
Abstract
Background:
Navigation is associated with improved accuracy in alignment. However, its influence on clinical outcome is inconclusive. The aim of this study was to compare the component alignment and functional outcome in patients undergoing navigation-assisted and conventional total knee replacement (TKR).
Materials and method:
A prospective randomized study consisting of two groups (group A and group B) was carried out. Group A consisted of patients undergoing TKR using conventional jig-based method, whereas group B consisted of patients undergoing TKR using computer navigation-assisted method. We measured and compared the coronal and sagittal plane alignment in X-ray and rotational alignment in computed tomography scan between both groups. Functional outcome was analysed using Knee Society Score (KSS) and Western Ontario and McMaster University scale (WOMAC) score.
Results:
A total of 50 patients were randomized into two groups A and B each with 25 patients. Navigation was associated with more accuracy in mechanical axis alignment (p = 0.011) and femoral component rotation (p = 0.033). The mean follow-up was 4.6 years (range 48–62 months). There was no statistically significant difference between the groups with respect to KSS and WOMAC score at the minimum follow-up of 4 years.
Conclusion:
We concluded that even though navigation-assisted system is associated with better accuracy, there was no difference in clinical outcome at an average follow-up of 4.6 years.
Keywords
Introduction
Total knee replacement (TKR) is a common surgical procedure done for severe knee joint degeneration and arthritis. 1 It has proved its effectiveness in relieving pain and improving function resulting in a better quality of life in patients affected with osteoarthritis. 2 The primary intent of TKR surgery is to bestow accurate alignment of the prosthetic components and the limb, stability of the knee and attainment of sufficient range of motion. 3 One of the five patients undergoing TKR is not satisfied with the surgical outcome. 4 The reason for this dissatisfaction is multifactorial and cannot be attributed to a single cause. One of the important causes for failure is inaccurate implant positioning. 5 The deviations of mechanical axis (MA) greater than 3° from the normal neutral alignment have been correlated with worsening of clinical outcomes, abnormal wear, premature loosening and early implant failure. 6
The failure of conventional total knee replacement (CTKR) to achieve within ±3° of the MA accounts for more than 30% of the TKR being unable to produce the desirable results, as reported by Mason et al. 7 The drawbacks of conventional alignment systems include difficulty with identifying anatomical landmarks intraoperatively as well as the assumption of standard anatomical relationships, which may not always be consistent across all patients. 7
Several previous randomized control trials and nonrandomized studies have demonstrated improved accuracy of alignment after navigation-assisted total knee replacement (NATKR) but failed to show any difference in functional outcome as compared with CTKR. 8,9 This study intended to compare the component alignment as well as functional outcome of patients following CTKR and NATKR.
Materials and method
Patients undergoing unilateral TKR between May 2012 and March 2013 were enrolled in this prospective randomized control study. After obtaining institutional ethical review board approval, computer-generated randomization sequence was used to randomize 50 patients. By using sealed envelope, patients were allocated into one of the two groups, group A (CTKR) and group B (NATKR), each with 25 patients (Figure 1). Informed written consent was taken from all the allocated patients. Outcome assessors were blinded, and all the patients were instructed not to reveal their treatment group.

CONSORT flow chart. CONSORT: Consolidated Standards of Reporting Trials.
The inclusion criteria were an adult patient diagnosed with knee osteoarthritis and suitable for unilateral TKR. The exclusion criteria were patient undergoing simultaneous hip and knee replacement, bilateral TKR, and morbid obesity (body mass index (BMI) > 40 kg/m2).
The preoperative evaluation included a collection of demographic data consisting of age, sex, BMI, diagnosis, side of pathology and knee range of motion and scores (Knee Society Score (KSS) and Western Ontario and McMaster University scale (WOMAC) score).
Post-operative evaluation was done based on patients’ clinical and radiological parameters, which was carried out in the outpatient department at predetermined intervals. The first follow-up period was scheduled 2 weeks post-surgery followed by 6 months, 1 year, 2 years, 4 years and then final follow-up in May 2017.
The clinical evaluation was done using KSS and WOMAC scores. The radiological evaluation was done by X-rays (which included a full-length standing scanogram, anteroposterior and lateral views of the knee) and computed tomography (CT) scan of the knee. The following angles were measured on the radiographs: MA, frontal femoral angle (FFA), frontal tibial angle (FTA), sagittal femoral angle (SFA) and sagittal tibial angle (STA). Femoral component rotation (FCR) was measured in axial CT scan.
Orthopilot Imageless Navigation system (OrthoPilot; Aesculap, Germany) was used in all the NATKR in group B, whereas conventional jigs were used in group A. All the surgeries were performed by a single surgeon (RM). The surgical approach was medial parapatellar, and the implant used was Columbus (cruciate retaining; Aesculap B Braun Tuttlingen, Germany) in both groups. The femur and tibia were implanted with bone cement (Palacos; Heraeus Kulzer GmbH, Germany) in all patients. Enoxaparin sodium (40 mg) was given subcutaneously once daily and elastic stockings were used for thromboprophylaxis.
FFA is the medial angle between the MA of the femur and intercondylar line, and FTA is the medial angle between the MA of the tibia and the line parallel to the tibial tray. Both were measured in full-length weight-bearing X-ray (Figure 2(a)).

(a) Showing MA of 0°, FFA (medial angle between the MA of the femur and intercondylar line) of 90° and FTA (medial angle between the MA of the tibia and the line parallel to the tibial tray) of 90° in group B patient. (b) Showing SFA (posterior angle between the longitudinal axis of femur and slope of distal femoral cut) of 91° and STA (posterior angle between posterior tibial cortex and slope of the proximal tibial cut) of 91° in group B patient. (c) Showing axial CT scan of distal femur with FCR of 1° external rotation in relation to surgical epicondylar axis in group B patient. MA: mechanical axis; FFA: frontal femoral angle; FTA: frontal tibial angle; SFA: sagittal femoral angle; STA: sagittal tibial angle; FCR: femoral component rotation.
SFA is a posterior angle between the longitudinal axis of femur and slope of distal femoral cut, and STA is a posterior angle between the posterior tibial cortex and the slope of the proximal tibial cut. Both the sagittal angles are measured in lateral knee X-ray (Figure 2(b)). The normal range of all the above-mentioned angles is between 87° and 93°. 10
FCR is an angle between the posterior condylar line and the surgical epicondylar axis of femur measured in axial CT scan (Figure 2(c)). FCR of −3° (internal rotation) to +3° (external rotation) is considered well aligned. 10,11
Modified KSS (modification by Insall et al. in 1993) was used for clinical evaluation, which included knee score and functional score, each has maximum score of 100. 12
WOMAC score consists of 24 questions focusing on pain, stiffness and physical function.
Each question has the grading score of 0–4, with maximum total score of 96 and minimum score of 0. Higher the score, worser will be the pain, stiffness and function. 13
Statistical analysis
A descriptive analysis was done. The inter-group comparison was evaluated using the χ 2 test. The Student’s t-test was done to capture the differences in preoperative and post-operative values of knee score, functional score, WOMAC score, FFA, FTA, STA, SFA, FCR and MA between the groups.
Results
There was no difference found between the two groups in age, sex, diagnosis, side to be operated and BMI (Table 1). One patient in group B had superficial wound infection at 11th post-operative day which was managed by wound wash and the patient completely recovered after that. The follow-up period ranged from 48 months to 62 months with a minimum follow-up of 4 years. None of the patient required revision.
Demographic data.

BMI: body mass index.
The mean FFA in group A was 89.88° (range 87–92°). Mean FFA in group B was 89.40° (range 88–91°). There was no statistically significant difference between two groups (p = 0.213). The mean FTA in group A was 89.28° (range 87–92°). Mean FTA in group B was 89.96° (range 89–91°). There was a statistically significant difference between the two groups (p = 0.040). The mean SFA in group A was 89.04° (range 86–92°). Mean SFA in group B was 89.64° (range 88–91°). There was no statistically significant difference between the two groups (p = 0.146). The mean STA in group A was 89.56° (range 86–92°). Mean STA in group B was 90.04° (range 89–92°). There was no statistically significant difference between the two groups (p = 0.243).
The mean MA of group A was 1.08° varus (range 2° valgus to 3° varus). Mean MA of group B was 0.480° varus (range 2° valgus to 2° varus). The restoration of MA was more accurate in group B with a statistical significance value (p = 0.011).
The mean FCR in group A was 2.64° external rotation (range 3° internal rotation to 5° external rotation). Mean FCR in group B was 1.80° external rotation (range 2° internal rotation to 4° external rotation). Group B patients had more precisely positioned femoral component in relation to transepicondylar axis (p = 0.033).
Figures 3 and 4 depict the distribution of patients in the two study groups according to FCR and MA, respectively.

Rotational alignment of the femoral component in relation to the transepicondylar axis. Negative values indicate internal rotation of the component relative to the surgical transepicondylar axis, and positive values indicate external rotation.

Distribution of patients in groups A and B according to their MA. MA: mechanical axis.
Mean preoperative knee score in groups A and B was 26.5 and 27.7, respectively, which improved post-operatively to 81 and 82 at the final follow-up.
Mean preoperative functional score in groups A and B was 28.20 and 27.40, respectively, which improved post-operatively to 83 in both the groups at the final follow-up.
Mean preoperative WOMAC score in groups A and B was 58.20 and 58.24, respectively, which improved post-operatively to 16.5 and 16 at the final follow-up.
We could not find statistically significant difference between two groups in clinical outcome at the minimum follow-up of 4 years.
The comparison of knee score, functional score and WOMAC score between groups A and B is given in Table 2.
Clinical preoperative and post-operative knee score, functional score and WOMAC score in groups A and B.
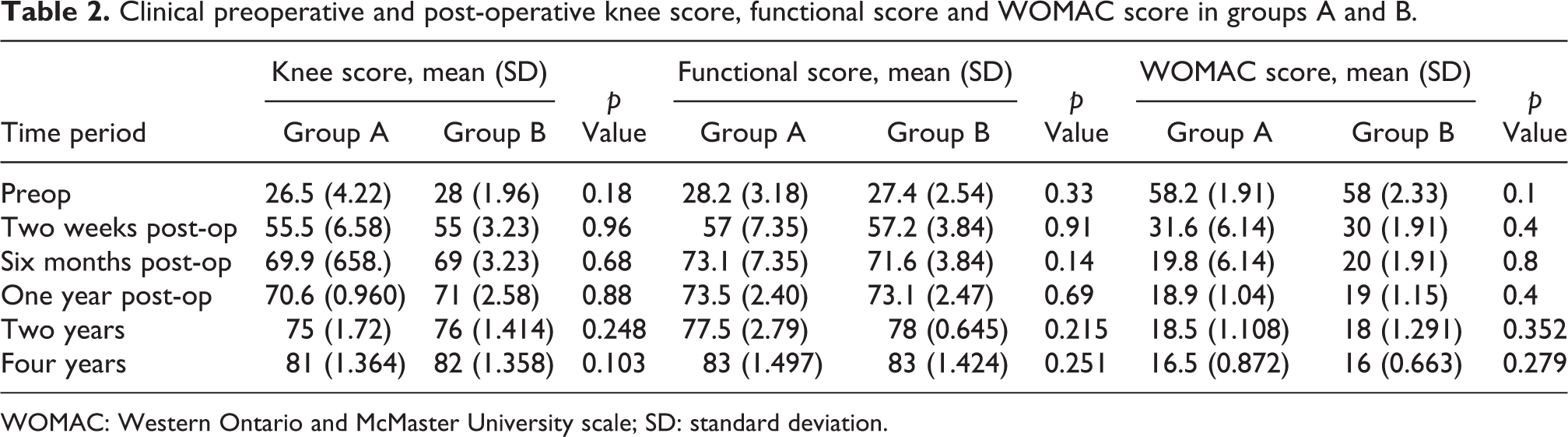
WOMAC: Western Ontario and McMaster University scale; SD: standard deviation.
Discussion
In this study, we found that the MA and FCR were more accurately restored in patients undergoing NATKR as compared to CTKR. However, clinical parameters like the knee score, functional score and WOMAC score in both groups were similar at the final follow-up.
The restoration of a neutral mechanical alignment in the coronal plane plays a pivotal role in the success of the TKR for improved functional and clinical outcome. In the present study, the 0° alignment of the MA was achieved in 40% of patients who underwent NATKR compared to 24% in CTKR (Figure 4). However, there were no outliers in both groups; all the patients in both groups achieved less than 3° MA. It has also been reported by Mason et al. and Hetaimish et al. that navigated TKR significantly improved prosthesis alignment. 7,14 Hetaimish et al. additionally found that 30.1% of patients in the conventional group had deviations in the coronal plane greater than 3° from neutral compared to 12.8% in the navigation cohort. Blakeney et al. reported a significantly better Oxford Knee Score for navigated knee arthroplasty in which MA alignment was within 3° of neutral. 15
Hoffart et al. 16 have reported that the precision in rotational alignment was the single predominant factor to achieve better KSS at 5 year follow-up after navigated surgery.
In our study, the FCR was 0° in 4 of 25 (16%) NATKR cases and 1 of 25 (4%) cases in CTKR; 17 of 25 (64%) CTKR cases and 18 of 25(78%) NATKR cases were within 3° in FCR. The number of outliers (>3° FCR) was more in CTKR compared to NATKR but without statistical significance.
There was no significant difference found between two groups in FFA, FTA, SFA and STA. The clinical outcomes measured with knee score, functional score and WOMAC score did not show any considerable difference between both groups at 4-year follow-up; Kim et al. also could not find differences in KSSs between the CTKR and the NATKR groups. 17 Cip et al. showed an improvement in Insall Knee Score and HSS Knee Score with computer-assisted technique, but no improvement in WOMAC scores. 18 Hoffart et al. reported improved KSSs for navigated TKRs, which may be attributed to a larger sample size. 16 Many studies found no significant difference in satisfaction, pain or quality of life outcome; however, this conclusion is somewhat heterogeneously reported. 19,20
Neutral MA plays a very pivotal role in the success of longevity of an implant prosthesis and validates post-surgical clinical and functional outcomes.
The long-term survival of TKA after navigation-assisted versus conventional instrumentation was characterized in a study by de Steiger et al., in which an overall lower rate of revision and decreased revision rate for loosening or lysis was found in the navigation group. 21 In the current study, there was no loosening of prosthesis found till 4 years of follow-up, and so revision was not required for any of the patient in both groups.
A small sample size and short-term follow-up were limitations of this study. However, the major strength was its prospectively randomized study design with standardized operative protocol, implant and uniform perioperative and post-operative management.
In our study, although MA and FCR were restored more accurately using navigation, there was no difference in FFA, FTA, SFA and STA. And also there was no difference in clinical outcomes using KSS and WOMAC scores.
In future, further long-term follow-up studies should be conducted over larger sample size and a single universally accepted scoring system should be developed to measure functional, clinical and radiological parameters for evaluating the success of TKRs, as every study reported till date measures different parameters under separate scoring systems.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.