
Abstract
Background:
Prophylactic pinning of the uninvolved side after unilateral slipped capital femoral epiphysis (SCFE) is controversial as it balances increased surgical risks against the possibility of protecting a normal hip from initial slip and deformity. A posterior sloping angle (PSA) of greater than 12–14.5° has been proposed by various authors as a treatment threshold to predict for contralateral hip progression and prophylactic pinning.
Methods:
A retrospective review of a 10-year series of patients with the diagnosis of SCFE and follow-up of 18 months was conducted. Patients were divided into two groups, those with Isolated Unilateral Slips and those who subsequently underwent Subsequent Contralateral Progression. PSA measurements were performed by two clinicians and assessed for inter-observer reliability. Data collected included age, sex, ethnicity, Loder class, endocrinopathy, renal impairment, radiation exposure, and PSA.
Results:
There were no significant differences between the distribution of gender, site of slip, age of onset, Loder class, and presence of medical comorbidities between the Isolated Unilateral Slip and Subsequent Contralateral Progression groups (p > 0.05). The mean PSA value was not significantly higher in the Subsequent Contralateral Progression group (17.9 ± 4.32 (10.5–23.5)) compared to the Isolated Unilateral Slip group (15.8 ± 5.31 (6–26)) (p = 0.32). The receiver operator coefficient-derived ideal treatment threshold of 16.5° gave a sensitivity of 0.71, specificity of 0.64, and number needed to treat of 3.
Conclusion:
PSA differences between the Subsequent Contralateral Progression and Isolated Unilateral Slip groups were not statistically significant in this series. All proposed treatment thresholds had poor specificity. Prophylactic pinning should not be based on isolated PSA values.
Level of evidence:
III.
Introduction
Slipped capital femoral epiphysis (SCFE) is the most common hip disorder in adolescents, with a prevalence of 10.8 cases per 100,000. 1 SCFE mostly occurs in the age range of 9–16 years with the average age at diagnosis of 13.5 years for boys and 12.0 years for girls. 2 The vast majority of SCFE patients are “idiopathic” without identifiable risk factors. 3 Atypical SCFEs are those that occur in the presence of an endocrine disorder, 4 renal failure osteodystrophy, 5 or radiation therapy. 6 The risk factors for further progression include atypical SCFE presentation, obesity, male gender, and early age of onset. 7 In cases of subsequent contralateral progression, the second slip was diagnosed within 18 months of the first slip 82% of the time. 8 The management of SCFE is targeted to prevent further deformity and vascular compromise. Fixation of the contralateral hip if clinically and radiologically normal is controversial especially in cases of idiopathic SCFE without risk factors. Proponents of prophylactic pinning attempt to prevent future osteonecrosis and chondrolysis 9 while other parties advocate close follow-up and observation to minimize complications of infection, chondrolysis, and osteonecrosis from the additional procedure. 10 Conclusions derived from multifactorial decision analysis of the risk–benefit trade-off have been diametrically opposite. 11,12 A new radiological parameter predicting contralateral slip could help tilt the decision balance.
The posterior sloping angle (PSA) of the physis is defined as the angle between the line along the plane of the physis and the line perpendicular to the femoral neck-diaphyseal axis on an axial radiograph. It is a measure with high inter-observer and intra-observer reliability. 13 To date, increases in PSA have been proposed to be predictive of contralateral slip in SCFE patients with threshold values for prophylactic fixation ranging from 12° to 14.5° with a number needed to treat (NNT) between 1.79 and 2.2. 1,8, 14, 15
An easily obtained and reproducible radiographic treatment threshold for prophylactic fixation is attractive and would contribute to resolving the controversy surrounding prophylactic fixation of a clinically and radiologically normal hip. Between the studies cited in Table 2, a range of treatment thresholds and NNTs have been proposed. Furthermore, all previous literatures have been derived from Western populations. We attempted to analyze the role of PSA in the Asian ethnic context.
This retrospective study aims to:
Evaluate the role of the PSA in predicting contralateral progression of SCFE in the Asian context.
Derive a PSA treatment threshold to guide the management of future patients.
Validate the intra-observer reliability of PSA measurement among junior surgical staff.
Materials and methods
A 10-year series of patients (January 2005–April 2015) who had initially presented to the KK Women’s and Children’s Hospital, Singapore, and diagnosed with SCFE was retrospectively analyzed. Patients were divided into two groups: Isolated Unilateral Slips without clinical or radiological evidence of subsequent contralateral hip involvement and Subsequent Contralateral Progression to contralateral SCFE within an 18-month window. Patients with bilateral SCFE with immediate bilateral pinning at presentation have been tabulated for completion but are excluded from the analysis. Clinical evidence of hip involvement was defined as pain, limited weight-bearing, or loss of range of motion. Radiological evidence of SCFE was defined as the presence of an abnormal Klein’s sign, the metaphyseal blanch sign of Steel, or frank slippage. The decision to perform bilateral pinning at first presentation was based on either radiological signs or clinical features of involvement of the contralateral head.
PSA measurements were performed with the Angle Measurement Tool in Carestream Vue Motion version 12.0.0.0757 (Carestream Health Inc., Rochester, New York, USA) on the frog-leg lateral film obtained either just prior to surgery of the affected hip or in the immediate postoperative period if not obtained preoperatively. All radiographs used for PSA measurement were within 1 month of surgical pinning and hence are representative of the information obtainable if planning prophylactic bilateral pinning in the same sitting. The frog-leg lateral views were routinely performed in our institution with the patient in supine position, with feet together and hips abducted as widely as tolerated.
The PSA was constructed by a line drawn perpendicular to a line running from a point in the center of the shaft of the femur to a point in the center of the femoral neck on the frog-leg lateral view and a line perpendicular to the best fit line of the plane of the physis (Figure 1). The measurement was conducted by two clinicians; (1) a fellowship-trained pediatric orthopedic surgeon and (2) an orthopedic surgery resident trainee. The measurements were obtained independently and in a blinded fashion. The final results were assessed for inter-observer reliability via the intra-class correlation coefficient (ICC). 16
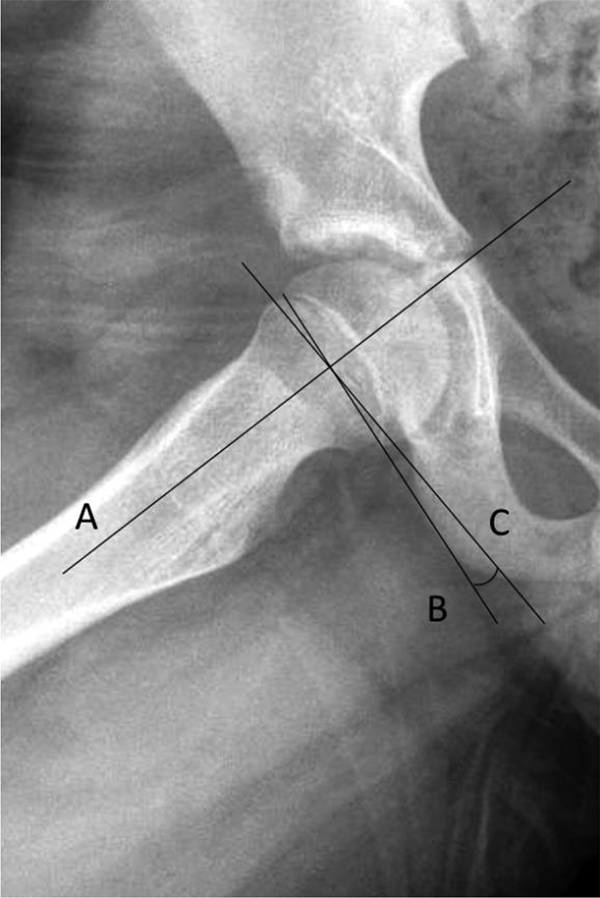
Construction of the posterior slope angle. Line A is along the femoral neck-diaphyseal axis. Line B is the best fit plane of the physis. Line C is perpendicular to A. The PSA is the angle subtended between B and C. PSA: posterior sloping angle.
The final measurement of PSA was the average of the values. Data collected included age, sex, ethnicity, Loder class, presence of endocrinopathy, renal impairment, radiation exposure, time to contralateral fixation, and PSA.
Ethical approval by the institutional review board was obtained for this study.
Statistical analysis
Categorical variables are presented as percentages and compared using Fisher’s exact test. Continuous variables are presented as mean ± standard deviation and range. Comparisons were made by use of the unpaired, two-tailed t test; the null hypothesis being that there was no significant difference between the group that had Isolated Unilateral Slip and the Subsequent Contralateral Progression group. The values of p < 0.05 were considered significant. A receiver operator coefficient (ROC) curve was generated with the averaged PSA measurement to predict the best treatment threshold. Statistical analyses were performed using MedCalc for Windows, version 15.8 (MedCalc Software, Ostend, Belgium).
Results
Fifty seven patients with SCFE were identified. Nine patients were excluded due to inadequate follow-up of at least 18 months. Five patients had bilateral slippage and pinning at presentation. Within the study groups, 7 (16.3%) patients had Subsequent Contralateral Progression while 36 (83.7%) remained stable with an Isolated Unilateral Slip. The overall gender distribution of the study population was 31 (72.1%) males and 12 (27.9%) females. The average age was 12.1 years (6–15) with males 12.7 (6–15) years and females 11.0 (9–14) years. The ethnicity was distributed as 13 (30.2%) Chinese, 9 (20.9%) Malay, 18 (41.8%) Indian, and 3 (7.0%) others. All patients had adequate radiographs. Seventeen (39.5%) slips occurred on the left and 26 (60.5%) occurred on the right hip at presentation. The Loder class was found to be unstable in 11 (25.6%) and stable in 32 (74.4%). Seven patients had endocrinological medical comorbidities with six in the Isolated Unilateral Slip group suffering from impaired fasting glucose and one in the Subsequent Contralateral Progression group with diabetes type 2. There were no statistical differences between the gender, site of slip, age of onset, Loder class, and presence of medical comorbidities between the Isolated Unilateral Slip and Subsequent Contralateral Progression groups (p > 0.05). The mean interval from index surgery to contralateral fixation was 43.7 weeks (16.2–77). The mean PSA value was higher in the Subsequent Contralateral Progression group (17.9 ± 4.32 (10.5–23.5)) compared to the Isolated Unilateral Slip group (15.8 ± 5.31 (6–26)) but the difference in PSA values did not reach statistical significance (p = 0.32) with overlapping confidence intervals. A detailed breakdown of values is shown in Table 1. The ICC was high at 0.89 between observers with 91% of values occurring within 5° of each other and a maximum discrepancy of 8°. The area under the ROC curve was 0.62. The ROC-derived ideal treatment threshold for this series was 16.5° with a sensitivity of 0.71, specificity of 0.64, and NNT of 3 (Figure 2). Referencing the highest value quoted in previous clinical literature, a treatment threshold of 14.5° gave a sensitivity of 0.85, specificity of 0.43, and NNT of 4. Referencing the cutoff value as derived from a lab-based biomechanical study 17 utilizing sawbones of 15° gave a sensitivity of 0.71, specificity of 0.5, and NNT of 3.3.
Demographics and PSA values of subjects.

IUS: Isolated Unilateral Slip; SCP: Subsequent Contralateral Progression; PSA: posterior sloping angle; SCFE: slipped capital femoral epiphysis.
a Mean ± standard deviation (range).
b PSA values in hips with established SCFE are not meaningful.
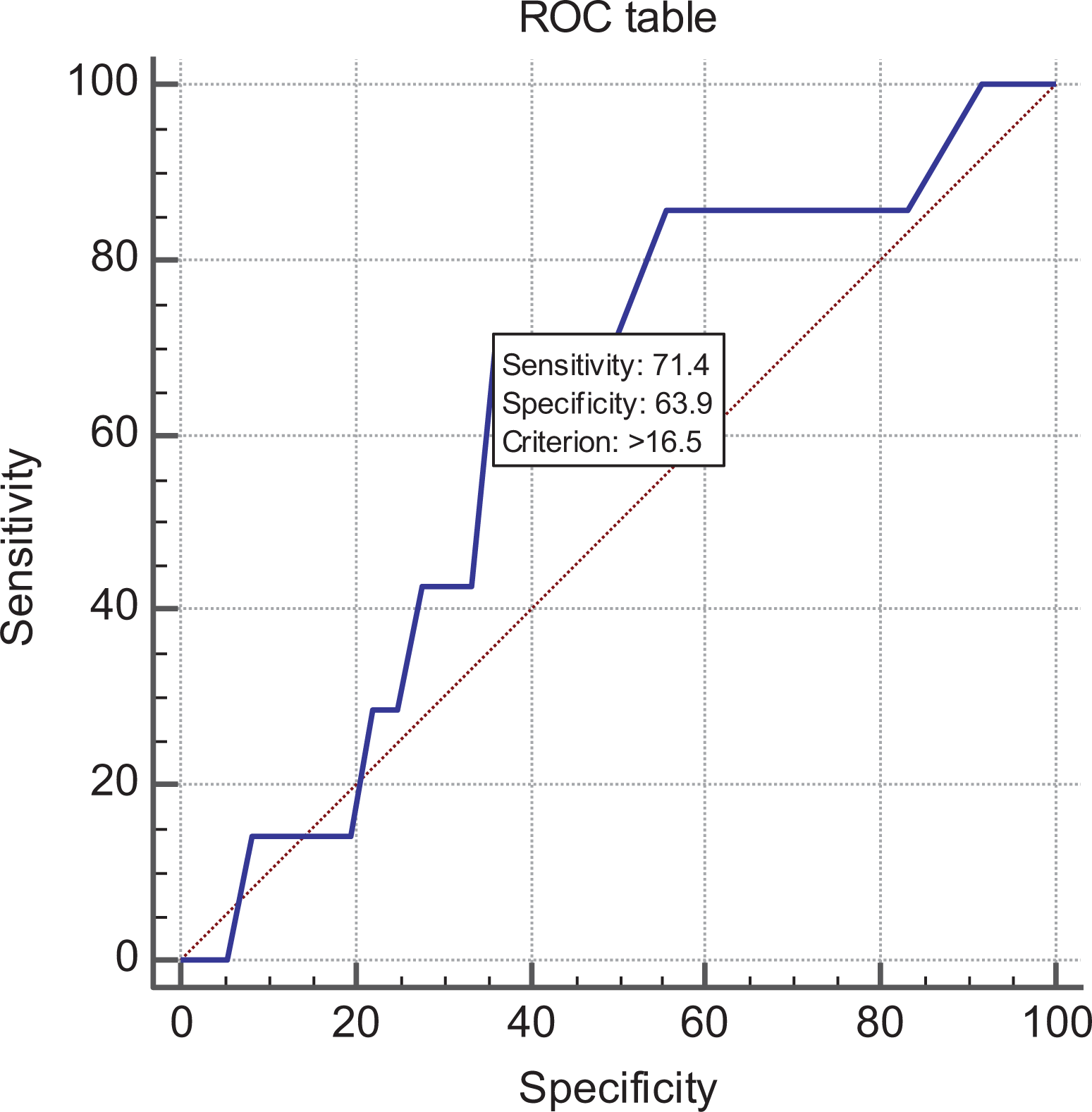
ROC curve for PSA with respect to contralateral progression. ROC: receiver operator coefficient; PSA: posterior sloping angle.
Discussion
A pre-study power calculation based on the work of Phillips et al. 15 suggested a sample size of 24 with an α of 0.05 and a β of 0.20. In this series, we collected a total sample size of 43 with 7 in the Subsequent Contralateral Progression group and 36 in the Isolated Unilateral Slip group. There was a trend toward a higher average PSA in the Subsequent Contralateral Progression versus Isolated Unilateral Slip groups (17.9° vs. 15.8°) but the difference was not found to be significant in contrast to previous literature.
The characteristics of patients within this series were virtually identical to a previous series published in 2008 by Lim et al. 18 on a series of Singaporean patients who had their data collected from 1997 to 2006. On comparing the data, the two series had similar age ranges (6–15 vs. 6–15), sex distribution (72.1% male and 27.9% female vs. 75% male and 25% female), slip rates (initial bilateral slips 8.8% vs. 10.4%, subsequent slip rates 16% vs. 9.6%), and racial distribution (Chinese 30.2% vs. 33.3%, Malay 20.9% vs. 19.4%, Indian 41.8% vs. 44.4%, and others 7% vs. 2.77%). 18 The close concordance of data gives a high degree of confidence to the validity of this series within the country of publication and of Asian patients. Previous studies 2,19 have noted a racial distribution of SCFE which is higher in Blacks, Hispanics, and American Samoa. An apparent racial predisposition appears to exist by comparing the national ethnic demographics within Singapore 20 and the distribution of ethnicities within this study (Chinese 76.2% vs. 30.2%, Malay 15.1% vs. 20.9%, Indian 7.4 vs. 41.8%, and others 1.4% vs. 7%). The largest deviation occurs within the Indian community which is 5.6 times overrepresented while the Chinese are underrepresented at 0.43. The reason for this racial disparity is unclear and may be subject to further study.
The average PSA value in the Isolated Unilateral Slip and Subsequent Contralateral Progression groups as well as the PSA delta between the two groups were close to previous published values as summarized in Table 2.
Comparison of data from existing literature on PSA and SCFE.

PSA: posterior sloping angle; SCFE: slipped capital femoral epiphysis; IUS: Isolated Unilateral Slip; SCP: Subsequent Contralateral Progression; NNT: number needed to treat; SD: standard deviation.
a When not explicitly stated, age data were replicated for both fields.
b Park et al. is a case control study with no incidence data.
c ± SD or (Range).
Within the four earlier publications that reported an association between increased PSA and contralateral slip, Park et al. 8 described an anomaly. Despite reporting that PSA was significantly associated with subsequent contralateral slip with p = 0.001, further subgroup analysis within the same study saw the relationship only hold true for females (p < 0.0001) but not males (p = 0.18) after division by gender. This was despite having similar numbers of male and female patients in each limb (males: unilateral slip n = 24, contralateral progression n = 27; females: unilateral slip n = 27, contralateral progression n = 24.) Other than a statistically significant but marginally younger population of females versus males (10.7 vs. 11.9 years), the authors could not account for the discrepancy.
Further literature review uncovered one additional publication and a poster presentation, which did not show any significant difference for PSA values. Boyle et al. published a large series of 168 patients which concluded that the α angle was a predictor of contralateral slippage. Although neither stated in the title nor abstract, the authors analyzed the PSA value in a similar fashion to this study and found that it did not significantly predict contralateral slippage (p > 0.1) despite the much larger sample size. 21
Kwiatkowska et al. presented a poster at the European Congress of Radiology 2014 using a similar methodology to our study. His team analyzed 76 patients and did not find a statistical significance (p = 0.21) for PSA values. He also noted a positive trend for PSA with Subsequent Contralateral Progression subjects having an average PSA of 17° versus 13° in the Isolated Unilateral Slip group. 22 Kwiatkowska’s findings mirror our own experience and highlight the possibility of publication bias overstating the significance of PSA. Brief scientific titles and abstracts may also keep “insignificant” values buried from notice while solely promoting positive and “significant” findings. Searching PubMed with the search terms such as “PSA & SCFE”, “PSA & SCFE progression”, and “PSA & prophylactic fixation” consistently yielded articles with only positive headlines. The correlation between PSA and the progression of contralateral slip requires further study in light of the evidence presented in this study and past literature.
We found that all patients had sufficient radiographs despite the retrospective nature of this study. A potential adoption of contralateral PSA measurements should therefore not add any additional radiation, cost, or hassle to patients as the relevant radiograph is currently already performed for other reasons and the PSA value can be obtained opportunistically. The two researchers exhibited an inter-observer ICC of 0.89 (good–excellent) which was higher compared to the previously reported value of 0.83 by Zenios et al. between two senior surgeons. 13
The post hoc power calculation resulted in a power of 20.3% due to the low proportion of the Subsequent Contralateral Progression group. While the possibility of a type II error due to an insufficient sample size is large, crucially, it is the author’s view that PSA values, even if shown to be significantly associated with contralateral progression, would nevertheless remain unsuitable as an isolated treatment threshold for the decision to perform prophylactic contralateral pinning.
This is due to three main criticisms. There was a very low delta between the mean PSA values of Isolated Unilateral Slip and Subsequent Contralateral Progression groups, which averaged a mere 4.08° in the studies quoted. 8,11,13 –15 The standard deviation (variance) in PSA values found in our study and others ranged between 4° and 6° which was larger than the PSA delta. Lastly, the absolute range of values in the Isolated Unilateral Slip group completely overlapped and encompassed the Subsequent Contralateral Progression group resulting in a very poor NNT as shown in Figure 3.
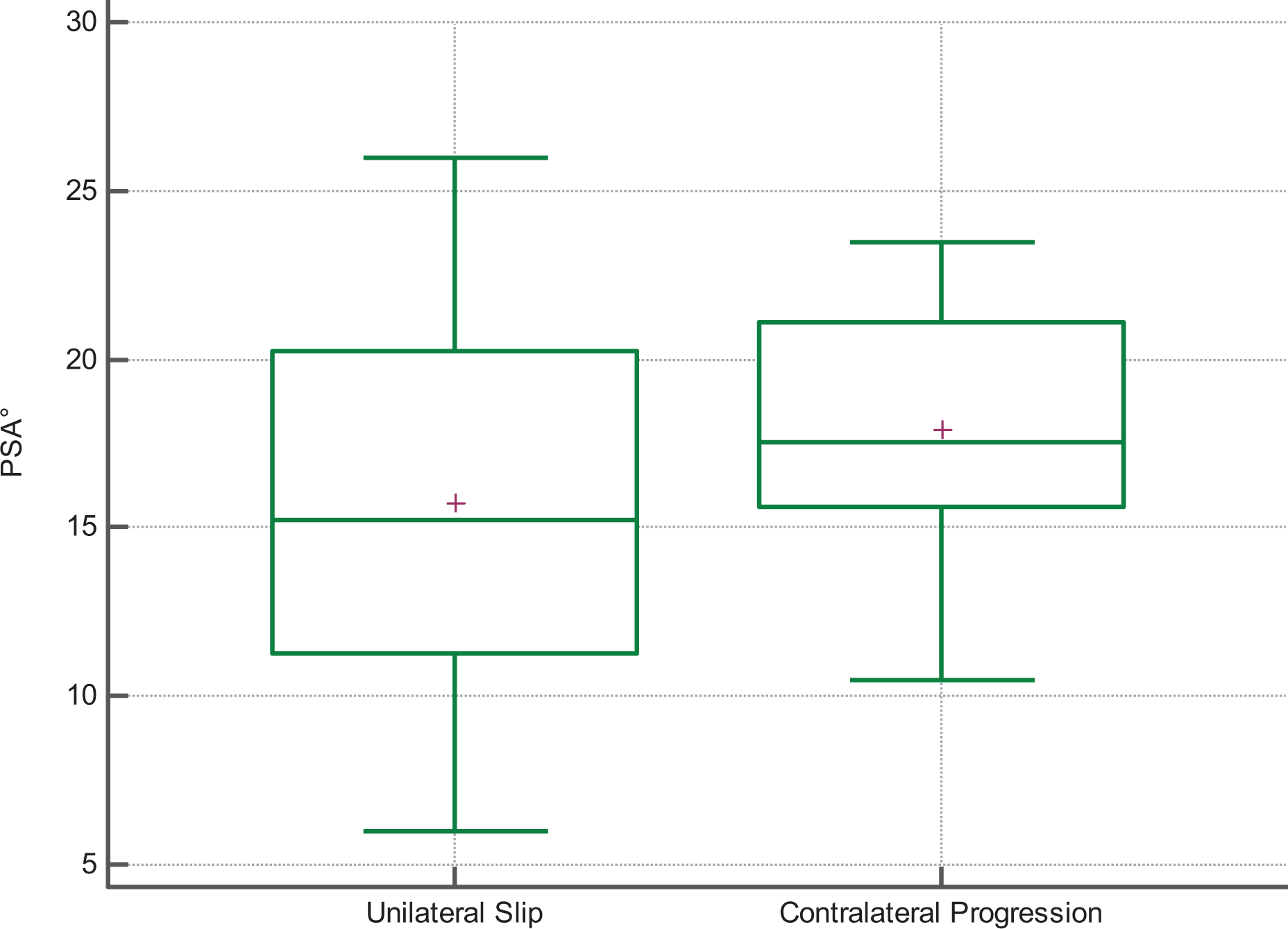
Box and whisker plot of PSA. The average PSA value is marked with the symbol +. PSA: posterior sloping angle.
To the author’s knowledge, this is the first study on the Asian population to address PSA in SCFE. The strength of our study lies in the minimum of 18 months of clinical and radiological follow-up. The measurement of the PSA was conducted by two independent researchers and exhibited a high degree of reliability. The point of radiographic evaluation replicated the clinical scenario faced by a surgeon planning prophylactic pinning. The thorough review pools all existing literature on PSA in SCFE and demonstrates the futility of adopting PSA measurements as an isolated marker of progression.
While our study sample size was limited, we are confident that this retrospective analysis has demonstrated that PSA measurement has poor clinical utility in guiding prophylactic surgical fixation in the Asian context. As body mass index data were not available, we were unable to analyze the effect of obesity on the subsequent progression to contralateral slip though other risk factors such as atypical SCFE, age of onset, and gender were accounted for. Despite the 18-month follow-up which would account for 82% of early contralateral slips, Hägglund et al. 23 have reported that up to 40% of patients could continue to develop late contralateral slips at a follow-up of 16–66 years. The inability to analyze contralateral slips at a much later date remains a limitation.
Conclusion
Despite the ease of access and good inter-observer reliability of the PSA measurement, comparable PSA values and predicted treatment thresholds to previous literature, PSA differences between the Subsequent Contralateral Progression and Isolated Unilateral Slip groups did not achieve statistical significance in this series. All proposed treatment thresholds had poor specificity and led to higher NNTs compared to previous literature (3 vs. 1.79–2.2). Crucially, the PSA value had a low delta between Subsequent Contralateral Progression and Isolated Unilateral Slip groups, exhibited high levels of variance, with the range of values in the Isolated Unilateral Slip group encompassing the Subsequent Contralateral Progression group. The PSA appears to have poor clinical utility.
Within the Asian population, the authors recommend that the decision to pin the contralateral hip should not be based on PSA treatment thresholds due to potential unnecessary surgery and costs. Surgical teams considering prophylactic pinning of the contralateral hip should factor in all available information including other radiographic measurements, clinical features, and patient preferences in multifactorial decision analysis models.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.