
Abstract
Purpose:
For anterior spine column reconstruction after corpectomy, expandable cages offer solid anterior support and allow correction of deformity, providing excellent primary stability. To provide a larger body of clinical observations concerning the effectiveness of the approach, this retrospective study examines patients treated by corpectomy and reconstruction with an expandable cage for different pathologies.
Methods:
Across 5 years, 39 patients underwent vertebral reconstruction with expandable cages after single (n = 34), double (n = 4), or triple (n = 1) corpectomy. Pathologies were tumors (n = 21), fractures, or deformities in traumatic injuries (n = 14), degenerative pathology (n = 2), and infection (n = 2). Levels were cervical (n = 10), thoracic (n = 14), and lumbar (n = 15). All patients were evaluated clinically and radiographically.
Results:
There were no cases of neurologic deterioration. Nurick grade showed significant improvement at 3 months postoperative versus preoperative (p < 0.01). Visual analog scale significantly improved preoperatively versus 3 and 12 months postoperatively (both p = 0). Regional angulation was significantly corrected, from preoperative to 3 and 12 months postoperative, at cervical, thoracic, and lumbar levels. We achieved reconstruction of the normal local anatomy with full recovery of the height of the vertebral body. Six patients (15.4%) had complications and two (5.1%) underwent revision surgery.
Conclusions:
In our experience, expandable cages confer stable anterior support, providing significant improvement of the segmental kyphosis angle and restoration of the original somatic height. Our clinical results are favorable, and the low rate of complications and revision accentuates the expandable cage as a valuable tool to replace the vertebral body in diverse pathologies and different spine levels.
Introduction
Anterior spinal column can be damaged as a consequence of pathologies, such as fractures, metastases, infections, or deformities. In some cases, it is necessary to perform a corpectomy, a widely used and increasingly common procedure. 1 –7 Corpectomy of the cervical spine is performed through an anterior approach. 2,8 For the thoracolumbar spine, approaches include anterior-only, posterior-only, or double (anterior–posterior). The posterior-only approach has the advantage of reducing the surgical time and the complications related to the change of position of the patient, thus avoiding the morbidity of an anterior approach. 9 –12
To reconstruct the anterior column, a graft or implant device is needed. The most suitable replacement of the vertebral body should provide the following benefits: anterior support resistant to the axial load, correction of the deformity, primary stability, and an extended contact surface with the adjacent vertebral bodies to allow a rapid fusion preventing mobilization. 13
Different material mesh and stackable cages can be useful, but optimal placement of these cages is challenging, especially through a posterior approach. 7 To obviate these difficulties, expandable cages have been developed. These are titanium cylinders, whose height can be increased and adjusted in situ. In recent years, these devices have been used in multifarious situations. 4 –7,11,12,14 –16
In this retrospective study, we report our clinical and radiological results with 39 patients with various pathologies treated with a corpectomy at cervical, thoracic, or lumbar level and reconstruction with expandable cages.
The aim of this study is to assess the clinical efficacy of the use of expandable cages to reconstruct the anterior column at cervical, thoracic, or lumbar level and restore a physiological curve in diverse pathological situations.
Materials and methods
Patient population
From 2013 to 2018, a total of 39 consecutive patients (20 males and 19 females) underwent surgery of reconstruction of the vertebral body with expandable cages after corpectomy.
Mean age was 55 years (range 18–78 years). The preoperatory clinical exam showed myelopathy in 15 cases and radiculopathy in 10 cases. In 14 cases, there were no neurological deficits. In all cases, the patient complained of neck and/or back pain. The indication for corpectomy was instability, segmental deformity, or neural compression. The cause was a tumor in 21 cases, fractures or deformities consequent to traumatic injury in 14 cases, degenerative pathologies in 2 cases, and infection in 2 cases. In the 21 cases of neoplastic disease, the primary tumor was breast (n = 4), hematologic (n = 4; 3 myeloma and 1 lymphoma), kidney (n = 3), lung (n = 3), liver (n = 2), prostate (n = 1), neuroendocrine (n = 1), gliosarcoma (n = 1), malignant peripheral nerve sheet tumor (n = 1), and giant lytic schwannoma (n = 1). All tumors were lytic, in the vertebral body, sometimes with extension into the epidural space and with existing or impending spinal cord compression. In the 14 trauma cases (deformity: n = 9, acute fracture: n = 5), we performed a careful discectomy of the upper and lower discs adjacent to the fractured vertebral body. We then partially removed the vertebral body to allow adequate space for the cage. We inserted the cage and expanded it to obtain correction of the kyphosis. In the case of infection, the causes were tuberculosis (n = 1) and methicillin-sensitive Staphylococcus aureus in a diabetic, obese patient (n = 1); both were at the cervical level with clinical signs of spinal cord compression. They were treated with antibiotics as managed by infectious disease specialists.
We performed a single corpectomy in 34 patients, a double level corpectomy in 4 patients, and a triple-level corpectomy in 1 patient.
In 10 cases, the cages were used at the cervical level, in 14 cases at the thoracic level, and in 15 cases at the lumbar level.
Patient characteristics are summarized in Table 1.
Patient characteristics.

M: male; F: female.
We used the visual analog scale (VAS) 17 to evaluate the pain and the Nurick grading scale 18 to evaluate the neurological status.
Radiographic evaluation
All the patients underwent preoperative conventional X-rays and magnetic resonance imaging as well as postoperative X-ray at 3 and 12 months. The regional angulation was determined by measuring the angle between the cranial end plate above and the caudal end plate below the affected segment. Kyphosis was documented as positive angulation and lordosis as negative. Stability was determined from the absence of radiolucency around the hardware.
Surgical procedure
The anterior approach is standard for performing a corpectomy at the cervical level and pertained to all cases considered here, in some cases completed by posterior fixation. At the thoracic level, we used a lateral and posterior approach or posterior-only. At the lumbar level, the approach was lateral and posterior, posterior-only, lateral-only, or anterior-only. The mean duration of surgery was 392 min (range 190–700), the mean blood loss in cervical approaches was 125 mL (range 100–150), and the mean blood loss in thoracolumbar approaches was 1296 mL (range 400–3000).
To insert the cage by the posterior approach, it was necessary to make a wide opening laterally. At the thoracic level, a costotransversectomy was first performed and one nerve root was cut. For this reason, at the thoracic level, we always perform an angiography before surgery to determine the origin of the anterior spinal artery. At the lumbar level, the nerve root must be extensively released and then retracted caudally to allow cage insertion. The expandable cage was inserted obliquely and then rotated vertically and expanded. With any approach, it is essential to carefully prepare the end plates.
We used CAPRI® Expandable Corpectomy Cage System (K2 M, Inc., Leesburg, Virginia, USA) in 16 cases and X-CORE® (NuVasive®, Inc., San Diego, California, USA) in 23 cases. The cage and surrounding space were filled only with β-tricalcium phosphate osteoconductive paste in patients with tumor or infection, whereas in the remaining cases, they were additionally filled with autologous bone.
Statistical analysis
Results are presented as the mean ± standard deviation. Two-tailed paired t-tests were used to compare pre- and postoperative Nurick grades, VAS values, and regional angulations. Because the paired t-test compares pre- and postoperative values, it cannot be applied in case of mortality before the scheduled postoperative evaluations, and those cases were omitted from the test. A p-value less than 0.05 was considered statistically significant. Statistical analyses were performed with Microsoft Excel version 15.25.1.
Results
Of 39 patients, 37 reached the 3-month follow-up and 2 died within 40 days. The follow-up at 12 months was limited to 34, as three patients died between 3 and 12 months (mean, 7 months). In every case, mortality was due to neoplastic disease. We are continuing to collect results from outpatient visits up to 36 months at present.
Surgical procedures were the following: one-level corpectomy was performed in 8 cervical, 11 thoracic, and 15 lumbar cases (total, 34 cases); two-level corpectomy in 1 cervical and 3 thoracic cases (total, 4 cases); and three-level corpectomy in 1 cervical case.
At the cervical level (10 cases), an anterior approach was used. In five of these (two with metastasis and three with a traumatic complex fracture, where the first surgery failed), a posterior approach was done subsequently.
At the thoracic and lumbar levels (29 cases), the posterior-only approach was performed in 13 cases (8 thoracic and 5 lumbar). A double approach, lateral plus posterior, was performed in 13 cases (6 thoracic and 7 lumbar); of these, in 11 cases, both approaches were performed in a single operating session, and in two cases, the approaches were executed across two sessions. At the lumbar level, in two cases, we performed an anterior approach, finished with an anterior plate in one case and with a posterior fixation in one case. In one lumbar case, we performed an only lateral approach finished with a lateral plate.
In four lumbar cases, the lateral approach was through a mini-open access.
Clinical results
Nurick grades are given in Table 2. Briefly, preoperatively, they were 0 in 24 patients with no deficits or radicular symptoms, 1 in 0 patients, 2 in 2 patients, 3 in 1 patient, 4 in 5 patients, and 5 in 7 patients. Postoperatively (3 months), they were 0 in 24 patients, 1 in 1 patient, 2 in 3 patients, 3 in 3 patients, 4 in 4 patients, and 5 in 2 patients. Comparison of the patients with spinal cord symptoms (Nurick grades from 1 to 5) preoperatively and at 3 months postoperatively revealed a significant improvement (p < 0.01). Among the 24 patients with Nurick grade 0, 14 had no deficit and 10 showed radicular symptoms or deficits preoperatively that resolved completely 3 months after surgery. No patient worsened after surgery.
Patient clinical characteristics and angles: preoperative and 3 and 12 months postoperative.

VAS: visual analog scale.
VAS scores are summarized in Table 2. Briefly, preoperative mean VAS value was 5.4 (±2.8). At 3 and at 12 months, mean VAS values were 1.4 (±1.6) and 1.1 (±1.4), respectively, in both cases, significantly improved compared to the preoperative value (p = 0).
Radiographic results
The mean preoperative regional angulation at the cervical level was +1.8°, at the thoracic level was +18.7°, and at the lumbar level was +5.0°. The mean angle, at 3 and 12 months postoperatively, respectively, was −8.6° and −7.3° at the cervical level, +12.9° and +15.3° at the thoracic level and −7.9° and −6.1° at the lumbar level. Ranges of angulation are given in Table 2.
Fusion rate was assessed by evaluating the plain radiographic images 12 months after surgery. The rate of fusion was 90% and we observed no significant differences among the two types of expandable cages.
Complications
Intra- and perioperative complications occurred in six patients (15.4%). Two of these required reoperation (5.1%), one of whom underwent two reoperations. The first reoperation was required because there was an early mobilization of the cage and the patient was reoperated through the same lateral approach; we repositioned the cage and fixed an additional plate. The second resulted from a deep posterior wound infection that required a revision; we did not remove the hardware and the patient was successfully treated with antibiotics for 12 weeks. In one case, there was an incidental dural tear without consequences. In one case, we intentionally opened the dura to remove the intradural portion of the tumor and a fistula formed later. A second operation was necessary to reinforce the dural closure and stop the leakage. In one case, rhabdomyolysis occurred. In one case, there was an incidental pleural perforation that required the insertion of a chest drain.
Discussion
As a consequence of numerous pathologies, the anterior column of the spine can be compromised and become instable or undergo kyphotic deformity. In these circumstances, it is sometimes necessary to perform a corpectomy. The expandable cage offers a good opportunity to adequately fill the gap and support the spine. In this study, we presented the results of 39 patients treated with expandable cages, confirming that they provide a solid structure that helps correct kyphosis and re-expands the vertebral body. Expandable cages can be used in conjunction with various approaches, including mini-open, and are associated overall with a low rate of complications. The adaptability of the cages to the full set of surgical approaches constitutes further merit of this methodology.
In the past, the material of choice to reconstruct the anterior column after a corpectomy has been structurally autograft or allograft, such as tricortical iliac crest. The integration of the allograft takes more time than the autograft, and there is a potential risk of infection, disease transmission, and graft fracture. 19 In addition to donor site morbidity in the autograft, insufficient biomechanical properties of the graft and secondary kyphosis of the spine 20,21 are to be considered. In the last 20 years, cages of various materials have been brought into use. Subsidence is one problem of these cages because, once inserted, it is necessary to apply compression. The expandable cage represents an innovation among the candidate devices to reconstruct a vertebral body. 4 –7,11,14,15 The main practical advantages are that their insertion, through any approach, is simple, because of the reduced initial height. Furthermore, the in situ expansion allows the correction of the kyphosis and the restoration of the somatic height. In our group of patients, we achieved a significant mean sagittal correction and the reconstruction of the normal local anatomy, with full recovery of the height of the vertebral body. This favorable result is similarly reported by other authors. 4,6
Though the expansion is an advantage overall, the surgeon must be careful when applying the distraction because overdistraction can cause the fracture of the adjacent vertebra, as reported in four cases by Chou et al. 22 According to these authors, one possible explanation is that the force generated by these cages during expansion may result in compression of the end plate. Another possible explanation is that the position of the cage creates a concentrated force applied to one point of the end plate. The third possible explanation is the poor quality of bone. This complication, typically not induced by mesh cages, was not seen in our patients.
Arts and Peul 4 reported a particularly high subsidence rate (42.6%) of the expandable cages. In comparison, other authors found lower subsidence rate: Tarantino et al. 8 reported 11.7%, and Uchida et al. 10 reported 17%. Our observed low rate of subsidence is probably related to the fact that we added posterior instrumentation at the thoracolumbar level in all cases except one and in five cervical cases. Arts and Peul 4 performed an anterior reconstruction without posterior instrumentation in approximately half of the patients. The fusion rate in our study was high, in accordance with the literature. 4,8,13
The anterior cervical approach is routinely used for the herniated disc, a particularly frequent pathology. The anterior approach for the corpectomy must be wider and the incision done along the medial margin of the sternocleidomastoid muscle. After the corpectomy, the end plates are prepared and the cage is easily inserted and expanded under fluoroscopy, obtaining good control over lordosis, as other authors have reported 2,4,8,16 However, as previously noted, there is a potential risk of overdistraction, which is increased in the cervical spine for anatomical reasons. In two cases, the fractures of the adjacent vertebra reported by Chou et al. were at the cervical level. 22 Furthermore, as described in a recent review, 23 the minimum height of the cages could limit their use in cases with the collapsed vertebra, and the amount of hardware in the expansion mechanism may limit the surface area available for fusion. After the insertion of the cage, a plate is commonly utilized to fix the spine. An example is shown in Figure 1. In five cases, we performed a 360° reconstruction, two with metastasis, and three with a traumatic complex fracture, revised after a first surgery failure.

Fifty-six years old woman with neck pain; history of cirrhosis hepatitis C virus (HCV)-related. Corpectomy of C4 and C5, insertion of an expandable cage and anterior plate was performed. The diagnosis was mycobacterial osteomyelitis and was adequately treated. (a) Preoperative X-rays showing the kyphosis at C4–C5. (b) CT sagittal reconstruction showing vertebral body destruction, loss of disk height, and erosion of end plates of C4 and C5. (c) T2 sagittal MRI and (d) T1 sagittal MRI with gadolinium, showing the osteomyelitis at C4–C5 and spinal cord compression. (e) Twelve month postoperative lateral X-rays showing the maintenance of lordosis. (f) T2 sagittal MRI showing the good decompression without signs of recurrence of the disease after the end of treatment. CT: computed tomography; MRI: magnetic resonance imaging.
At the thoracic level, the posterior-only approach was performed in eight cases. At this level, before surgery, angiography should be performed to visualize the origin of the anterior spinal artery. In the case of a tumor, with the same procedure, we can obtain the embolization of the neoplastic vessels. After the angiographic study, we can cut a thoracic root without consequences if we avoid the origin of the anterior spinal artery. The corridor used for the surgical approach is unilateral or bilateral transpedicular and/or lateral extracavitary, which obviates the transcavitary associated risks. Rhizotomy and wide costotransversectomy are necessary to allow the decompression, anterior to the spinal cord, through the midline, until the contralateral pedicle. The wide lateral opening is also necessary to gain the space required to insert the expandable cage. Several retrospective case series have demonstrated the utility of the posterior-only approach for a variety of pathological conditions. 6,9,15,24 The case in Figure 2 is an example of a thoracic posterior-only approach.

Seventy-three years old woman who underwent a nephrectomy for renal cell carcinoma. (a) Two years later, bone scintigraphy showed solitary T11 metastasis. (b) Sagittal CT and (c) coronal CT reconstruction, where the lithic aspect is clear (arrows). (d) T1 sagittal MRI showing the impending spinal cord compression. (e) Lateral and (f) anteroposterior X-rays after corpectomy of T11, insertion of an expandable cage through a posterior-only approach. (g) Sagittal CT and (h) coronal CT reconstruction 1 year after surgery showed that the construct was stable and there were no signs of subsidence. CT: computed tomography; MRI: magnetic resonance imaging.
At the lumbar level, the posterior-only approach is even more challenging compared to the thoracic level because of the depth of the operative field and the need to preserve the nerve roots. At the lumbar level, the posterior-only approach was performed in five of our cases. Shen et al. 5 reported the largest series of cases, all tumors, for which the posterior extracavitary approach for lumbar corpectomy and reconstruction with expandable cages was used. Other authors reported a similar experience. 14,15 The lower lumbar levels, L4 and L5, are the most challenging to resect and reconstruct from a posterior-only approach. We have done a single L4 posterior-only approach. Jandial et al. 25 reported their experience with four cases at L4 or L5. In agreement with those authors, we think that the key to performing this approach is wide dissection and mobilization of the lumbar spinal roots to create a lateral corridor for cage insertion. The expandable cage is inserted obliquely above the root that has to be retracted inferiorly. The implant is then rotated vertically and expanded. The new design of expandable cages facilitates the insertion with narrower inserters and a greater percentage of in situ expansion. 25 Patients who underwent transpedicular corpectomies experienced lower complication and morbidity rates and shorter operative times compared with patients who underwent anterior–posterior multilevel corpectomies. 9 Definitely, the technique from a single posterior approach and insertion of expandable cages offers several advantages over traditional anterior or combined approaches using strut graft or nonexpandable implants. 11,12
A double approach is often demanding and is associated with significant risks. 9,10 Conventional transthoracic and thoracoabdominal approaches are extensive procedures that create a deep surgical field. Furthermore, they require a greater duration of surgery and an opening thoracic or general surgeon and changing the position of the patient for the posterior approach. A lateral and posterior approach was performed in 13 of our cases at the thoracolumbar level; 6 of these were metastases. In spinal metastases, it is fundamental to judge a patient’s life expectancy before considering extensive spinal surgery with instrumentation. 4,26 In two lumbar metastatic cases, we performed an anterior approach. In one case, it was an anterior-only approach combined with the Urologist who performed the nephrectomy. We had the possibility to have a wide transperitoneal exposition that consented to insert the cage and an anterior plate.
Mini-open techniques were introduced in recent years. In our hands, the mini-open techniques for thoracolumbar corpectomy are an extreme lateral procedure. The patient lies in lateral decubitus on the right or left side depending on the anatomy and the pathology. Compared to the standard open approach, the mini-open has the advantage of being extracelomic. It provides a short, direct route to the thoracic and thoracolumbar spine and leaves the pleura and peritoneum intact. Further, it involves low blood loss and a skin incision of only about 5 cm over the vertebra, with limited soft tissue injury. Smaller incisions and less retraction than what is required for traditional approaches result in a reduction of postoperative pain and complications. The spine surgeon does not require the presence of an additional specialist. The disadvantage is the small space and the scarce visualization of the anatomic structures; this can be compensated for by the use of an appropriate retractor and a suitable light source. As its advantages outweigh its disadvantages, we are increasing the number of patients treated with this approach. Agreeing with our positive experience, Scheufler et al. 27 described a series of 38 patients who underwent corpectomy and reconstruction with minimally invasive approaches. They had favorable clinical results at least equal to conventional open surgery, with significant reductions in perioperative morbidity and pain, expedited ambulation, and early discharge from the hospital.
In three cases, we performed a mini-open lateral access, in two cases, associated with a posterior approach, and in one case, we applied a lateral plate. This last case is shown in Figure 3.
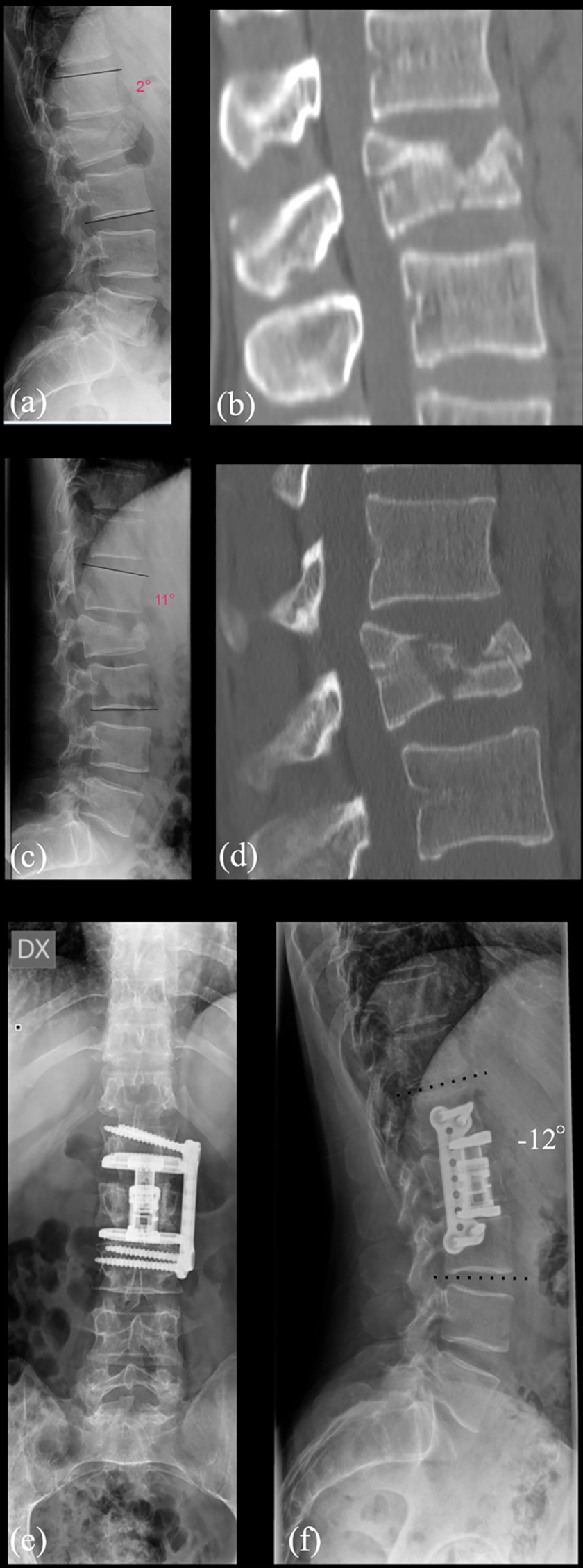
Thirty-nine years old man who fell from a ladder. (a) Lateral X-rays and (b) CT sagittal reconstruction showed a fracture A3 type (AO classification) with 2° of kyphosis. (c) X-rays and (d) CT sagittal reconstruction after 2 months showed that the fracture and the degree of kyphosis worsened. Through a mini-open access, we performed a corpectomy of L3, inserted an expandable cage, and fixed the segment with a lateral plate. (e) Anteroposterior and (f) lateral postoperative X-rays after 1 year showing the maintenance of good lordosis and a solid fusion. CT: computed tomography.
The complication and reoperation rates in our series are low. The single complication related to the hardware was the early mobilization of the cage, detected 2 days after surgery. The patient had a progressive deformity due to a traumatic fracture of L3, which occurred 15 years earlier. She was operated on with a triple approach: posterior release, lateral corpectomy of L3 and insertion of the cage, and posterior stabilization. Notwithstanding circumferential spondylodesis, the cage had mobilized. In our view, mobilization occurred because the surface of the L4 end plate was hard, sclerotic, and slippery, conditions not adequately taken into account in our preparation. We reoperated through the same lombotomic approach, drilled the surface of L4, expanded the cage, and applied a lateral plate. Arts and Peul 4 reported five cases of hardware displacement; they underline that this complication results from a lack of experience in vertebral body reconstruction. The cages are an effective tool, however, for a good outcome the planning, the preparation of the end plates, and the insertion have to be done with attention to all details.
Limitations of our study include its retrospective design and its short follow-up period. Furthermore, the patient population is heterogeneous and various pathologies were treated at different levels. In the future, it would be interesting to compare in a randomized prospective study expandable cages with other forms of reconstruction used in the past, such as mesh cages or traditional bone allograft. The set of patients reported here is still under our care, allowing for a longer follow-up analysis.
Conclusions
Various pathologies can cause instability or deformity of the spine. In some cases, it is necessary to perform a corpectomy, a procedure that is widely used and increasingly common. Expandable cages are crucial tools to reconstruct the spine after a corpectomy.
In this retrospective study of 39 patients, followed for 19 months on average, the use of the expandable cages proved to be advantageous in the cervical, thoracic, and lumbar reconstruction after corpectomy. The cages confer primary stability and the mechanism of expansion allows correction of the kyphosis, regaining the vertebral somatic height. Their use requires careful surgical preparation, both to have the space to insert them and to have the end plates correctly prepared.
The good clinical results with neurological improvement and resolution of pain, the high rate of fusion, and low rates of subsidence, complications, and revision make the expandable cages an attractive tool for replacing the vertebral body.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.