
Abstract
Purpose:
To evaluate how the accuracy of coronal-plane bone cutting and operative time may be affected by the experience of navigated total knee replacement (TKR) in starters of manual TKR.
Methods:
We analyzed 30 cases of navigated TKR performed in the early years (group 1), 30 consecutive cases of navigated TKR performed after experiencing more than 100 cases of navigated TKR (group 2), and the initial 30 consecutive cases of manual TKR (group 3). Postoperative mechanical hip-knee-ankle (mHKA) angle, mechanical medial proximal tibial angle (mMPTA), and mechanical lateral distal femoral angle (mLDFA) were measured. Bone cutting was aimed at mHKA angle of 0°, mMPTA of 90°, and mLDFA of 90°. We have set the tolerance of absolute value of errors in mHKA angle, mMPTA and mLDFA as 0 ± 3°. Comparative analysis of tourniquet times have been performed.
Results:
Postoperative absolute error values of mHKA angle, mMPTA, and mLDFA were 2.78 ± 3.53°, 1.06 ± 1.91°, and 1.44 ± 1.90° in group 1; 1.18 ± 1.32°, 1.20 ± 1.49°, and 0.98 ± 1.09° in group 2; and 2.11 ± 2.49°, 1.35 ± 0.62°, and 1.92 ± 2.85° in group 3. Tourniquet times were 67.50 ± 21.50 min in group 1, while group 2 and group 3 showed tourniquet times of 51.87 ± 12.00 and 52.00 ± 15.00 min, respectively.
Conclusion:
In starters of manual TKR, previous experience of performing navigated TKR may help the error values during femoral and tibial bone cutting to fall within the values similar to the median error value of navigated TKR. It may also help to reduce the operative time of manual TKR similar to the operative time of and experienced surgeon with over 100 cases of navigated TKR.
Introduction
Total knee replacement (TKR) is a surgical procedure with one of the highest patient satisfaction in the field of orthopedic surgery. 1 As life expectancy increases, implant survival has become a major concern in TKR. Computer-assisted navigation has been developed to obtain optimal coronal plane alignment, which is thought to be crucial for long-term survival. 2,3 However, there are still debates about the benefits of computer navigation. 4 –7 Most of the authors who claim that computer-navigated TKR is not superior to manual TKR are surgeons experienced in manual TKR, who have already acquired the potential benefits of computer navigation. 7,8 On the other hand, studies about the benefits of computer-navigated TKR for starters of manual TKR are few in number. Accordingly, from a surgeon with experience of over 100 cases of computer-navigated TKR, we analyzed the differences in accuracy of coronal plane bone cutting and operative time between the first 30 manual TKR cases of the surgeon and his previous computer-navigated TKR cases. We tried to evaluate how the experience of computer-navigated TKR would affect the accuracy of coronal plane bone cutting and operative time in starters of manual TKR. We assumed that the experience of computer navigation TKR would help a surgeon with no experience of manual TKR to have similar bone cutting accuracy and operative time with those of computer navigation TKR. The Institutional Review Board of Daegu Catholic University approved the study (CR-19-070).
Methods
The surgeon
The single surgeon has performed more than 100 cases of computer-navigated TKR from 2016 (when staring TKR) to 2018. Manual TKR has not been performed by the surgeon during that period, and the surgeon has started to perform manual TKR since March 2019.
Participants
Patients who have underwent TKR by a single surgeon in a single center due to knee joint osteoarthritis were enrolled for the study. Patients who underwent TKR due to other conditions than osteoarthritis, and revision TKR cases were excluded from the study. We analyzed the surgical outcomes of 30 consecutive cases of computer-navigated TKR performed in the early years (group 1), 30 consecutive cases of computer-navigated TKR performed after experiencing more than 100 cases of computer-navigated TKR (group 2), and the initial 30 consecutive cases of manual TKR (group 3). Retrospective analysis of group 1 and group 2, and prospective analysis of group 3 was done.
Surgical procedure
Computer navigation-assisted TKR
The Imageless navigation system version 2.6 (BrainLAB, Feldkirchen, Germany) was used in all cases (Figure 1). Nexgen (Zimmer, Warsaw, Indiana, USA), a cemented posterior cruciate ligament substituting implant, was used in all cases. Measured gap technique was used in bone cutting.
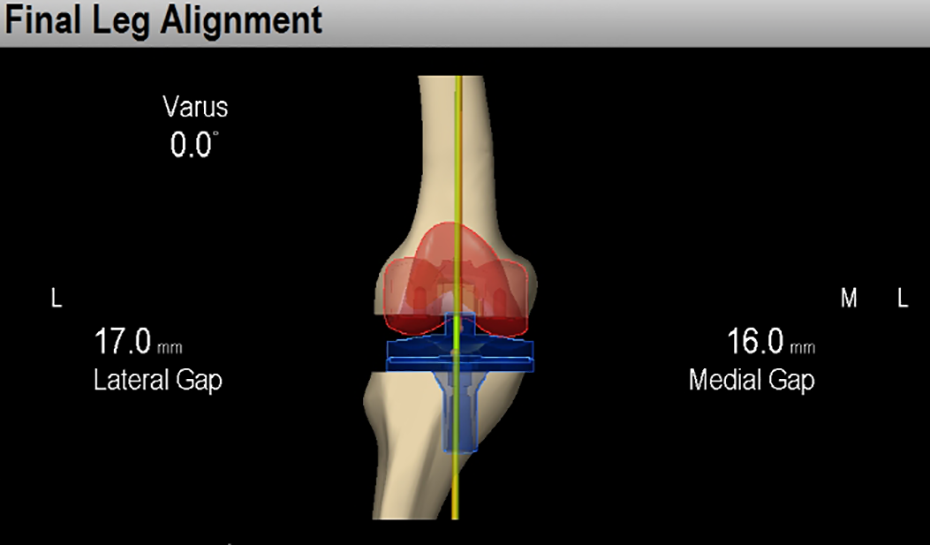
The imageless navigation system version 2.6 (BrainLAB) was used in groups 1 and 2. The surgeon can see the coronal angle through screen.
Manual TKR
Nexgen (Zimmer, Warsaw, Indiana, USA), a cemented posterior cruciate ligament substituting implant, was used in all cases. Measured gap technique was used in bone cutting. The distal femoral valgus cut was made using an intramedullary guide and was aimed at the angle difference between the mechanical axis and the anatomical axis of the femur measured on the preoperative scanogram. Using an extramedullary guide, the tibial bone cutting was made perpendicular to the mechanical axis of the tibia.
Measurement
In all groups, radiographic severity of knee osteoarthritis was classified according to the Kellgren–Lawrence grading scale preoperatively. Mechanical hip knee ankle (mHKA) angle, mechanical medial proximal tibial angle (mMPTA), and mechanical lateral distal femoral angle (mLDFA) were measured on the preoperative scanogram. 9
The accuracy in bone cutting of the three groups were assessed by measuring mKHA angle, mMPTA, and mLDFA on scanograms taken 1 month after surgery. Mechanical HKA angle of 0°, mMPTA of 90°, and mLDFA of 90° were the targets for optimal coronal plane bone cutting. Tolerance of the absolute value of errors in mHKA angle, mMPTA, and mLDFA was set as 3°. 6 Comparative analysis of tourniquet times, as proxy for operative times, has been performed among the three groups.
Statistical analysis
The Kruskal–Wallis nonparametric test was used to analyze the three groups, and the Mann–Whitney test was used to compare differences between two groups. All values were shown as the median ± quartile (mean ± standard deviation). A p-value of less than 0.05 was considered to indicate statistical significance. All analyses were performed with the use of IBM SPSS Statistics ver. 19 (IBM Corp., Armonk, New York, USA).
Results
Epidemiology
No significant differences among groups in age, body mass index, preoperative mHKA angle, mMPTA, and mLDFA were found at baseline (Table 1).
Epidemiology of all participants.
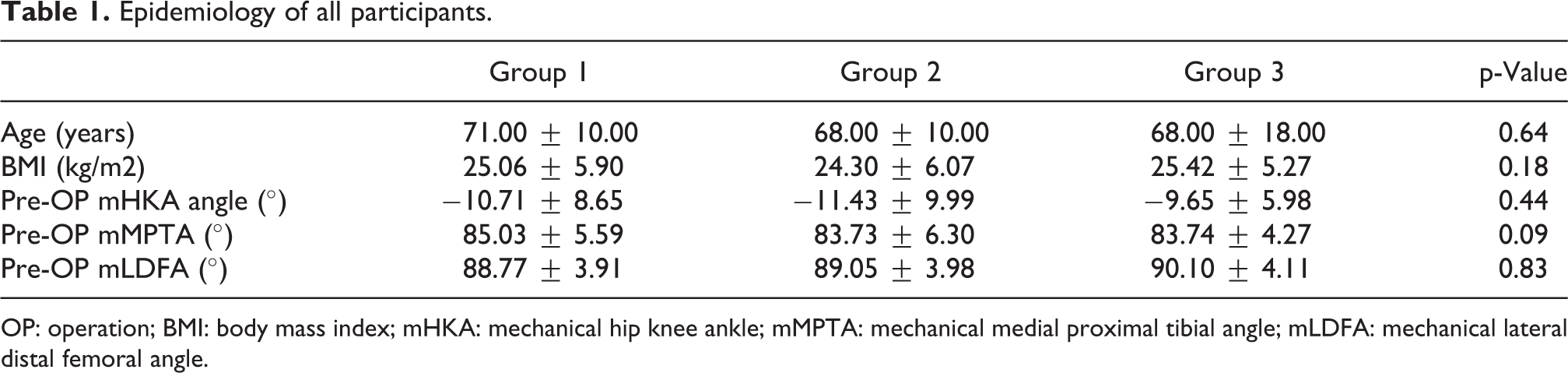
OP: operation; BMI: body mass index; mHKA: mechanical hip knee ankle; mMPTA: mechanical medial proximal tibial angle; mLDFA: mechanical lateral distal femoral angle.
Radiographic measurement
Postoperative values of mHKA angle, mMPTA, and mLDFA measured on scanograms taken 1 month after surgery were −1.47 ± 3.57°(−1.40 ± 2.79°), 89.68 ± 2.49°(89.74 ± 1.80°), and 91.00 ± 2.20°(91.21 ± 1.51°) in group 1; 0.63 ± 2.42°(−0.25 ± 2.08°), 90.35 ± 2.21° (90.23 ± 1.88°), and 90.84 ± 1.38°(90.77 ± 1.16°) in group 2; and −1.91 ± 4.03°(−1.51 ± 4.79°), 89.93 ± 2.66°(89.92 ± 2.15°), and 91.92 ± 3.40°(91.68 ± 1.70°) in group 3. Postoperative absolute error values of mHKA angle, mMPTA, and mLDFA, which were measured on the same scanograms, were 2.78 ± 3.53°(2.43 ± 1.93°), 1.06 ± 1.91°(1.42 ± 1.09°), and 1.44 ± 1.90°(1.50 ± 1.21°) in group 1; 1.18 ± 1.32°(1.67 ± 1.24°), 1.20 ± 1.49°(1.20 ± 0.68°), and 0.98 ± 1.09°(1.14 ± 0.79°) in group 2; and 2.11 ± 2.49°(2.23 ± 1.42°), 1.35 ± 0.62°(1.25 ± 0.52°), and 1.92 ± 2.85°(1.89 ± 2.11°) in group 3. No significant differences in absolute error values of mHKA angle, mMPTA, and mLDFA were found among the three groups (Table 2).
Differences in absolute error values of mHKA angle, mMPTA, and mLDFA were found among the three groups.

mHKA: mechanical hip knee ankle; mMPTA: mechanical medial proximal tibial angle; mLDFA: mechanical lateral distal femoral angle.
Outlier of bone cutting
In terms of outliers, which have exceeded the tolerance of absolute error values, outliers of mHKA angle, mMPTA, and mLDFA were 16 of 60 (26.7%), 4 of 60 (6.7%), and 5 of 60 (8.3%) in computer-navigated TKR cases (group 1 and group 2) and 9 of 30 (30%), 0 of 30 (0%), and 8 of 30 (26.7%) in manual TKR cases (group 3). The manual TKR group had a significantly higher probability of outliers in mLDFA than did the computer-navigated TKR group (p = 0.03) (Table 3).
Outlier of bone cutting (femur side).

LDFA: lateral distal femoral angle.
Operative time
Tourniquet times were 67.50 ± 21.50 (69.5 ± 11.74) min in group 1, 51.87 ± 12.00 (51.50 ± 7.41) min in group 2, and 52.00 ± 15.00 (52.86 ± 10.80) min in group 3. Group 1 had a significantly longer tourniquet time than did groups 2 and 3 (p < 0.01).
Discussion
Theoretically, compared to manual TKR, computer-navigated TKR allows more precise bone cutting and optimal coronal plane alignment. 2 However, the usage of computer-assisted navigation in clinical settings remains controversial. However, if we take a look on the study designs of existing data, most of the cases were performed by senior surgeons with a volume of experience in manual TKR, who have already acquired the potential benefits of computer navigation. 7,8 Accordingly, from a surgeon with experience of over 100 cases of computer-navigated TKR but with no experience of manual TKR, we analyzed the differences in accuracy of coronal plane bone cutting and operative time between the surgeon’s first 30 cases of manual TKR and his previous computer-navigated TKR cases. We tried to evaluate how the experience of computer-navigated TKR would affect the accuracy of coronal plane bone cutting and operative time in starters of manual TKR.
In our study, there were no significant differences in absolute error values of mHKA angle, mMPTA, and mLDFA among all groups. Based on the result, we may assume that the initial use of computer-navigated TKR would allow bone cutting to have no significant difference with those of after experiencing 100 cases of computer-navigated TKR. We may also assume that the previous experience of performing computer navigation would allow to have similar accuracy of bone cutting when starting TKR without computer navigation.
However, since we have compared the median error values of bone cutting, we have analyzed the outlier values after setting the tolerance of absolute value of errors in mHKA angle, mMPTA, and mLDFA as 3°. The manual TKR group had a significantly higher probability of outliers in mLDFA than did the computer-navigated TKR group. However, there were no outliers in mMPTA in the manual TKR group. The reason for this may be due to two reasons: there is no way to confirm alignment after inserting the intramedullary guide during femoral cutting, and a particularly high incidence of femoral bowing in Asians, 10 which makes it difficult for surgeons to insert the guide accurately.
Computer navigation may delay operative time due to the additional process of registration, 11 and manual TKR may induce latency while applying the rod during bone cutting. There were no significant difference in operative time between group 2 and group 3. The time duration required to complete the process of registration during computer-navigated TKR may be similar to the time required to apply the rod during manual TKR, thus making no difference in operative times.
Our study has limitations. First, we have obtained data from only 30 cases. Larger sample size would be needed to generalize. Secondly, results were obtained from cases performed by a single surgeon, and due to potential singularity of the surgeon, there is possibility of error.
Conclusion
In starters of manual TKR, previous experience of performing computer-navigated TKR may help the error values during femoral and tibial bone cutting to fall within the values similar to the median error value of computer-navigated TKR. It may also help to reduce the operative time of manual TKR similar to the operative time of and experienced surgeon with over 100 cases of computer-navigated TKR. However, due to significantly higher probability to exceed the error tolerance during femoral bone cutting, great care is needed for surgeons starting manual TKR during femoral bone cutting.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.