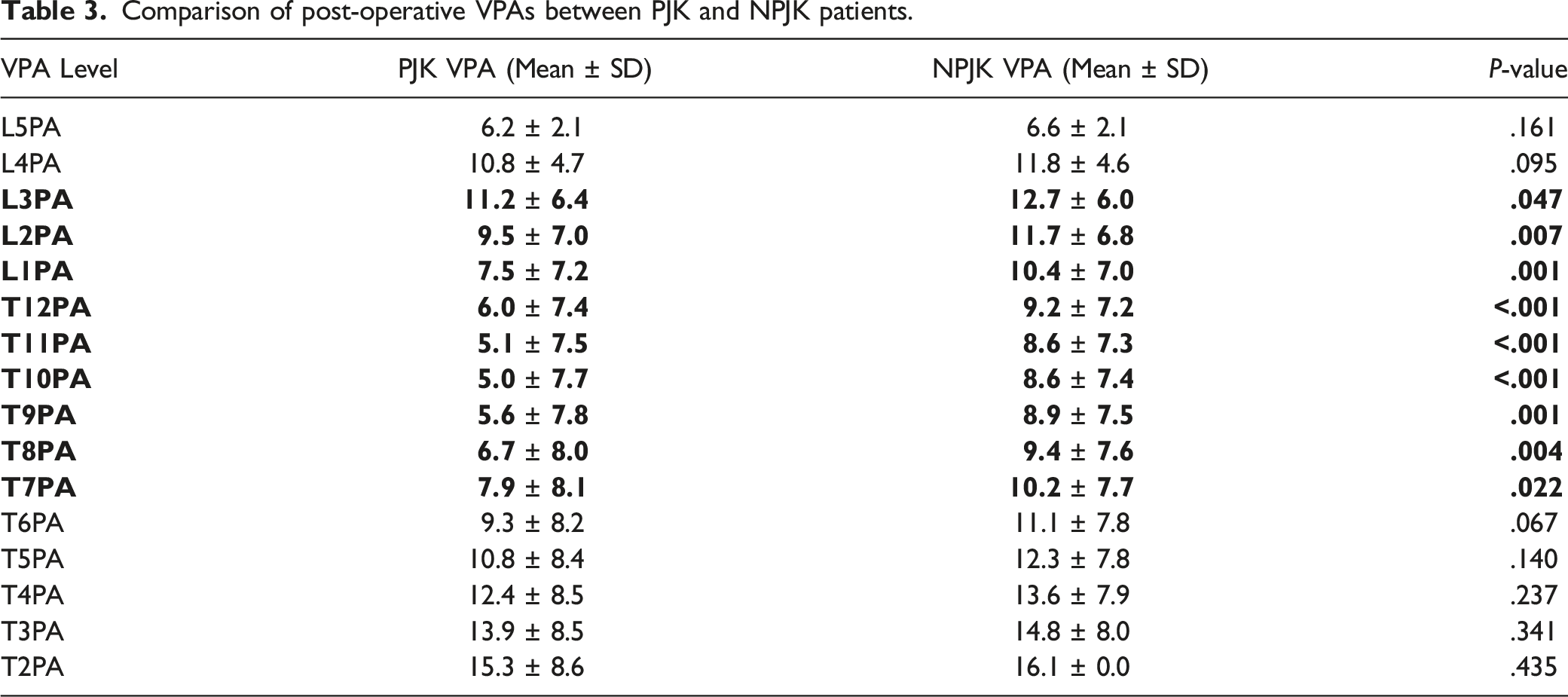
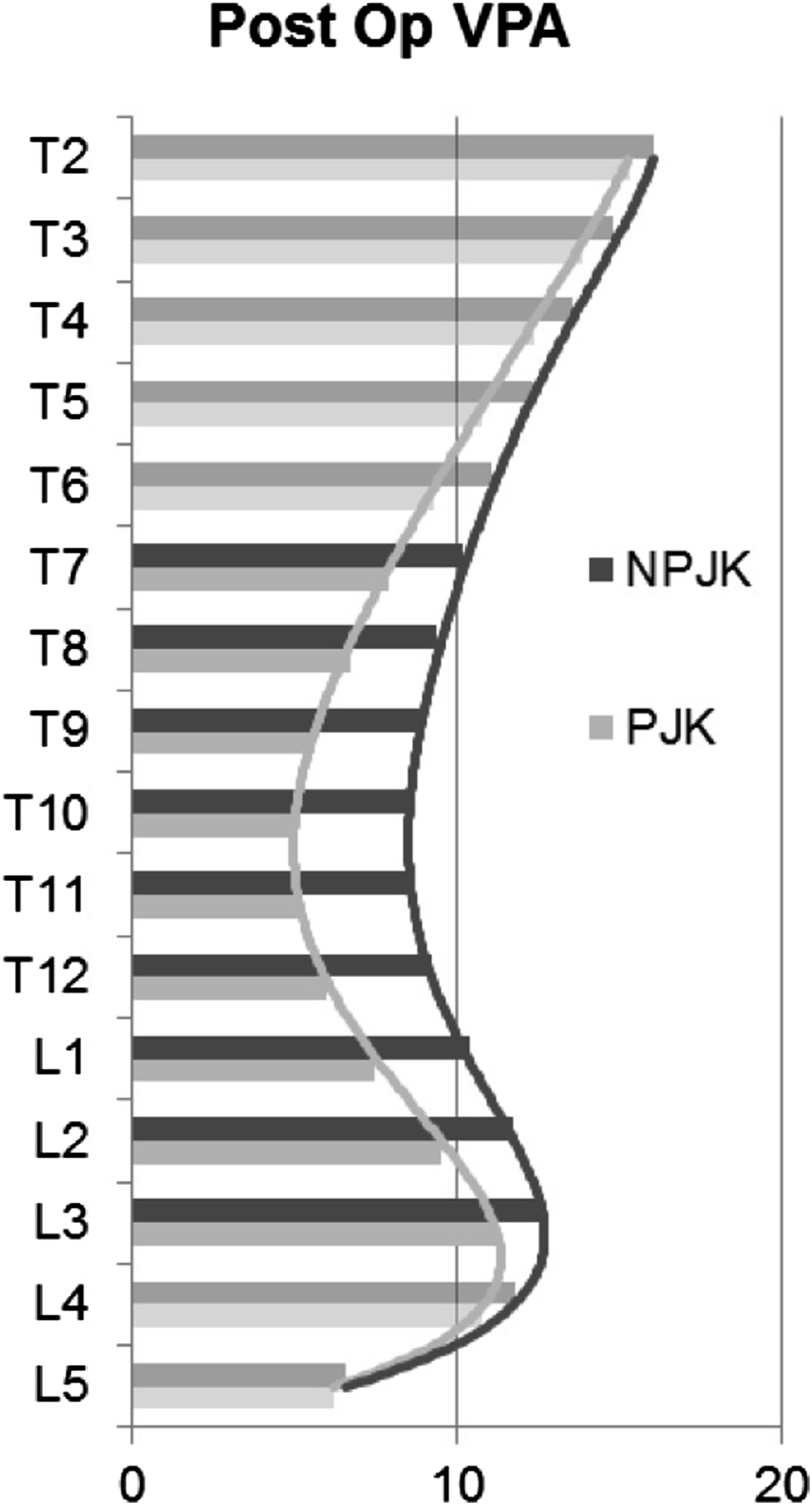
Histogram representing VPA values for PJK and NPJK patients.
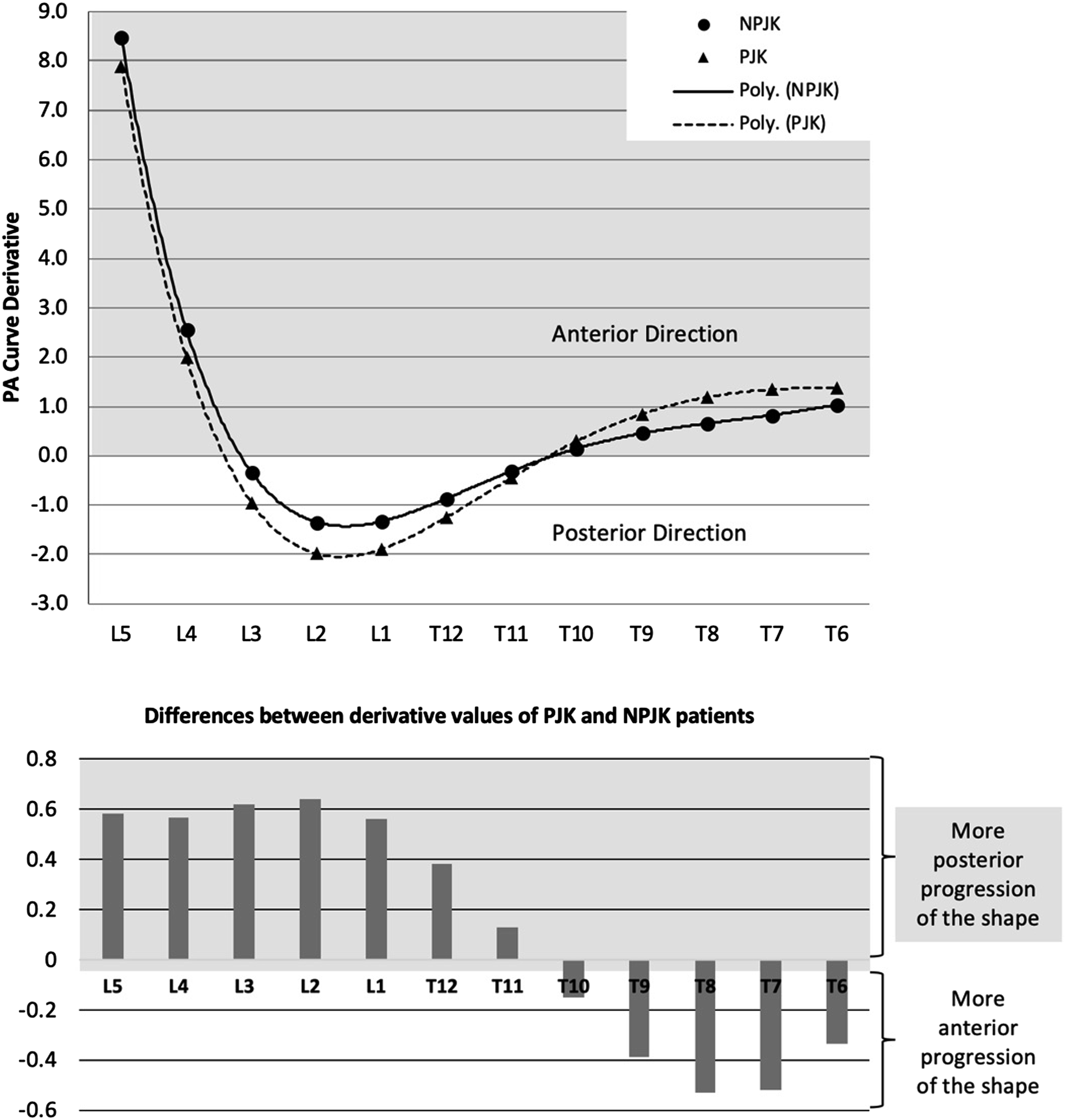
Derivative analysis of VPA curves for PJK and NPJK patients.
Prediction of Post-operative T10-S1 Shape Using Key VPAs
Equations to calculate non-measured VPAs using PI, L3PA, and T11PA.

Point-to-point error between key VPA-predicted shape and actual shape, as a percentage of the T10-S1 spine length.
Discussion
Improved understanding of spino-pelvic alignment has permitted significant advances in spine surgery in recent decades. As new concepts are developed, the importance of spine shape has become increasingly apparent. Roussouly et al 19 investigated the shape of the spine by establishing a classification with 4 types, and even a fifth in the most updated version. 20 However, ability of this classification to drive pre-operative planning has remained limited because the physiologic lumbar shape is more strongly correlated with the sacral slope than with the PI. In other words, knowing the PI is not sufficient to deduce the physiological shape, or Roussouly type, of a given patient prior to pathologic alteration of the spine by the aging process. Consequently, it becomes increasingly difficult for the surgeon to know which ideal shape should be restored in a patient with ASD, simply based on the PI.
Instead, Pesenti et al 21 preferred a different approach to describing the lumbar spine, whereby the lumbar curve is divided into L4-S1 and L1-L4. They demonstrated a linear relationship between the PI value and proximal lordosis, while distal lordosis remained independent of the PI. 21 While these results are valuable, our study showed that neither proximal lordosis nor distal lordosis values were significant parameters to discriminate between patients who subsequently develop PJK and those who do not. As such, we sought to develop an accurate method for describing the shape of the spine that would be capable of predicting PJK occurrence, without unnecessarily increasing the number of parameters already abundant in the literature.
In a previous study, Lafage and colleagues used Ferguson angles and successfully demonstrated that a more proximal correction of LL was associated with a higher rate of PJK. 22 However, Ferguson angles are not commonly used in clinical practice and are time-consuming to measure. In our study, other well-known angles, namely VPAs, appeared sufficient in highlighting segmental differences in the lumbar spine shape between PJK and NPJK patients. These angles were developed by Protopsaltis et al as an advantageous alternative to the SVA, as they are independent of patient pelvic position and do not require calibration of the radiographs. 15
In this study, we derived the vertebral pelvic angle for any levels not directly measured and were able to accurately describe the average shape progression, showing that PJK patients had a more posterior progression within the fused spine, relative to the pelvis, with the maximum posterior divergence of the shape between the 2 groups occurring at L2 and L3. These results are consistent with previous studies, citing overcorrection of LL23,24 and primary correction within the proximal part of the lumbar spine22,25 as risk factors for PJK development.
By combining VPAs with intervertebral length, we constructed a predicted shape of the fused spine. As the goal was to guide the surgeon in planning alignment correction for ASD patients, we investigated the shape in ASD patients, testing the hypothesis that specific spinal contours present a higher risk for PJK occurrence. We successfully demonstrated that by utilizing VPAs and preoperative intervertebral distances, it is possible to accurately represent the true post-operative T10-S1 shape.
Finally, by creating a model using only a subset of VPAs, we discovered that 2 key VPAs were most strongly correlated with PJK occurrence: L3PA and T11PA. These findings imply that surgeons would simply have to measure PI and pre-operative intervertebral distances on preoperative x-rays, along with L3PA and T11PA during surgery, in order to accurately predict post-operative spinal shape. These findings suggest a tangible method that could be used as an intra-operative reconciliation tool for controlling the shape in the setting of a T10-pelvis fusion. 26
This study is not without limitations. Although a 68% positive predictive value is acceptable, it is far from perfect and highlights proximal junctional kyphosis as a multifactorial event, with sagittal alignment being just one of the important factors. 27 Moreover, this study is only applicable for T10-pelvis instrumentation surgeries and cannot be extrapolated beyond this. Further studies are needed for other lengths of fusion.
Conclusion
VPAs appear to be highly accurate in describing shape variations within the fused spine that are associated with PJK occurrence, and a model using only L3PA, T11PA, and PI is sufficient to predict post-operative shapes of the T10-pelvis stabilized spine. Still, further investigations will be needed to determine thresholds values for these key VPAs, in order to provide the optimal alignment for ASD patients. By combining this shape-control method with other known concepts, such as the SRS-Schwab classification, the orthopaedic spine community could build a very powerful tool for improving clinical outcomes, while minimizing the risk of PJK in patients with ASD.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author’s Note
The International Spine Study Group (ISSG) is funded through research grants from DePuy Synthes (current), Nuvasive (current), K2M (current), Innovasis (past), Biomet (past), and individual donations. Funding sources did not play a role in investigation.